Stepwise Approach to the Different Parts of Vasovagal Syncope in a Patient Undergoing Cardioneuro Ablation
Tolga Aksu1, Tumer Erdem Guler1, Serdar Bozyel1, Kivanc Yalin2
1Associated Professor of Cardiology, Kocaeli Derince Education and Research Hospital, Department of Cardiology, Kocaeli/Turkey.2Usak University Hospital, Department of Cardiology, Usak/Turkey.
A 30-year-old man underwent ganglionated plexi ablation due to cardioinhibitory type vasovagal syncope with asystole. After asymptomatic period of 15-month following the procedure, the patient experienced 2 new syncope episodes. Tilt test demonstrated vasodepressor response without significant bradycardia. Following the onset of midodrine therapy, the patient was asymptomatic for 1 year and tilt test demonstrate normal response.
Key Words : Ganglionated Plexi, Parasympathetic, Syncope, Atrial Fibrillation.
Correspondence to: Tolga Aksu, Derince Education and Research Hospital Department of Cardiology, Derince Kocaeli/Turkey.
Syncope is a clinical condition characterized with transient loss of consciousness due to cerebral hypoperfusion[1]. In the younger population, the vast majority of cases are associated with vasovagal syncope (VVS). Although there are still some debates about pathophysiological background of VVS, reflex mechanism consisting of sympathetic nervous system inhibition and subsequent excessive parasympathetic activity seems to be the most plausible mechanism[2]. Demonstration of an increase on sinus rate or atrioventricular conduction properties following various radiofrequency ablation procedures has led to the introduction of several new ideas such that attenuation of parasympathetic innervation might be achieved by endocardial radiofrequency catheter ablation and be used in the treatment of conditions associated with parasympathetic hyperactivity[3-4]. The technique is simply named as cardioneuroablation (CNA). Although effectivity of the technique was well documented in patients with cardioinhibitory type VVS, there is no clear clinical data about the patients with ongoing syncope after CNA. We aimed to define our approach in a patient with ongoing syncope complaints after CNA.
A 30-year-old male had been suffering from recurrent episodes of syncope. On his medical recording, 25 months ago, he was admitted to our center with similar complaints despite of treatment with midodorine hydrochloride (5 mg/day). He had 6 syncope episodes which occurred with upright posture and prodromal symptoms in preceding 6 months accompanied by type 2B response according to the New Vasovagal Syncope International Study (VASIS) classification on Head-up tilt table test (HUT)[Figure 1][5]. The frequency of the syncopal spells was twice a week, but intensity and frequency of episodes considerably increased recently. The patient was offered pacemaker implant in another institution, however, was reluctant to accept and asked for a second opinion at our center. Before performing ablation, conventional treatment modalities consisting of optimal fluid intake and counter-pressure maneuvers were attempted. Within the scope of our previous study, the patient underwent CNA to attenuate the cardio-inhibitory component of VVS 24 months ago[Figure 2][6]. During the procedure, the three-dimensional geometry of both atria was created by using the electro-anatomical mapping system (EnSite Velocity, St Jude Medical, Sylmar, CA, USA). As defined by Pachon et al[7], the compact and the fibrillar atrial myocardium were detected. The potentials showing complex fractionated pattern with ≥ 4 deflections at filter settings of 300-500 Hz were considered as fibrillar atrial myocardium and tagged. Continuous high frequency stimulation (HFS) was then delivered to the presumed ganglionated plexi sites with a frequency of 20 Hz, amplitude of 0.1-1mA, and pulse duration of 1-10 ms for 5 seconds per each site. Subsequently, HFS was started by applying progressive voltage increases until a parasympathetic response was induced. The sites showing a parasympathetic response were assigned as ablation target. RF energy was delivered with power of up to 35 W and a maximum temperature of 43°C with a cooling rate of 18 mL/min until elimination (<0,1 mV) of targeted electrograms and positive parasympathetic responses. As a routine protocol of our previous study, to check the real denervation achievement, atropine response, sinoatrial and atrioventricular nodes functions were evaluated before and after the procedure.
