The Role of Implantable Cardiac Monitors in Atrial Fibrillation Management
Giuseppe Ciconte1, Daniele Giacopelli2, Carlo Pappone1
1Department of Arrhythmology, IRCCS Policlinico San Donato, University of Milan, San Donato Milanese (MI), Italy.2Biotronik Italia, Clinical Research, Vimodrone (MI), Italy.
Continuous heart rhythm monitoring using implantable cardiac monitors (ICMs) for atrial fibrillation (AF) management is steadily increasing in current clinical practice, even in the absence of an established indication provided by international guidelines. The increasing use of such devices is mainly associated with recent technological improvements including miniaturization, easier implant procedures, and remote monitoring, all of which make this strategy continuously more appealing and promising. For these and other reasons, ICMs have been proven to be a safe and highly effective tool for detecting AF episodes. However, ICMs are not the best option for every patient, as limitations exist. Therefore, it is imperative to weigh the possible benefits against the potential limitations of using these devices when deciding individualized patient care.
Key Words : Atrial fibrillation, Continuous monitoring, Implantable Cardiac Monitor, Loop recorder, Subcutaneous electrocardiogram.
Correspondence to: Giuseppe Ciconte, MD Department of Arrhythmology IRCCS Policlinico San Donato, University of Milan Piazza E. Malan 1, 20097 San Donato Milanese, Milano, Italy Phone: +39 0252774260; Fax: +39 0252774306 e-mail: g.ciconte@gmail.com
Atrial fibrillation (AF) is the most common cardiac arrhythmia, and it is associated with a reduced quality of life and an increased number of adverse outcomes such as stroke, heart failure, increased number of hospitalizations, and mortality[1]-[4]. Therefore, an early diagnosis of this arrhythmia is crucial in order to adopt the most appropriate treatment strategy. Cardiac implantable electronic devices (CIEDs) and sub-cutaneous cardiac monitors (ICMs) seem to be a very effective tool to achieve this objective, rather than intermittent monitoring[5]-[9]. In fact, the use of ICMs is continuously growing in everyday clinical practice, together with recent technological improvements including miniaturization, easier implant procedures, and remote monitoring. However, due to the lack of sufficient trial-based evidence[6], AF is currently not considered an established indication for ICM adoption.
The aim of this review is first to evaluate and potentially expand the contemporary role of ICMs in clinical AF management and then to describe the technical issues eventually affecting the efficacy of this monitoring system.
Rhythm monitoring in AF patients
The rate control therapy for AF management does not require any sophisticated tools to monitor its efficacy. In contrast, ECG monitoring is needed when “rhythm control” approach is applied. However, an accurate detection and quantification of AF episodes might be very challenging. It is well established that there is a poor correlation between symptoms and arrhythmic events in AF patients[6]. Also, silent AF frequently occurs, as a high incidence of episodes without any symptoms has been detected using CIEDs[7],[8]. The TRENDS trial was a prospective, multicenter observational study that enrolled 2486 patients after CIED implantation (pacemakers or defibrillators with an implanted atrial lead). Subclinical (asymptomatic) atrial tachyarrhythmias (TAs) were diagnosed in 45% of 1988 patients without a documented history of prior AF[7].
Table 1. Recommendations, advantages and limitations for the use of ICM in atrial fibrillation management
| Indications for ICM use in AF management |
| Determination of the efficacy of rhythm control therapy |
| Assessment of freedom from AF after catheter ablation |
| Detection of AF in patients with cryptogenetic stroke |
| Advantages |
| Avoidance of unreliable subjective evaluation of the effect of any therapy |
| Overcoming the limits of intermittent AF monitoring system |
| Shortening of the time needed to obtain relevant information |
| Limitations |
| Lack of clinical evidence of the benefits of ICM to guide medical and device therapy |
| Presence of false positive arrhythmic episodes |
| Invasive procedure and risk of local complications |
In the ASSERT trial there was a substantial incidence of subclinical AFs in a cohort of 2580 patients without previous evidence of AF and in whom there was implanted a pacemaker or implantable cardioverter defibrillator (ICD) containing an atrial lead. These arrhythmias were detected in 10.1% of the patients within the first 3 months after implantation and at least once in 34.7% of the patients during a mean follow-up period of 2.5 years[8].
