Same-Day Versus Next-Day Discharge Strategies for Left Atrial Ablation Procedures: A Parallel, Intra-Institutional Comparison of Safety and Feasibility
Matthew T. Brown1, Mary M.Pelling1, Soroosh Kiani1, Faisal M. Merchant2, Mikhael F. El-Chami2, Angel R. Leon2, Stacy Westerman1, Anand Shah1, Donna Wise1, Michael S. Lloyd1
1Emory University Hospital, Atlanta, GA.2Emory University Hospital Midtown, Atlanta, GA.
Head-to-head comparative data for the postoperative care of patients undergoing left atrial ablation procedures are lacking.
We sought to investigate complication and readmission rates between patients undergoing same-day (SD) or next-day (ND) discharges for ablative procedures in the left atrium, primarily atrial fibrillation (AF).
Two electrophysiology centers simultaneously perform left atrial ablations with differing discharge strategies. We identified all patients who underwent left atrial ablation from August 2017 to August 2019 (n = 409) undergoing either SD (n = 210) or ND (n = 199) discharge protocols. We analyzed any clinical events that resulted in procedural abortion, extended hospitalization, or readmission within 72 hours.
The primary endpoint of complication and readmission rate was similar between SD and ND discharge (14.3% vs 12.6%, p = 0.665). Rates of complications categorized as major (2.4% vs 3.0%, p = 0. 776) and minor (11.9% vs 9.5%, p = 0.524) were also similar.Multivariable regression modeling revealed no significant correlation between discharge strategy and complication/readmission occurrence (OR 1.565 [0.754 – 3.248], p = 0.23), but a positive association of hypertension and procedure duration (OR 3.428 [1.436 – 8.184], p = 0.006) and (OR 1.01 [1 – 1.019], p = 0.046) respectively.
Left atrial ablation complication and readmission rates were similar between SD and ND discharge practices. Hypertension and procedural duration were associated with increased complication rates irrespective of discharge strategy. These data, which represent the first side-by-side comparison of discharge strategy, suggests same-day discharge is safe and feasible for left atrial ablation procedures.
Key Words : Atrial fibrillation, Left atrial, Ablation, Complications, Hospitalization, Discharge strategy.
Michael S. Lloyd, 1364 Clifton Rd NE, Suite F424, Atlanta GA 30322
Catheter ablation for atrial fibrillation (AF) has established superiorityto medical therapy for the long-term maintenance of sinus rhythm and improvement in quality of life.Catheter ablation for AF and left atrial flutter (LAFL)is emerging as the most common ablation procedure performed in the U.S.with exponential growth observed in the past decade.3, 4 Despite the high frequency, there is little consensus on the postoperative management for these procedures. The standard remains inpatient admission and overnight monitoring. However, many practices have begun exploring alternative discharge strategies including outpatient AF ablation. 5While it would be more efficient and cost-effective to adopt a same-day discharge strategy for these types of procedures, concerns due to longer procedure times, left atrial lesion delivery, and heparinization have rendered the appropriate discharge strategy controversial.
Table 1. Demographic, Clinical, and Procedural Characteristic Comparison by Discharge Strategy
|
Same-Day (210) |
Next-Day (199) |
P |
| Age |
64.7 (11.1) |
63.14 (10.9) |
0.273 |
| Gender (F) |
31.9% (67) |
32.7% (65) |
0.916 |
| Body Mass Index |
29.06 (5.27) |
31.11 (6.3) |
<0.001 |
| Arrhythmia Type |
|
|
0.019 |
| Permanent Afib |
0.5% (1) |
0% (0) |
|
| Persistent Afib |
31.9% (67) |
45.7% (91) |
|
| Paroxysmal Afib |
61% (128) |
48.7% (97) |
|
| Other |
6.7% (14) |
5.5% (11) |
|
| Hypertension |
56.7% (119) |
67.3% (134) |
0.032 |
| Hyperlipidemia |
38.6% (81) |
40.7% (81) |
0.686 |
| Structural (Valvular, Congenital) |
18.1% (38) |
13.6% (27) |
0.226 |
| Congestive Heart Failure |
14.8% (31) |
26.6% (53) |
0.003 |
| Ejection Fraction (%) |
54.46 (8.35) |
50.97 (11.12) |
0.003 |
| Coronary Artery Disease |
11% (23) |
