A Chromosome 4q25 Variant is Associated with Atrial Fibrillation Recurrence After Catheter Ablation: A Systematic Review and Meta-Analysis
Pattara Rattanawong1,2, Jirat Chenbhanich3, Wasawat Vutthikraivit4, Pakawat Chongsathidkiet5
1University of Hawaii Internal Medicine Residency Program, Honolulu, HI, USA.2Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand.3Department of Internal Medicine, Metrowest Medical Center, Framingham, MA, USA.4Department of Medicine, Texas Tech University Health Sciences Center, TX, USA.5Department of Pathology, Duke University Medical Center, Durham, NC, USA.
Recent studies suggested that variants on chromosome loci 4q25, 1q21, and 16q22 were associated with atrial fibrillation recurrence after catheter ablation. In this study, we performed a systematic review and meta-analysis to explore the association between variants on chromosome loci 4q25, 1q21, and 16q22 and atrial fibrillation recurrence after catheter ablation
We comprehensively searched the databases of MEDLINE and EMBASE from inception to January 2017. Included studies were published prospective or retrospective cohort and case control studies that compared the risk of atrial fibrillation recurrence after catheter ablation in AF patients with chromosome 4q25, 1q21, and 16q22 variants versus no variants. Single-nucleotide polymorphism rs1906617, rs2106261, rs7193343, rs2200733, rs10033464, rs13376333, and rs6843082 were included in this analysis. Data from each study were combined using the random-effects, generic inverse variance method of DerSimonian and Laird to calculate the risk ratios and 95% confidence intervals
Seven studies from January 2010 to June 2017 involving 3,322 atrial fibrillation patients were included in this meta-analysis. According to the pooled analysis, there was a strong independent association between chromosome 4q25 variant (rs2200733) and the risk of atrial fibrillation recurrence after catheter ablation (risk ratio 1.45 [95% confidence interval 1.15-1.83], P = 0.002). No association was found in other variants
Our meta-analysis demonstrates a statistically significant increased risk of atrial fibrillation recurrence after catheter ablation in 4q25 variant (only in rs2200733) but not in 1q21 or 16q22 variants.
Key Words : Atrial Fibrillation, Catheter Ablation, Chromosome 4q25.
Correspondence to: Pattara Rattanawong
1133 #2007 Waimanust, Honolulu, Hawaii, 96814
Atrial fibrillation (AF) is the most common cardiac arrhythmia treated in clinical practice and affects 10% of the population by 80 years of age. It increases risks of stroke, heart failure, and all-cause mortality[1]. The cornerstones of management include stroke prevention, ventricular rate control, and symptomatic relieve. Catheter ablation is another method to restore and maintain sinus rhythm used widely in selected patients with medically refractory AF. Its efficacy and safety have improved during the last decade, and clinical trials have reported fewer episodes and symptoms after the procedure[2]. Unfortunately, recurrence of AF after catheter ablation is common, ranging from 20% to 60%, and results in repeat of the procedure or re-initiation of antiarrhythmic drugs[2,3].
This variable treatment response, among other clinical heterogeneities, has led physicians explore the molecular basis of AF that may optimize the treatment efficacy and safety. Since Gudbjartsson et al. used genome-wide association study (GWAS) to identify 2 risk variants on chromosome 4q25 (rs2200733 and rs10033464) in 2007, multiple single-nucleotide polymorphisms (SNPs) have been shown to be associated with occurrence of AF[4]. Among these discoveries, the SNPs on chromosome loci 4q25, 1q21, and 16q22 have been replicated in many studies[4-8] and recently demonstrated their potential relations to the AF recurrence after catheter ablation[9-13]. We systematically reviewed current evidence on the association, as well as its significance and characteristics, between common variants on 4q25, 1q21, and 16q22 and AF recurrence after catheter ablation.
Two investigators (JC and WV) independently searched for published studies indexed in MEDLINE and EMBASE databases from inception to January 2017 using a search strategy that included the terms for “atrial fibrillation”, “ablation”, “recurrence”, “4q25”, “1q21”, and “16q22”. Only English language publications were included. A manual search for additional pertinent studies and review articles using references from retrieved articles was also completed.