While the prevalence of AF can be underestimated, especially in asymptomatic patients, its incidence can also be overestimated as some patients may incorrectly attribute extra beats or sinus tachycardia to AF. In patients with permanent pacemakers for brady-tachy syndrome, the sensitivity and positive predictive value of symptoms to detect AF were 19% and 21%, respectively[9]. Other confounding variables may be antiarrhythmic drugs and catheter ablation. Although catheter ablation may affect the progression of the disease by reducing the rate of relapses[10], it can also change the perception of arrhythmia recurrences. In particular, asymptomatic episodes may occur and significantly increase after catheter ablation[11],[12].
Table 2. Atrial fibrillation detection performance of ICM
|
Hindricks G. et al.30
(Reveal XT, Medtronic) |
Ciconte G. et al.31 (Bio-
Monitor, Biotronik SE&Co.) |
Nolker G. et al.32 (Confirm
DM2102, St. Jude Medical) |
| Episode sensitivity |
88.2% |
95.4% |
94.0% |
| Episode specificity |
- |
- |
96.7% |
Episode positive
predictive value |
73.5% |
76.3% |
59.1% |
Episode negative
predictive value |
- |
- |
88.3% |
| Subject sensitivity |
96.1% |
100% |
100% |
| Subject specificity |
85.4% |
67.0% |
85.7% |
Subject positive
predictive value |
79.3% |
83.0% |
64.0% |
Subject negative
predictive value |
97.4% |
100% |
100% |
Heart rhythm monitoring can be performed with continuous or intermittent strategies. The continuous approach is essentially based on implantable devices (pacemakers, ICD, ICM), whereas the intermittent approach includes ECG, Holter (24h to 7 days) and event recorders. It is not surprising that studies have demonstrated that arrhythmia detection improves with increasing intensity of monitoring[13]. When compared with CIEDs, intermittent ECG monitoring demonstrated a significantly lower sensitivity (31–71%) and negative predictive value (21–39%) for identification of patients with any atrial TAs[13]. Charitos et al. reported similar results, using the rhythm histories from 647 patients with implanted devices[14]. For this reason, intermittent rhythm monitoring techniques are unreliable estimators of the true AF burden as well as subjective evaluation based upon putative symptoms. In this scenario, where the CIEDs are considered as the gold standard for AF monitoring, the ICM offers a valuable tool of continuous rhythm monitoring in patients without indication for permanent pacemaker or ICD.
Clinical Indications for ICM
AF detection for the Assessment of Arrhythmic Burden
According to current guidelines, one of the primary indications of AF catheter ablation is to reduce arrhythmia-related symptoms and to improve quality of life[5]. However, arrhythmia monitoring is an essential component of clinical trials aimed at assessing the outcomes of ablation procedures. In fact, silent AF was found to be associated with morbidity and mortality. Therefore, there is general agreement that continuous arrhythmia monitoring should be incorporated in all clinical trials designed to assess the efficacy of AF catheter ablation tools and techniques[5].
The ABACUS study compared the ICM to conventional monitoring (30-day transtelephonic monitors at discharge and after 5 months) in patients undergoing AF ablation, showing that ICM can detect more arrhythmias, despite the presence of false detections[10]. After AF ablation, 44 patients received ICMs and conventional monitoring. Over the first 6 months after ablation, conventional monitoring revealed AF in 7 patients (18%) and ICM confirmed AF in all of them. In an additional 11 patients (29%), no AF was seen by standard monitoring but was accurately detected by ICM[15]. Pedrote et al. estimated the AF burden before and after catheter ablation with an ICM, establishing the true efficacy of the technology. This study showed a complete freedom from AF after circumferential pulmonary vein isolation in 57% of patients and a significant worsening in AF burden in 17% of patients[16]. In a randomized trial by Pokushalov E. and colleagues, arrhythmia recurrences detected by ICM guided the decision for an early repeat catheter ablation, showing that patients with AF recurrences after index procedure are likely to benefit from a redo ablation, especially when AF is triggered by atrial premature contractions or atrial flutter/tachycardias (AFl, ATs)[17]. Continuous monitoring with ICM was also used in other studies after surgical AF ablation[18] and coronary artery bypass grafting (CABG)[19]. In both these studies, the ICM was considered an essential tool to correctly quantify the AF incidence. In addition, patients with typical AFl without documentation of AF episodes represent another cohort of interest. In fact, Mittal S and colleagues documented, using ICM monitoring, that 55% of AFl patients experienced AF episodes after cavo-tricuspid isthmus ablation during a mean follow-up of 382±218 days. This study proved the important role of ICM for long-term AF surveillance also in this subset population[20].