15.6% (31) |
0.19 |
| Diabetes Mellitus |
10.5% (22) |
19.6% (39) |
0.012 |
| Cerebrovascular Accident |
11.4% (24) |
7.5% (15) |
0.238 |
| Chronic Kidney/End-stage Renal Disease |
7.1% (15) |
5.5% (11) |
0.548 |
| Obstructive Sleep Apnea |
21.4% (45) |
29.6% (59) |
0.069 |
| Chronic Obstructive Pulmonary Disease |
2.4% (5) |
4% (8) |
0.406 |
| Prior Ablation |
34.3% (72) |
31.2% (62) |
0.528 |
| Prior Direct Current Cardioversion |
47.1% (99) |
54.0% (107) |
0.167 |
| Ablation Type |
|
|
<0.001 |
| PVI Only |
23.7% (49) |
33.7% (67) |
|
| PVI + |
63.3% (131) |
46.2% (92) |
|
| Non-PVI |
10.6% (22) |
6.5% (13) |
|
| Convergent |
0.5% (1) |
13.1% (26) |
|
| Other |
1.9% (4) |
0.5% (1) |
|
| Sedation Type |
|
|
<0.001 |
| Moderate Sedation |
78.8% (164) |
55.1% (109) |
|
| General Anesthesia |
21.2% (44) |
44.9% (89) |
|
| Hemostasis Type |
|
|
<0.001 |
| Manual |
68.6% (144) |
97.5% (194) |
|
| Device |
31.4% (66) |
2.5% (5) |
|
| Procedure Duration (hours:min) |
2:14 (0:36) |
2:09 (0:31) |
0.181 |
| Ablation Duration (min) |
41.4 (40.7) |
40.3 (27.9) |
0.404 |
| Cryo Lesions [#] |
8 (8, 8) |
8 (7, 9) |
0.025 |
| RF time (min) |
13.7 (13) |
22.4 (23) |
0.062 |
| RF Lesions [#] |
18.5 (9, 34.25) |
16 (7.75, 30.25) |
0.145 |
| Power [watts] |
59.5 (18.719) |
56.84 (23.369) |
0.788 |
Abbreviations: Non-PVI=ablation excluding pulmonary vein isolation; PVI=pulmonary vein isolation; PVI+=pulmonary vein isolation plus additional lesion set; RF=radiofrequency
There have been limited published data regarding same-day discharge for AF ablation procedures – with the majority consisting of historical case control studies or simple descriptive studies of clinical experience. Prior studies have either used non-randomized patient preference 6, historical control after institutional discharge strategy implementation7, 8, or observational longitudinal descriptions 9-11.
With two high-volume electrophysiology centers simultaneously performing left atrial ablation differing primarily in post-procedure discharge strategies, we found a unique opportunity to compare outcomes between same-day (SD) and next-day (ND) post-ablation discharge with little variability to ablation strategy, operator experience, or patient factors. We analyzed acute outcomes of AF ablation and other left atrial ablation procedures in terms of complications and readmission rates to assess,in a temporally-parallelformat, the safety and feasibility of SD versus ND discharge strategy.
Consecutive patients undergoing AF, LAFL, or left atrial tachycardia ablationsinvolving transseptal puncture at two high-volume centers within the Emory Healthcare systembetween August 2017 and August 2019 were analyzed. Discharge strategy consisted of general practice guidelines within each hospital and were defined as: 1. ND, consisting of routine overnight stay in a telemetry floor with subsequent discharge the following morning after clinical assessment and groin check; and 2. SD, consisting of discharge after 2-4 hours of bedrest, clinical exam, and groin check. Ablation procedures followed accepted practice guidelines and consisted of predominantly cryo-ablation for paroxysmal AF andradiofrequency (RF) for persistent AF. Ultrasound either by intra-cardiac echo (ICE) or trans-esophageal echo (TEE) was used in the majority of cases and general anesthesia was used according to physician discretion.To specifically compare discharge practices, analysis excluded those who deviated from the institutional discharge strategy, but a separate intention to treat analysis was performed as well. The study was approved by the EmoryInstitutional Review Board.
All routine demographic data including gender, age, and body mass index as well as routine medical history was evaluated. Specificbaseline arrhythmia characteristics were also noted, includingAF subtype (paroxysmal, persistent, or permanent) and history of cardioversion or prior ablation. Procedural characteristics were also analyzed including anesthesia type, ablation type and location, procedure duration, and hemostasis method use.