The eligibility criteria included the following:
(1) Cohort study (prospective or retrospective) reporting incident of recurrent AF
in AF patient after catheter ablation with and without variants on chromosome loci 4q25, 1q21, or 16q22
(2) Relative risk, hazard ratio, odds ratio, incidence ratio, or standardized incidence ratio with 95% confidence intervals or sufficient raw data for the calculation were provided
(3) AF participants without 4q25, 1q21, or 16q22 variants were used as controls
Study eligibility was independently determined by two investigators (PR and PC) and differences were resolved by mutual consensus. Newcastle-Ottawa quality assessment scale was used to evaluate each study in three domains: recruitment and selection of the participants, similarity and comparability between the groups, and ascertainment of the outcome of interest among cohort studies[14].
A standardized data collection form
was used to obtain the following information from each study: title of study, name of first author, year of
publication, country of origin, number of participants, demographic data, ablation techniques, outcomes of interest (variants and AF recurrence),
and average duration of follow-up. To ascertain the accuracy, all investigators independently performed this data extractionprocess. Any data discrepancy was resolved by referring back to the original articles.
We performed a meta-analysis of the included cohort studies using a random-effects model. The extracted studies were excluded from the analysis if they did not present an outcome in each intervention group or did not have enough information required for continuous data comparison. We pooled the point estimates from each study using the generic inverse-variance method of Der Simonian and Laird[15]. The heterogeneity of effect size estimates across these studies was quantified using the I2 statistic and Q statistic. For the Q statistic, substantial heterogeneity was defined as p<0.10. The I2 statistic ranges in value from 0 to 100% (I2<25%, low heterogeneity; I2=25%–50%, moderate heterogeneity; and I2>50%, substantial heterogeneity)[16]. A sensitivity analysis was performed to assess the influence of the individual studies on the overall results by omitting one study at a time. Publication bias was assessed using funnel plot and Egger’s regression test[17] (p<0.05 was considered significant). All data analyses were performed using the Stata SE 14.1 software from StataCorp LP.
Description of Included Studies
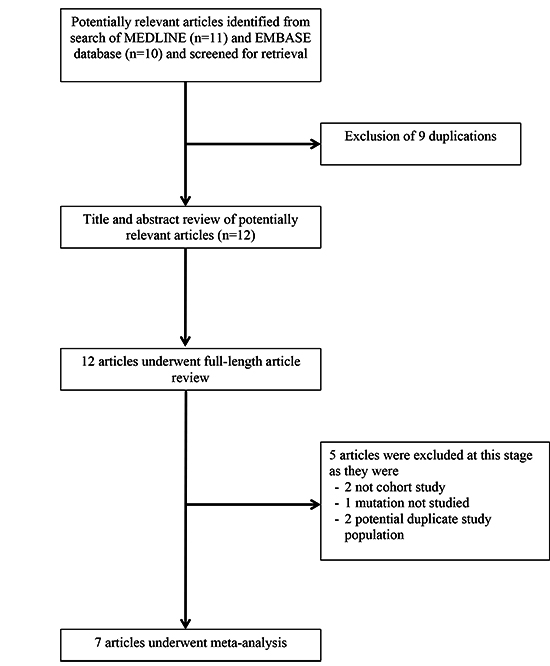
Our search strategy yielded 21 potentially relevant articles (11 articles from EMBASE and 10 articles from MEDLINE). After exclusion of 9 duplicated articles, 12 articles underwent title and abstract review. Five articles were excluded at this stage since they were not cohort studies, did not report the outcome of interest (AF recurrence) or were not conducted in patients with AF underwent catheter ablation, leaving 7 articles for full-length article review. Therefore, 6 prospective cohort studies, and 1 case-control studies of 3,322 AF patient underwent catheter ablation were included in this meta-analysis. [Figure 1]outlines the search and literature review process. The clinical characteristics and summary of included studies are described in [Table 1]
Table 1. Characteristics of Included Studies
| First author |
Husser et al. |
Shoemaker et al. |
Choi et al. |
Kiliszek et al. |
Chen et al. |
Zhao et al. |
Miyazaki et al. |
| Country |
Germany |
USA/Germany |
South Korean |
Poland |
China |
China |
Japan |
| Study design |
Prospective cohort |
Prospective cohorts from 3 centers |
Prospective cohort |
Prospective cohort |
Prospective cohort |
Case control |
Prospective cohort |
| Year of publication |
2010 |
2015 |