There is no evidence that ICM could guide the use of anticoagulant drugs, and discontinuation of oral anticoagulation (OAC) is not recommended in post-ablation patients with elevated CHADS2 or CHA2DS2-VASc scores. However, patients undergoing AF ablation, particularly in younger cohorts, are usually highly motivated by the potential OAC interruption in case of procedural success. One possible way to minimize the risk of thromboembolism in these patients could be continuous rhythm monitoring[5]. A recent study by Zuern et al. showed that rhythm monitoring by ICM in patients who have stopped OAC after catheter ablation of AF seems to be a safe and promising approach. The entire cohort of patients was composed by 63 individuals with a CHADS2 score ranging between 1-3 undergoing ablation. At 1.3 years after ablation, about two-thirds of patients were off OAC in the absence of cerebrovascular events[21]. However, despite the promising and attractive results, the relatively small sample size and the short follow-up interval prevent one from drawing robust conclusions. Recently, the REACT.COM pilot study established the feasibility of ICM-guided intermittent anticoagulation with novel anticoagulants (NOAC) in patients with a low thromboembolic risk profile. After AF ablation, 59 patients with a mean CHADS2 score of 1.3±0.5 underwent continuous rhythm assessment with ICM. Use of rapid onset novel oral anticoagulants (NOACs) allow for targeted anticoagulation only around an AF episode. Over 466±131 mean days of follow-up there were 35 AF episodes longer than 1 hour in 18 (31%) patients, resulting in a total time on NOAC of 1,472 days. This represents a 94% reduction in the time on NOAC compared to chronic anticoagulation. There were three traumatic bleeds (all on aspirin), three potential transient ischemic attacks (all on aspirin with CHADS2 score of 1), and no strokes or deaths[22]. A randomized trial of ICM-guided versus chronic NOAC (REACT-AF) is ongoing in a moderate-risk AF population with nonpermanent AF[22].
The use of ICM has class IIa indication in case of undocumented palpitations[6]. This statement is based on the results of the RUP study, in which 50 subjects with unexplained palpitations were randomly assigned to receive a ICM or a conventional monitoring strategy[23]. A diagnosis was obtained in 5 patients in the conventional strategy group, and in 19 subjects in the ICM group (21% vs. 73%, p < 0.001). Among all documented supraventricular tachycardias, AF was the most frequent finding with an incidence of 23% in the ICM group as compared to only 4% in the conventional group.
ICM in cryptogenic stroke patients
Cryptogenic stroke (CS), or brain infarction from an unknown cause, accounts for 20 to 40% of ischemic stroke[24]. AF can be the underlying cause of CSs, as recent trials have observed a significant relationship between device-detected atrial arrhythmias and stroke risk[7],[8]. Detection of silent AF is crucial, as it changes the standard of care from antiplatelet to anticoagulation therapy[25]. Two recent prospective randomized studies, CRYSTAL AF and EMBRACE, demonstrated that a marked improvement in AF detection yielded more comprehensive arrhythmia monitoring strategies compared to standard care in subjects with CS[26],[27]. In particular, the CRYSTAL AF trial used ICM in the continuous monitoring arm, detecting AF episodes in 12.4% of patients during a 12 month period of time as compared to 2% in the control group. Cumulative AF detection rates in the ICM arm increased progressively to 30% at 36 months[28]. Therefore, the benefit of an ICM strategy for the detection of AF in patients with CS is clear; the number of estimated ICMs necessary to detect a first episode of AF is 14 for 6 months of monitoring, 10 for 12 months, and 4 for 36 months[28]. In addition, a meta-analysis of three randomized controlled trials and 13 observational studies was published including 774 patients with ICM and 996 patients with wearable devices for a median duration of 365 days (range 50–569 days). Pooled odds ratio (OR) showed increased detection of AF with prolonged monitoring (OR 4.54, 95% confidence interval [CI] 2.92, 7.06; P < 0.00001) compared to not-implantable routine follow-up. There was a significantly higher AF detection with ICM (23.3%; CI: 13.83–32.29) compared to wearable devices (13.6%; CI: 7.91–19.32; P < 0.05)[29].