The primary endpoint was defined as any clinical event that resulted in procedural abortion, a longer hospital stay than anticipated at either center, or readmission within 72 hours. Individual complications were categorized by type and classified as major or minor based on their clinical significance. Major complications included stroke, tamponade, phrenic nerve palsy, sinus node dysfunction, and esophageal perforation. Minor complications included access site issues, pericarditis, simple effusion, unstable labs or vitals, incomplete studies, and a few others.
Differences between groups were subjected to the Student’s t test or Wilcoxon rank sum test for normally and non-normally distributed continuous data, respectively, or the Fisher’s exact test for categorical variables. A 2-tailed P <.05 was considered significant. Continuous data are presented as mean ± standard deviation. We also performed multivariable regression to identify independent predictors of complications among the cohortthat included discharge strategy in an a priori fashion, as well as variables found to be associated with complications in univariateanalysis (p<0.05) as covariates. All analyses were performed using IBM SPSS ver. 26 (2019; IBM SPSS Statistics for Macintosh, Version 26.0. Armonk, NY: IBM Corp).
A total of 507 patients underwent left atrial ablation involving transseptal puncture between the two centers. 257 patients were ablated under the SD discharge protocol and of these patients182 dischargedSD according to planwhile 75 deviated from the discharge strategy. 250 patients were ablated underthe NDdischarge protocol and 196 discharged asplanned after overnight monitoringwhile 54 deviated from the discharge strategy.There were a total of 98 patients excluded from the following data analysis due to deviations from the protocol not due to complication (e.g. patient preference, time of day, transportation). Therefore, a total of 409 patients undergoing atrial ablation were included for comparison of 210 SD discharge patients and 199 ND discharge patients [Figure 1]
Figure 1. Schematic Outline of Patient Classification According to Pre-determined Discharge Protocol and Actuality.
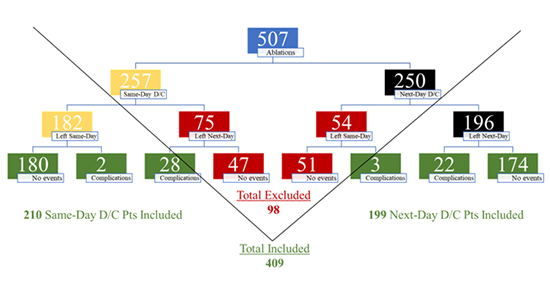
507 total ablations (blue) were performed between sites with 182 out of 257 anticipated same-day (yellow) and 196 out of 250 anticipated next-day(black) discharges proceeding according to plan. 75 patients in the same-day group and 54 in the next-day group did not discharge according to plan (red), some uneventful and others experiencing complications. Patients with deviation from anticipated discharge protocol and no events were excluded from additional analysis (red) while those discharging according to anticipated strategy plus those that deviated and experienced a complication were further analyzed (green). Abbreviations: D/C = Discharge, Pts = Patients.
Clinical and Procedural Characteristics between Discharge Strategy Cohorts
The average age and gender between the 210 SD and 199 ND discharge patients were similar as were rates of most medical comorbidities and prior ablations or cardioversions. A few statistically significant differences were found between cohorts with ND patients having higher body mass index (31.11% vs 29.06%, p = <0.001) and rates of hypertension (67.3% vs. 56.7%, p = 0.032), diabetes (19.6% vs. 10.5%, p = 0.012), and congestive heart failure (CHF) (26.6% vs 14.8%, p = 0.003) associated with lower ejection fractions (50.97 vs. 54.46, p = 0.003) than their SD counterparts. While AF accounted for over 90% of arrhythmia type in either group, SD patients had higher rates of paroxysmal (61% vs. 48.7%) and lower rates of persistent (31.9% vs. 45.7%) AF which contributed to a significant difference (p = 0.019). Overall procedure and ablation duration were similar between discharge strategies as were RF time, lesion number, and power. SD patients were more likely to undergo pulmonary vein isolation (PVI) plus additional lesion sets (63.3% vs. 46.2%) under moderate sedation (78.8% vs. 55.1%) with aid of a hemostasis device (31.4% vs. 2.5%). ND patients underwent more convergent ablations in combination with cardiothoracic surgery (13.1% vs. 0.5%) and lone PVI procedures (33.7% vs. 23.7%) that more often involved general anesthesia (44.9% vs. 21.2%) and manual pressure hemostasis (97.5% vs. 68.6%).