2015 |
2016 |
2016 |
2017 |
2017 |
| Study subject |
German patients who underwent left atrial catheter ablation for drug-refractory paroxysmal or persistent AF |
Patients underwent de novo AF ablation between 2008 and 2012 at Vanderbilt University, the Heart Center Leipzig, and Massachusetts General
Hospital |
All AF patients underwent radiofrequency catheter ablation from Yonsei AF Ablation Cohort registry |
Paroxysmal or persistent AF patients at Medical University of Warsaw |
Drug-refractory Chinese Han AF patients at the First Affiliated Hospital |
Chinese Han patients admitted to department of cardiology from July 2011 to August 2013 at Shanghai First People's Hospital |
Japanese patient whom underwent cryoballoon ablation from July 2014 to January 2016 for paroxysmal atrial fibrillation |
| Exclusion criteria |
Presence of left atrial thrombus |
N/A |
Permanent AF refractory to electrical cardioversion, valvular disease, structural heart disease other than left ventricular hypertrophy, prior AF
ablation. |
Hyperthyroidism, significant mitral valve disease, left atrial dimension over 5.5 cm, severe diseases with life expectancy below 1 year |
Familial AF, hyperthyroidism, valvular heart disease, cardiomyopathy, left atrial thrombus, other severe diseases with life expectancy below 1 year
|
Familial AF, lone AF, recent MI (6 months or less), cardiac surgery (30 days or less), NYHA class III or IV, thyroid, renal, or lung dysfunction AF due
to trauma surgery, or acute medical illness |
N/A |
| Number of subjects (%M, mean age±SD) |
195 (73%, 56±12) |
991 from 3 centers: 245 (71%, 61±9.63); 659 (67%, 60±10.4]); 87 (82%, 57±9.63) |
1068 (74.6%, 57.5±10.9) |
238 (66.80%, 55±10.4 |
235 (73.7%, 59.41) |
438 (52.12%, 63.75 ± 15.93) |
157 (72.6%, 64±10.8) |
| Paroxysmal AF |
78% |
58.8% |
67.9% |
N/A |
56.7% |
N/A |
100% |
| Hypertension |
N/A |
72.3% |
47.8% |
58.4% |
38.7% |
N/A |
48.4% |
| Diabetes |
N/A |
N/A |
13.0% |
7.6% |
20.0% |
N/A |
N/A3(4%) |
| Ablation technique |
Radiofrequency pulmonary vein isolation (with linear ablation in persistent AF) |
Radiofrequency pulmonary vein isolation (with linear ablation based on operator discretion) |
Radiofrequency pulmonary vein isolation (with linear ablation based on operator discretion) |
Radiofrequency pulmonary vein isolation |
Radiofrequency pulmonary vein isolation (with linear or complex fractionated ablation based on operator discretion) |
Radiofrequency pulmonary vein isolation (with linear ablation in unsuccessful pulmonary vein isolation) |
Cryoballoon pulmonary vein isolation |
| Variants : and SNP(s) investigated for the recurrence risk (and its closest gene) |
4q25:rs2200733 (PITX2), rs10033464 (PITX2) |
4q25:rs2200733 (PITX2), rs10033464 (PITX2),1q21:rs13376333 (KCNN3), 16q22:rs7193343 (ZFHX3) |
4q25:rs6843082 (PITX2), rs2200733 (PITX2), 1q21:rs13376333 (KCNN3)16q22:rs2106261 (ZFHX3) |
4q25:rs2200733 (PITX2), rs10033464 (PITX2), rs17570669 (PITX2), rs3853445 (PITX2), rs6838973 (PITX2), 1q21:rs13376333 (KCNN3), 16q22:rs7193343 (ZFHX3) |
4q25:rs2200733 (PITX2), 16q22:rs2106261 (ZFHX3) |
4q25:rs2200733 (PITX2) |
4q25:rs1906617(PITX2) |
| Endpoints: early recurrence of AF |
Within 7 days |
N/A |
Within the 3-month post-ablation |
Within the 6-month post-ablation |
N/A |
N/A |
After the 3-month post-ablation blanking period |
| Endpoints: late recurrence of AF |
Between 3 and 6 months |
After the 12 months post-ablation |
After the 3-month post-ablation |
After the 6-month post-ablation |
After the 3-month post-ablation blanking period |
After the 3-month post-ablation blanking period |
N/A |
| Mean follow-up |
6 months |
12 months |
18.3±13.9 months |
45 months |
12 months |
N/A [0-48 months] |
12 months |
| Conclusions by authors |