ICM-Related Technical Aspects
The modern ICMs are equipped with an automatic algorithm for AF episodes detection. The arrhythmia detection algorithms are all based on the identification of QRS signals. The AF detection algorithm analyses the stability of the R–R interval, based on the differences in consecutive pairs of QRS cycles. If the variability shows a predefined pattern, the heart rate is classified as AF. The corresponding episode snapshots are stored in the device memory. Additionally, ICM allows the quantification of the daily AF burden, defined as the percentage of time spent in AF. These detection algorithms have been extensively validated using continuous Holter monitoring as the gold standard. Sensitivity and specificity in detecting AF patients ranged from 96% to 100% and 67% to 86%, respectively. Sensitivity was lower when considering the detection of all AF episodes, ranging from 88% to 95% with positive predictive values around 70%[30]-[32]. Complete data are reported in table 2. Despite these positive results, nowadays, the most accurate method for assessing the true AF-burden is represented by CIEDs[33].
Recently, some solutions have been implemented to increase the AF detection performance of ICMs. Among them, an improved algorithm has been developed (Reveal LINQ, Medtronic Inc.) by checking the presence of P waves once the R-R variability exceeds the AF threshold. This algorithm aims to reduce the false positive episodes triggered by runs of atrial ectopies with irregular coupling intervals or sinus arrhythmia, and it was able to reduce inappropriate episodes and duration by 46% and 55%, respectively, compared to the original system[34]. Another solution has been implemented by a different manufacturer (BIOTRONIK SE&Co) in order to reduce false positive episodes caused by the instability between adjacent cycles for ectopic beats. This improved “geminy” algorithm checks not only the immediate adjacent intervals but also every second (bigeminy), third (trigeminy) and fourth (quadrigeminy) interval for periodicity. If such a periodicity is found, AF detection is suspended.
Clinical data are lacking regarding the ICM performance focusing on P wave detection and signal. Currently available devices do not automatically report this information, but the possibility to have visual evidence of the P wave in the sub-ECG snapshot is a real adjunctive value. Improving filtering and amplification of atrial signal frequencies might be possible, as demonstrated by research analysis[35].
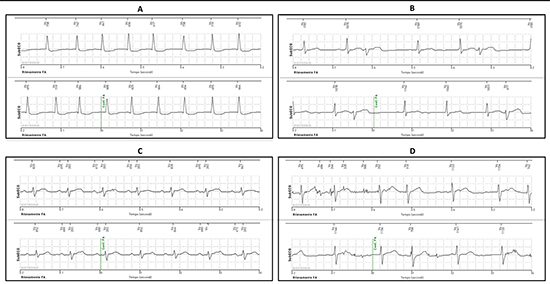
One of the main problems regarding the use of ICMs is the inability to obtain a clear and accurate signal during sub-cutaneous ECG (subECG) monitoring. Artifacts are often present and can hamper the clinical value of these devices, leading to frequent non-diagnostic interrogations. A QRS or R wave undersensing and oversensing may reflect false asystole and false high ventricular rate episodes, respectively[36],[37]. This issue can also interfere with the AF detection performance due to a false high RR variability. The most important action to avoid such a problem is based upon the implantation technique (choosing the implantation site, creating a tight subcutaneous pocket) in order to achieve a higher and more stable R wave sensing. The devices have a dynamic sensing threshold, which is automatically adjusted after each sensed R wave. Higher amplitudes of sensed R waves means higher chances to avoid oversensing of P waves, T waves and noise, while ensuring a reliable sensing of the next R wave. Additionally, it can allow for faster sensing thresholds decreases to avoid R wave undersensing, as the ICM signal is usually affected by intrinsic beat-to-beat amplitude variability. Examples of true and false positive AF episodes are shown in [Figure 1].