Univariate Predictors of Complication and Readmission
Severalunivariate predictors of complications and readmission were identified in the cohort. As seen in [Table 2], patients with higher body mass index (31.49 vs 29.83, p = 0.040), rates of hypertension (76.36% vs 59.6%, p = 0.017), and CHF (30.91% vs. 18.93%, p = 0.049) were more likely to have complications or be readmitted within 72 hours. Procedure duration was significantly longer in those with complications (2:26 +/- 0:45 vs. 2:10 +/- 0:32, p = 0.25), in addition,ablation type (p = 0.020) and sedation type (p = 0.042) varied significantly. A higher percentage of patients with complications underwent convergent (15.1% vs 5.4%) and non-PVI (13.2% vs. 7.9%)ablations while a lower percentage with complications underwentPVI only (17% vs. 30.3%) procedures. General anesthesia (45.28% vs. 30.88%) was more commonly used among patients with complications than moderate sedation (54.72% vs. 69.12%). All other factors such as average age, gender breakdown, medical comorbidities, and technical procedural aspectswere similar between those with and without experiencing complications.
Table 2. Demographic, Clinical, and Procedural Characteristic Comparison by Complication Occurrence
|
Complication (55) |
No Complication (354) |
P |
| Age |
66.16 (10.39) |
63.57 (11.11) |
0.109 |
| Gender (F) |
43.64% (24) |
30.51% (108) |
0.063 |
| Body Mass Index |
31.49 (6.62) |
29.83 (5.73) |
0.040 |
| Arrhythmia Type |
|
|
0.483 |
| Permanent Afib |
0% (0) |
0.28% (1) |
|
| Persistent Afib |
47.27% (26) |
37.29% (132) |
|
| Paroxysmal Afib |
49.09% (27) |
55.93% (198) |
|
| Other |
3.64% (2) |
6.5% (23) |
|
| Hypertension |
76.36% (42) |
59.6% (211) |
0.017 |
| Hyperlipidemia |
43.64% (24) |
38.98% (138) |
0.554 |
| Structural (Valvular, Congenital) |
21.82% (12) |
14.97% (53) |
0.232 |
| Congestive Heart Failure |
30.91% (17) |
18.93% (67) |
0.049 |
| Ejection Fraction (%) |
51.82 (11.91) |
52.85 (9.65) |
0.397 |
| Coronary Artery Disease |
5.45% (3) |
14.45% (51) |
0.085 |
| Diabetes Mellitus |
21.82% (12) |
13.84% (49) |
0.152 |
| Cerebrovascular Accident |
9.09% (5) |
9.6% (34) |
1 |
| Chronic Kidney/End-stage Renal Disease |
12.73% (7) |
5.37% (19) |
0.066 |
| Obstructive Sleep Apnea |
21.82% (12) |
25.99% (92) |
0.618 |
| Chronic Obstructive Pulmonary Disease |
5.45% (3) |
2.82% (10) |
0.406 |
| Prior Ablation |
36.4% (20) |
32.2% (114) |
0.540 |
| Prior Direct Current Cardioversion |
52.7% (29) |
50.1% (177) |
0.773 |
| Ablation Type |
|
|
0.020 |
| PVI Only |
17% (9) |
30.3% (107) |
|
| PVI + |
52.8% (28) |
55.2% (195) |
|
| Non-PVI |
13.2% (7) |
7.9% (28) |
|
| Convergent |
15.1% (8) |
5.4% (19) |
|
| Other |
1.9% (1) |
1.1% (4) |
|
| Sedation Type |
|
|
0.042 |
| Moderate Sedation |
54.72% (29) |
69.12% (244) |
|
| General Anesthesia |
45.28% (24) |
30.88% (109) |
|
| Hemostasis Type |
|
|
0.088 |
| Manual |
90.91% (50) |
81.36% (288) |
|
| Device |
9.09% (5) |
18.64% (66) |
|
| Procedure Duration (hours:min) |
2:26 (0:45) |
2:10 (0:32) |
0.025 |
| Ablation Duration (min) |
47.43 (37.17) |
39.3 (27.08) |
0.541 |
| Cryo Lesions [#] |
8 (7, 9) |
8 (8, 9) |
0.303 |
| RF time (min) |
21.81 (17.35) |
20.7 (22.47) |
0.484 |
| RF Lesions [#] |
22.5 (12, 30.25) |
17 (9, 34) |
0.206 |
| Power [watts] |
53.23 (19.77) |
58.56 (22.13) |
0.198 |