rs2200733 and rs10033464, modulate are associated with increased rate of AF recurrence after ablation |
rs2200733, but not rs10033464, rs13376333, or rs7193343, is associated with increased rate of AF recurrence after ablation |
rs6843082, rs2200733, and rs2106261 were associated with AF |
rs2200733 is associated with increased rate of AF recurrence after pulmonary vein isolation in short-term (6 months) follow-up. |
rs2200733 is associated with AF recurrence after ablation, potentially by influencing the size of the RA and superior PVs |
rs2200733 was associated with AF and was associated with recurrence after ablation |
rs1906617 was associated with AF and was associated with recurrence after cryoballoon ablation |
* Recurrence is defined as any episode of non-sinus atrial tachyarrhythmia (atrial tachycardia, atrial flutter, or AF) lasting greater than 30 seconds
Table 2. Newcastle–Ottawa scales of the included studies
| Study |
|
Selection |
|
|
Comparability |
|
Outcome |
|
total |
|
Representativeness |
Selection of Thenonexposed Cohort |
Ascertainment |
End point not present at start |
Confounding |
Assesment of Outcome |
Follow up duration |
Adequacy follow-up |
|
| Husser et al. |
* |
* |
* |
* |
** |
* |
|
* |
8 |
| Shoemaker et al. |
* |
* |
* |
* |
** |
* |
* |
* |
9 |
| Choi et al. |
* |
* |
* |
* |
** |
* |
* |
* |
9 |
| Kiliszek et al. |
|
* |
* |
* |
* |
* |
* |
* |
7 |
| Chen et al. |
* |
* |
* |
* |
** |
* |
* |
* |
9 |
| Zhao et al. |
|
* |
* |
* |
* |
* |
* |
* |
8 |
| Miyazaki et al. |
* |
* |
* |
* |
** |
|
* |
* |
8 |
Figure 1. Search methodology and selection process
Quality Assessment of Included Studies
Newcastle–Ottawa scales of the included studies are described in the supplement [Table 1]. The Newcastle-Ottawa scale uses a star system (0 to 9) to evaluate included studies on 3 domains: selection, comparability, and outcomes. Higher scores represent higher study quality. Intra-study risks of bias of included studies are also described in the supplement [Table 2]
Table 3. Intra-study risks of bias of included studies
| Study |
Clear definition of study population |
Clear definition of outcomes and assessment |
Independent assessment of outcomes? (e.g. by third party) |
Sufficient Follow-up duration? |
Selective loss during Follow-up? |
Limitations identified? |
| Husser et al. |
yes |
yes |
no |
no |
no |
yes |
| Shoemaker et al. |
yes |
yes |
no |
yes |
no |
yes |
| Choi et al. |
yes |
yes |
no |
yes |
no |
yes |
| Kiliszek et al. |
no |
yes |
no |
yes |
no |
yes |
| Chen et al. |
yes |
yes |
no |
yes |
no |
yes |
| Zhao et al. |
no |
yes |
no |
yes |
no |
yes |
| Miyazaki et al. |
yes |
no |
no |
yes |
no |
yes |
There were 7 studies from January 2010 to June 2017 involving 3,322 atrial fibrillation patients were included in this meta-analysis. Seven SNPs among 4q25, 1q21, or 16q22 variants were reported in previous AF ablation studies. Four SNPs including rs2200733, rs10033464, rs6843082, and rs1906617 were reported in 4q25 variants. One SNPs, rs13376333, was reported in 1q21 variants. Two SNPs including rs2106261and rs2106261 were reported in 16q22 variants
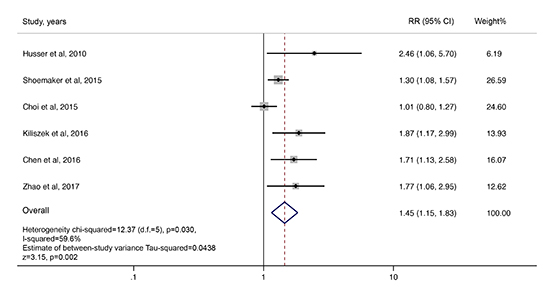
For rs2200733, 6 studies from January 2010 to June 2017 were included in meta-analysis [9-13,18]. Five out of six studies reported statistical significant increased risk of AF recurrence in patent with SNP rs2200733[9-13]. According to the pooled analysis, there is a strong independent association between chromosome 4q25 variant and AF recurrence after catheter ablation (RR 1.45 [95% CI 1.15-1.83], p = 0.002) with high heterogeneity (I2=59.6%) [Figure 2].
Figure 2. Forest plot of the included studies assessing the association between recurrence of atrial fibrillation after catheter ablation and variant rs2200733 on 4q25.