Figure 1. Hemodynamic parameters during head-up tilt table test were obtained before cardioneuroablation procedure.
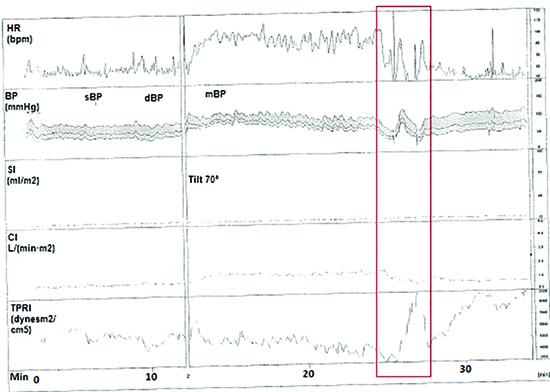
Heart rate decreased with 6 seconds asystole in the passive phase and the patient lost consciousness transiently (red rectangle, cardioinhibitory type). Although there was a slight decrease in blood pressure, it did not fall below the baseline values. The test was performed under midodrine treatment. BP, blood pressure; CI, cardiac index (The CI was computed as stroke volume which was calculated from the impedance signal X heart rate; DBP, diastolic blood pressure; HR, heart rate; mBP, mean blood pressure; SBP, systolic blood pressure; SI, stroke index (The SI was calculated by dividing stroke volume by body surface area); TPRI, total peripheral resistance index (The TPRI was calculated as mean blood pressure divided by CI).
Figure 2. Electroanatomical mapping view and demonstration of vagal response to high frequency stimulation
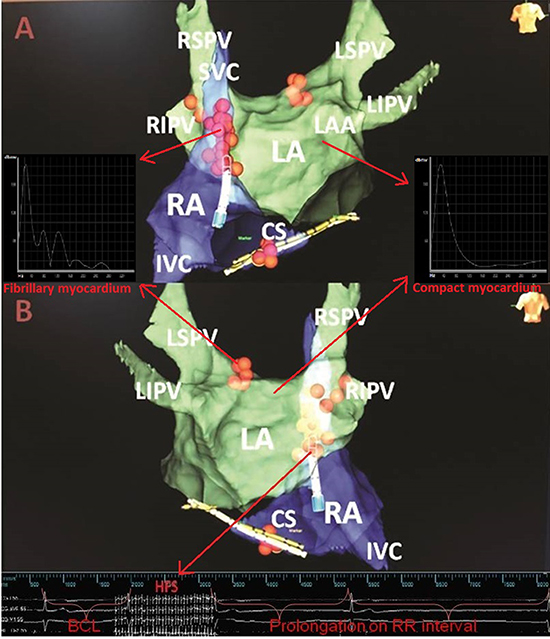
(A) Antero-posterior view, (B) Postero-anterior view. Red spheres indicate ablation lesions. During high frequency stimulation on the right inferior pulmonary vein, significant prolongation on RR interval is seen in surface ECG and intracardiac electrograms. In fibrillary myocardium, the incursion of the nervous fibres into the myocardium causes anisotropic conduction interrupting the cell connections. This anisotropic conduction detected as heterogeneous segmented spectrum with frequencies deviated to the right. In compact myocardium, due to well connected cells, spectral analysis demonstrates a homogeneous and unipolar spectrum. Images of high frequency stimulation and spectral (Fast Fourier Transform) analysis were modified from our previous work (Ref. 13). BCL, basal cycle length; CS, coronary sinus; HFS, high frequency stimulation; IVC, inferior vena cava; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; RSPV, right superior pulmonary vein; SVC, superior vena cava.