Results of the univariate predictors of complications during left atrial ablations. Univariate predictors identified were body mass index, hypertension, congestive heart failure, ablation type, sedation type, and procedure duration. Abbreviations: Non-PVI=ablation excluding pulmonary vein isolation; PVI=pulmonary vein isolation; PVI+=pulmonary vein isolation plus additional lesion set; RF=radiofrequency
Overall Complication and Readmission Rates
Among the 409 patients that analyzed, 55 (13.5%) experienced complication or readmission within 72 hours. Complications were classified asminor (n=44, 10.8%))and major (n=11, 2.7%) events. No statistically significant differences were found between either discharge strategywhen comparing readmission, major, or minor complication groups. [Table 3]Major complications included 4 (0.98%) cases of cardiac tamponade involving drain placement, 3 (0.73%) cases of persistent phrenic nerve palsy at follow-up, 2 (0.45%) post-procedure thromboembolic strokes causing mild deficits, and 2 (0.45%) cases of sinus node dysfunction requiring either temporary or permanent pacemaker insertion. Minor complications were more prevalent with the leading problems involving unstable vitals/labs and access site difficulties. A total of 19 (4.7%) cases necessitated additional monitoring or medical intervention for hemodynamicinstability such as hypotension or tachycardia or laboratory abnormality such as anemia or acute kidney injury. Furthermore, 12 (2.93%) patients experienced bleeding or mild hematoma/bruising from their access site post-operatively. There were no cases of pseudoaneurysmformation or retroperitoneal bleeding. Additional minor complications involved rates < 1% for incomplete procedures due to findings of atrial thrombus or difficulty with transseptal access, clinically significant pericarditis or small pericardial effusions, and other problems such as uncontrolled pain or urinary retention prompting additional monitoring.
Table 3. Overall Complication Rates of Transseptal Ablations Stratified by Discharge Policy
|
Total(n = 409) |
Same-Day(n = 210) |
Next-Day(n = 199) |
P-level |
| Overall Complication Rate |
13.45% (55) |
14.3% (30) |
12.6% (25) |
0.665 |
| Major |
2.69% (11) |
2.38% (5) |
3.01% (6) |
0.776 |
| Cardiac Tamponade |
0.98% (4) |
0.95% (2) |
1.01% (2) |
|
| Phrenic Nerve Palsy |
0.73% (3) |
0.48% (1) |
1.01% (2) |
|
| Cerebrovascular Accident |
0.45% (2) |
0.95% (2) |
0% (0) |
|
| Sinus Node Dysfunction |
0.45% (2) |
0% (0) |
1.01% (2) |
|
| Esophageal Perforation |
0% (0) |
0% (0) |
0% (0) |
|
| Minor |
10.76% (44) |
11.90% (25) |
9.55% (19) |
0.524 |
| Unstable Vitals or Labs |
4.65% (19) |
5.71% (12) |
3.52% (7) |
|
| Access Site Comp. |
2.93% (12) |
3.33% (7) |
2.51% (5) |
|
| Anatomic Diff. / Thrombus |
0.98% (4) |
0.95% (2) |
1.01% (2) |
|
| Significant Pericarditis |
0.73% (3) |
0.95% (2) |
0.50% (1) |
|
| Simple Effusion |
0.45% (2) |
0.48% (1) |
0.50% (1) |
|
| Other (pain, urinary retention) |
0.98% (4) |
0.48% (1) |
1.51% (3) |
|
Complications rates among the same-day and next-day cohorts. Both the major and minor complication rates were found to be similar among the groups. Abbreviations: Comp.=Complication; Diff.=difficulty
Of all patients, 2 were readmitted within 72 hours of same-day discharge (0.95%) - onefor chest pain found to be pericarditis and another for syncope deemed a vasovagal event although with findings of a small pericardial effusion. A separate intention-to-treat analysis including those patients deviating from the hospital-defined discharge strategy was also performed for overall complication/readmission rates and yielded no statistically significant differences (p = 0.546).