Three studies were included for meta-analysis for rs10033464 [10,12,13] which reveals no association with AF recurrence (RR 1.11 [95% CI 0.64-1.94], p = 0.703) with high heterogeneity (I2=66.2%) [Figure 3A]. We did not performed meta-analysis in rs6843082 and rs1906617 since only one study of each provided available data. For rs6843082, previous report revealed no association with AF recurrence (RR 0.84 [95% CI 0.61-1.15], p = 0.280)[18]. However, for rs1906617, recent study reported significant association with AF recurrence (RR 2.44 [95% CI 1.06-5.61], p = 0.035)[19].
Figure 3A Forest plot of the included studies assessing the association between recurrence of atrial fibrillation after catheter ablation and variant rs10033464 on 4q25, B) rs13376333 on 1q21, C) rs2106261 on 16q22, and D) rs7193343 on 16q22.

For rs13376333, 3 studies from January 2010 to June 2017 were included in meta-analysis [12,13,18]. All of 3 studies reported no association between patients with SNP rs13376333 and risk of AF recurrence. According to the pooled analysis, there is no independent association between rs13376333 in chromosome 1q21 variant and atrial fibrillation recurrence after catheter ablation (RR 0.86 [95% CI 0.71-1.05], p = 0.142) with low heterogeneity (I2=0%) [Figure 3B].
For rs2106261, 2 studies from January 2010 to June 2017 were included in meta-analysis [9,18]. All of two studies reported no association between patients with SNP rs2106261 and risk of AF recurrence. According to the pooled analysis, there is no independent association between rs2106261 in chromosome 16q22 variant and atrial fibrillation recurrence after catheter ablation (RR 0.92 [95% CI 0.74-1.14], p = 0.434) with low heterogeneity (I2=21.2%) [Figure 3C].
For rs7193343, two studies from January 2010 to June 2017 were included in meta-analysis[12,13]. All of two studies reported no significant association between patients with SNP rs7193343 and risk of AF recurrence. According to the pooled analysis, there is no independent association between rs7193343 in chromosome 16q22 variant and atrial fibrillation recurrence after catheter ablation (RR 0.90 [95% CI 0.73-1.11], p = 0.331) with low heterogeneity (I2=0%) [Figure 3D].
To assess the stability of the results of the meta-analysis, we conducted a sensitivity analysis by excluding one study at a time. We used a sequential exclusion strategy, as described by Patsopoulos and colleagues, to examine whether overall estimates were influenced by the substantial heterogeneity observed[20]. None of the results was significantly altered, indicating that our results were robust
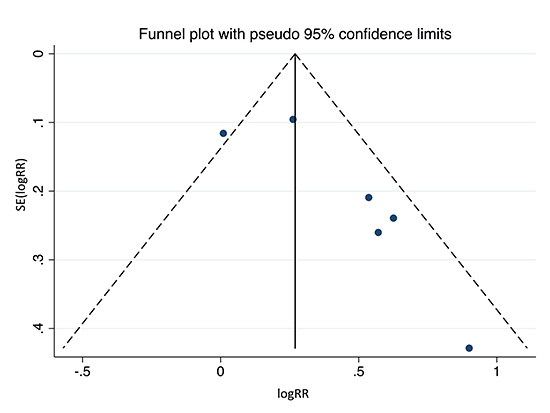
To investigate potential publication bias in rs2200733, we examined the contour-enhanced funnel plot of the included studies in assessing change in log OR of AF recurrence [Figure 4]. The vertical axis represents study size (standard error) while the horizontal axis represents effect size (log odds ratio). From this plot, distribution of studies on both sides of the mean is asymmetrical. The Egger's test was not significant in rs2200733 (p = 0.060), and rs10033464 (p = 0.279) which confirmed no small study bias. However, small study bias was observed in rs13376333 (p = 0.007)
Figure 4 Funnel plot of recurrence of atrial fibrillation after catheter ablation and variant rs2200733 on 4q25. Circles represent observed published studies
Our analysis found that the variant rs2200733 on 4q25 significantly associated with AF recurrence after catheter ablation (RR 1.45 [95% CI 1.15-1.83], p = 0.002), whereas no association was found among variants rs10033464 from 4q25, rs13376333 from 1q21, and rs7193343 and rs2106261 from 16q22. We did not analyze SNPs that presented only in single publication; among these non-analyzed SNPs, only rs1906617 from 4q25 increased a risk of AF recurrence, with a relative risk of 2.44, in the report by Miyazaki et al.[19].