Throughout 15 months following the procedure, he had been attending our outpatient clinic, he had no attacks of syncope without any medications. Ten months ago, the patient was admitted again to our center after two syncope episodes within 1 month. After resting in a supine position for 20 minutes, the patient was tilted at an angle of 70 degrees for 40 minutes. Neither syncope nor hypotension was induced. A sublingual glyceryl trinitrate was applied with the tilt table at 70 degrees, his systolic blood pressure dropped from 100 to 30 mmHg without bradycardia or asystole[Figure 3]. Within a few seconds, overt syncope occurred and the tilt table was immediately returned to a horizontal position.
Figure 3. Hemodynamic parameters during head-up tilt table test were obtained 15 months after cardioneuroablation procedure
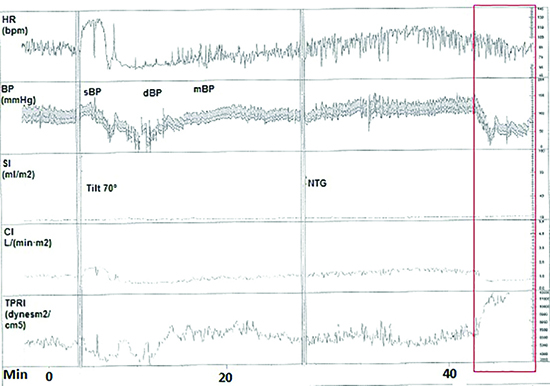
Blood pressure decreased in the sublingual glyceryl trinitrate phase, and the patient lost consciousness transiently (red rectangle, vasodepressor type) BP, blood pressure; CI, cardiac index (The CI was computed as stroke volume which was calculated from the impedance signal X heart rate; DBP, diastolic blood pressure; HR, heart rate; mBP, mean blood pressure; SBP, systolic blood pressure; SI, stroke index (The SI was calculated by dividing stroke volume by body surface area); TPRI, total peripheral resistance index (The TPRI was calculated as mean blood pressure divided by CI).
Given the vasodepressor response during HUT, we speculated that the episodes were partially due to vasodilatation and that CNA was not strong enough to prevent his syncope. Therefore, we attempted administration midodrine hydrochloride. The tilt table test was performed again with the patient taking midodrine hydrochloride 5 mg/day and syncope was not induced even by the administration of sublingual nitroglycerin[Figure 4]. He was discharged with this medication. At the end of 9 months follow-up period, he has had no attacks of syncope.
Figure 4 Hemodynamic parameters during head-up tilt table test were obtained 2 months after the restarting of midodrine treatment
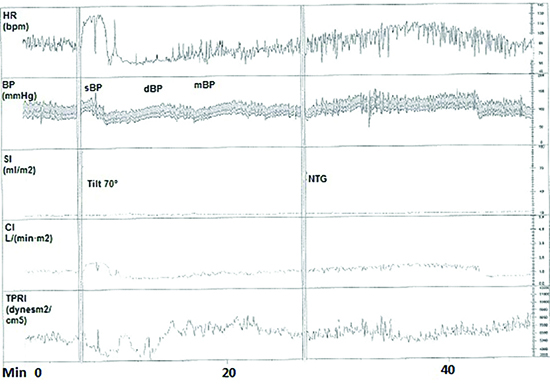
The patient felt mild chest discomfort; however, heat rate and blood pressure did not decrease in the passive and sublingual glyceryl trinitrate phases (Normal response). BP, blood pressure; CI, cardiac index (The CI was computed as stroke volume which was calculated from the impedance signal X heart rate; DBP, diastolic blood pressure; HR, heart rate; mBP, mean blood pressure; SBP, systolic blood pressure; SI, stroke index (The SI was calculated by dividing stroke volume by body surface area); TPRI, total peripheral resistance index (The TPRI was calculated as mean blood pressure divided by CI).
We have described a case of resolution of recurrent syncope after sequential interventional and medical treatments for VVS. Pathophysiological nature of VVS was detected by well interpreted HUTs. The present case demonstrated that the major component of syncope or the response to HUT might change according to applied treatments. A similar phenomenon may be one of the reasons of ongoing syncope episodes despite normal functioning pacemaker. Thus, we considered that a well interpreted HUT may provide valuable clinical information in following patients who undergo CNA and change our approach.