Figure 1. Examples of subcutaneous electrocardiogram (subECG) from ICMs identified as AF episodes by the automatic algorithm. (A) True positive AF episode (B) False positive AF episode due to undersensing of premature ventricular contractions (C) False positive AF episode due to oversensing of P waves (D) False positive AF episode due to oversensing of noise. First-line ICM markers (black ticks); second-line ICM subECG; third-line time (seconds).
When dealing with sub-ECG technology, one should always be aware that atrial arrhythmias with regular ventricular response would be probably missed, as they do not exceed the irregularity threshold of the AF algorithm. These episodes might be detected by lowering the threshold for high ventricular rate episodes, but this is not always possible as it may increase the number of false positive events, especially in younger patients.
Another pitfall might be the storage capacity of every ICM device, as the presence of many false episodes might reduce the diagnostic accuracy, because such events may be overwritten due to memory limitation[37]. Newer ICMs, with daily remote monitoring, can overcome this issue, providing the possibility of daily and automatic data transmission, allowing full availability of all episodes in the remote archive, even when the events number exceeds the nominal storing capacity.
Finally, even if the ICM implantation is a minimally invasive procedure, it might carry a risk of minor complications requiring extraction, such as insertion site pain, minor bleeding, and wound infection. The small size of the new devices and the lack of device fixation with sutures also make spontaneous ICM migration along the tissue plane over the chest, axilla, or abdomen plausible, leading to possible loss of signal or difficulties during the next explant procedure. The lack of device fixation is particularly a problem for patients with generous sub-cutaneous fat, in whom a potential ICM migration may lead to a lower signal quality in the follow-up as compared to the one recorded at the time of the implant. However, the incidence of such events appears to be very low, being reported in roughly 1% of the cases[38].
Implantation Considerations
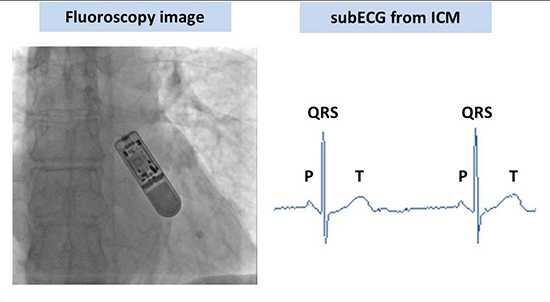
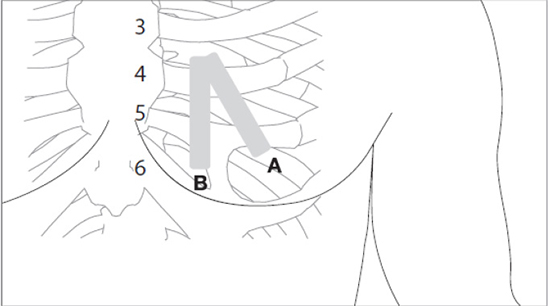
The implantation procedure of injectable or insertable new generation devices has become easier and faster as compared to the implantation of older devices. All systems include an implantation kit and minimal skin opening is needed to execute the subcutaneous device insertion. The typical implant location for an ICM is the left parasternal area of the chest over the fourth-fifth intercostal space. An example is reported in [Figure 2]. There are two recommended inclinations: device parallel to the sternum and device at a 45° angle to the sternum. This second position should be parallel to both ventricular and atrial depolarization vector and, therefore, should maximize the signal of the ICM [Figure 3]. Because the surgical scar in the anterior chest region may have aesthetic implications, especially in younger patients, a transaxillary approach has also been proposed, which provides a more cosmetic implant where the wound is hidden in the left axillary region[39]. A recent study reported that injectable ICMs are usually implanted with an incision site prepared with Betadine or Chlorhexidine. Device fixation is usually not performed and periprocedural antibiotics are used in roughly half of the cases. The wound closure method is usually suture or adhesive strips[38].
Figure 2. Example of ICM implantation with the corresponding final fluoroscopy image and the subcutaneous electrocardiogram (subECG) detected by the device.
Although the procedure is minimally invasive, the feasibility and safety of insertion outside the traditional electrophysiology laboratory has not been deeply investigated. There is only one non-randomized single-center study comparing ICM implantation between the electrophysiology laboratory and a procedure room. There were only 1.7% of overall complications without any significant difference between the two environments[40]. Moreover, an increased risk of complications with the new injectable ICM compared to its predecessor has been reported to be due to the use of the implantation kit and to the lack of suture for the incision[41]. Additionally, a recent case report described a spontaneous external device migration of the new generation device due to the slim profile and the lack of secure skin closure[42]. These data highlight that, despite the easy implant technique, the ICM procedure has to be performed rigorously in order to avoid potential complications.