Genetics of AF has been emerging in recent years. Researchers from Framingham Heart Study initially found that parental history could double the risk of AF in offspring[21]. Variants in genes encoding cardiac potassium and sodium channel complexes and gap junction proteins were found to cause a familial form of AF [22]. In contrast to these high-penetrant rare variants, the low-penetrant polymorphisms found via GWAS tend to interact with environment and result in the more common non-familial phenotype. The variant rs2200733, not surprisingly, has been studied the most and strongly associated with AF occurrence, with an odd ratio of 1.89, according to the recent meta-analysis of 10,546 subjects with AF[23]. Presence of rs2200733 also implicated in cardioembolic stroke[24] and postoperative AF after coronary artery bypass graft surgery [25,26]. Our study is the first meta-analysis to evaluate this variant, along with others, and its risk of AF recurrence after catheter ablation. We believe that only a variant with strong molecular signals (e.g. rs2200733) will affect AF recurrence after catheter ablation, whereas the others (e.g. those in 1q21 and 16q22 loci) will not[13]. Nonetheless, the precise mechanism how they affect AF recurrence is yet to be determined.
The paired-like homeodomain transcription factor 2 (PITX2) gene is located closest to variant rs2200733, and the hypotheses underlying the AF susceptibility of 4q25 loci lies, probably, in this gene[4]. PITX2 expressed in left atrium of mice and humans, and both over- and underexpression of the gene are associated with AF[27]. In mice, its haploinsufficiency resulted in ectopic automaticity in the left atrium and thus predisposed to atrial arrhythmia[28]. Moreover, PITX2 promotes cardiac left-right asymmetry and development of pulmonary vein sleeves, which are isolated during AF ablation procedure–referred to pulmonary vein isolation [13,27,29]. No known gene was identified in the linkage disequilibrium block containing variant rs2200733[4]; thus, the variants at this location may indirectly be a marker of unidentified mechanisms independent of PITX2, or, on the other hand, may have an unknown direct relation with the gene [10].
Chen et al have additionally demonstrated that, when compared to AF patients with wild-type allele, carriers of rs2200733 had larger superior pulmonary veins, which are more common AF-driving ectopic loci than the inferior pulmonary veins[9]. This might explain the propensity of AF recurrence, and shows how genetic data promisingly suggests a different ablation method in this patient population.
Among the early researchers who showed how the variant potentially implicated clinical practice on AF recurrence, Shoemaker et al. found that the presence of rs2200733 risk allele in patients having left atrial diameter larger than 5cm–which usually used as a cutoff for AF ablation eligibility–increased the risk of AF recurrence from 40% to 87.5% [30]. In the multivariate analysis, the risk allele predicted a 24% shorter recurrence-free time with a survival time ratio of 0.76 (CI 0.6-0.95)[30]; this is crucial since patients with earlier recurrences tend to have less sporadic episodes and respond poorer to anti-arrhythmic drugs and repeat ablation[31]. We know that established risk factors of AF recurrence after catheter ablation include hypertension, obesity, sleep-disordered breathing, metabolic syndrome, left atrial dilatation, and longstanding persistent AF [3,32], and the decision to pursue ablation procedure depends on type of AF, left atrial size, symptom severity, systolic dysfunction, estimated risk of complications, and patient preference[2]. Thus, adding rs2200733 to the list may help physicians predict outcomes and risk stratify patients before performing the procedure–reducing patients and physicians’ frustration and creating the most efficacious strategy for this invasive, high-cost, success-limited procedure. Accordingly, a large-scale study exploring its accuracy and cost-effectiveness, especially with the rapidly decreasing cost of genomic sequencing, are required.
Our study is not without limitations. Different study populations and designs were included and thus might introduce potential sources of heterogeneity. We also did not demonstrate independent predictors of recurrance in AF such as age, sex, diabetes, and hypertension because of insufficient data from included studies to perform meta-analysis in these subgroups. Theses factors might introduce potential sources of heterogeneity as well. Some heterogeneity exists among studies. Nonetheless, we used sensitivity analysis methods in the random-effects model and found no difference of the imputed risk ratio and its 95% confidence interval.
We systematically reviewed variants from chromosome loci 4q25, 1q21, and 16q22, and demonstrated that only rs2200733 from 4q25 confers an increased risk of AF recurrence after catheter ablation. The most plausible mechanism is related to the closest gene, PITX2; however, its molecular pathophysiology is yet elusive and more studies are warranted to explore how these variants impact the clinical course and prognosis of AF. Incorporation of this variant as a pre-procedural risk factor to predict an outcome of catheter ablation is an attractive paradigm in personalized AF management in the near future.