Previous reports demonstrated that CNA might be an alternative to permanent pacemaker in well selected patients with VVS[6,8]. Although short-term results after CNA are promising, ratio of positive response may be up to 23% of patients at post-procedural HUTs [8]. Since the type of positive response is not clearly indicated in the studies, there is no clinical data on what to do next. As it demonstrated in the present case, syncope or prodromal symptoms may recur after CNA with a different mechanism.
To explain the different types of VVS, different degrees of activation or depression of the autonomous nervous system are be used: (1) cardioinhibitory VVS is associated with an activation of the parasympathetic nervous system which provokes bradycardia; (2) vasodepressor VVS primarily originates from the acute loss of sympathetic stimulation which causes a drop of blood pressure; (3) Nevertheless in most cases a combined mechanism is seen and called as mixed VVS. In the present case, pre-procedural HUT demonstrated a decline in blood pressure was accompanied by a fall in heart rate would suggest a mixed type VVS. Despite this suggestion, the nature of the spontaneous syncope
could not be fully explained. It is well known that a HUT solely based diagnose might be deceivable. For evaluation of the syncope mechanism, Holter or Loop recordings could add valuable clinical data, especially when syncope episodes have been so frequently reported. If we could demonstrate a collapse in the absence of marked bradycardia, it would have provided some basis for our consideration.
Wieling et al[9] reviewed the classic literature related to the mechanisms underlying VVS and concluded that reduction in cardiac output through bradycardia, rather than vasodilation, may be the primary cause of the hypotension of VVS. The idea that CNA may prevent the development of bradycardia or asystole due to parasympathetic hyperactivity and be effective in resolving cardioinhibitory VVS is based on these general assumptions.
In our case, the contribution of the vasodepressor component was probably not detected in the pre-procedural HUT due to the fact that the increase in parasympathetic activity was more pronounced. However, after successful vagal denervation, the vasodepressor response became obvious. Kim et al[10] recently assessed the determinants of VVS during glyceryl trinitrate -stimulated HUT and demonstrated that syncope might be related with systemic vascular resistance rather than cardiac output. In our case, HUT was demonstrated glyceryl trinitrate -stimulated vasodepressor response after CNA. So, we prescribed midodrine hydrochloride to deal with vasodepressor response which is a potent peripherally acting alfa 1 agonist. In our previous published article, we performed the technique in some mixed cases. Although syncope episodes and asystole are no longer seen, there was a significant hypotension response during HUTs. Therefore, our case might be an additional clue to demonstrate that CNA may present not such adequate clinical results in mixed or vasodepressor syncope as those observed in purely cardioinhibitory syncope.
In our case, the passive phase of HUT lasted longer than 30 minutes. Protocols with shorter passive phases, followed by sensitization with nitrate or isoproterenol, are linked with greater specificity than protocols with a more prolonged passive phase[11]. That may raise the question whether HUT response after denervation was a true vasodepression or simply a false positive. In the present work, continuous HFS was applied to detect localization of ganglionated plexus. However, using an atrioventricular nodal functional response to continuous HFS to locate ganglionated plexi may not be sufficient to locate the sites as those observed with synchronized HFS[12]. Thirdly, one of the important issues related CNA is to check, as a hard end point, the real denervation achievement. Although we evaluated immediate autonomic functions, it requires a method for extracardiac vagal effect evaluation at the end of procedure[13]. Lastly, there is no primary scientific evidence of direct association between vagal response during clinical syncopal situation and parasympathetic response site in the HFS application during electrophysiological study.
Parasympathetic hyperactivity based bradycardia or sympathetic withdrawal guided vasodilatation contributes varying grades to VVS. Although there are serious concerns about sensitivity and specificity, a well interpreted HUT might be used to reveal partial contribution of different components in VVS. The concept of CNA may offer an alternative way to treat recurrent cardioinhibitory VVS cases. Further studies are warranted to investigate the utility of CNA in these conditions.