Figure 3. The typical location of an ICM is in the left parasternal area of the chest over the fourth-fifth intercostal space. There are two recommended inclinations: device parallel to the sternum (B) and device at a 45° angle to the sternum (A).
Finally, one should consider complications arising from the device explant. In fact, the extraction is not always as simple as the implantation procedure, since it may have some drawbacks with the new miniaturized injectable ICMs. First, again in patients with generous subcutaneous fat tissue, it could be difficult to identify the exact device location, and a chest radiograph could become necessary to identify the correct position and avoid multiple incisions[42]. In addition, the skin wound, at the time of the extraction, may be larger as compared to the one performed for the implantation, raising an esthetic issue, particularly in women.
The new-generation ICMs are equipped with remote monitoring (RM) technology. The devices are able to transmit daily diagnostic data and arrhythmic episode snapshots through a wireless receiver without any active patient or physician interaction. Therefore, these transmissions can be reviewed by the hospital staff, who are automatically advised in case of predefined clinical alerts. There are two main advantages related to this technology: (i) avoidance of frequent in-hospital visits scheduled to reduce the risk of loss of information due to device memory overflow, (ii) shortening of the time needed to obtain relevant information and to take appropriate therapeutic action. Although RM has already been proven to be effective in the follow-up of patients with pacemaker or ICD[43], there are few published data regarding ICM. Furukawa and colleagues showed that when RM was used in patients with unexplained syncope, the mean time from ICM implantation to the diagnosis was 28±49 days, which was 71+17 days less than in the clinical practice of 3-monthly in-office follow-up examinations. In addition, RM was well accepted by patients and avoided a 45% of memory saturations which would have occurred without it[44]. A significant reduction in the mean time from implant to diagnosis was also confirmed in a study of 109 patients implanted with ICM for syncope using RM [260 days (range, 5-947 days) vs 56 days (range, 0-650 days)][45]. To date, to the best of our knowledge, there is only a single report regarding RM of ICM for AF reporting promising results. A single center pilot study involving 186 patients suffering from AF demonstrated that 26% of the patients had a clinical intervention triggered by remote transmissions with a mean follow-up of 6 months. All the clinical interventions were performed within 24 hours after the remote alert. The most common response was a change in therapy [46]. In addition, RM may be a useful tool for identifying patients with frequent false positive alerts, allowing immediate corrective actions (i.e. reprogramming the ICM, modifying the predefined RM alerts). However, it should be noted that the RM of ICM generates a higher number of alerts compared with other implantable devices that will need to be reviewed, resulting in a consequent higher workload for the hospital staff[47].
Conclusions and Future Perspectives
In current clinical practice, the use of ICMs is considered a safe and highly effective tool for detecting episodes of AF. Recent technological improvements, including miniaturization, easier implant procedures, and remote monitoring, make this strategy appealing and promising in the real world management of AF patients, leading to a more extensive adoption by expanding the current indications. In the future, the next-generation ICMs may be also integrated with smartphones allowing self-monitoring with a handheld electrocardiogram[48].
However, improvements regarding automatic algorithm are still required for ameliorating AT/AF detection, which may significantly reduce the misdetection rate without affecting device sensitivity. A reliable P wave detection might also be crucial to reach this objective.
There are still some „grey-zones‟ in which the use of such devices could also be useful. In fact, patients with a history of non-persistent AF and intermediate to low thromboembolic risk might benefit from an ICM-guided pharmacological therapy according to the effective AF burden. This approach might prevent the adverse events risk related to both antiarrhythmic and anticoagulant therapy.
Finally, the recent technological improvements do not necessary imply a step forward, as the signal quality of a sub-ECG may be affected by patient-specific features. For this reason, this technology may not represent the best option for every patient. Therefore, it is imperative to weigh the possible benefits against the potential limitations when deciding individualized patient care and especially when dealing with a more extensive adoption of these devices.
GC and CP have nothing to disclose. DG is employee of Biotronik Italia.