Multivariable Regression Analysis
Multivariable regression modeling was performed to further evaluate the relationship ofbaseline clinical or procedural characteristics found to be significant predictors of complications with univariate analysis. Discharge strategy was also included in this analysis. Results are outlined in [Table 4]with univariate predictorsof CHF, body mass index,ablation type, and sedationtype not found to be associated with complications in multivariate analysis. The presence of hypertension (odds ratio of 3.428 [1.436 - 8.184])and procedure duration (odds ratio of 1.01 [1 – 1.019]) was significantly associated with increased rates of complication in our regression model. Finally, our regression model showed no effect of discharge strategyon complication rate(odds ratio at 1.565 [0.754 – 3.248)].
Table 4. Multivariable model of predictors of complications for Atrial Fibrillation Ablation.
|
Beta Coefficient |
Odds Ratio (95% CI) |
P-Level |
| Discharge Strategy (Same-Day vs. Next-Day) |
0.448 |
1.565 (0.754 - 3.248) |
0.230 |
| Congestive Heart Failure |
0.514 |
1.671 (0.809 - 3.453) |
0.165 |
| Hypertension |
1.232 |
3.428 (1.436 - 8.184) |
0.006 |
| Body Mass Index |
0.015 |
1.015 (0.957 - 1.076) |
0.619 |
| Ablation Type (Compared to PVI only) |
|
|
0.380 |
| PVI+ |
0.488 |
1.628 (0.644 - 4.118) |
0.303 |
| Non-PVI |
0.852 |
2.344 (0.594 - 9.249) |
0.224 |
| Convergent |
1.295 |
3.652 (0.979 - 13.625) |
0.054 |
| Other* |
-18.269 |
0 (0 - .) |
0.999 |
| Sedation Type (General vs Conscious) |
0.543 |
1.721 (0.807 - 3.672) |
0.160 |
| Procedure Duration (per min) |
0.01 |
1.01 (1 - 1.019) |
0.046 |
Results of the multivariable regression model of predictors of complication after atrial fibrillation ablation. Independent predictors in the model include hypertension (HTN), as well as procedure duration. *Because there were vert few patients in this group, the odds ratio and confidence interval are less meaningful. Abbreviations: CI=confidence interval; Non-PVI=ablation excluding pulmonary vein isolation; PVI=pulmonary vein isolation; PVI+=pulmonary vein isolation plus additional lesion set
Our analysis using an intra-institutional comparison of SD versus ND discharge strategy represents a unique and more robust form of analyzing complication and readmission rates for patients undergoing left atrial ablation procedures. Our data indicate two important findings. First, there was no significant difference in complication rates or readmission ratesamong SD or ND discharge strategy when used as a general hospital-based approach. We feel this adds strength to the limited but growing evidence in favor of SD discharges for most AF and left atrial ablative procedures. Comparable rates of major complications are reported in large reviews12-16 and, while there is limited data from the U.S., other countries’ analyses introduced above reveal a lack of significant difference in these rates when patients are kept overnight. When examining a variable such as time of discharge, the importance of selection bias cannot be overstated, as those who do well would tend to have physicians choose to send the patient home sooner, and those in whom there was clinical concern would be expected to be monitored longer. This is why we chose to exclude those who deviated from the general discharge policy at the two comparator clinical sites. Importantly, when we chose to include the deviations from each site as an intention to treat, we continued to observe a non-significant difference in complication rate.
Secondly, multivariate analysis showed hypertension and procedure duration, not discharge strategy as inepedentpredictors of our primary endpoint. There were unavoidable differences in our patient demographic between the SD and ND hospitals that warrant mention and could confound our findings. Namely, a higher incidence of persistent AF, CHF, general anesthesia, and convergent/hybrid surgical procedures were observed in the ND cohort. Of these, procedure type, CHF, and sedation type were associated in univariate analysis with higher complication. However, multivariate analysis including these variables only identified hypertension and duration of procedure as significant predictors of complication. Gender has been identified as a risk marker for complication in other studies not examining discharge strategy for AF.17-20 In our analysis we found a trend (P=0.06) toward higher univariate risk for complication, but this variable did not meet clinical significance. Other risk markers as outlined in [Table 2] are congruent with prior published studies.21
Complication and readmission rates among two high-volume medical centers within the same healthcare system adhering to either SD or ND discharge strategy do not significantly differ for left atrial ablation procedures. These data support a growing body of evidence in favor of SD discharge for this common procedure and the need for a prospective randomized trial.






