Apixaban-Induced Resolution of A Massive Left Atrial and Appendage Thrombosis
in a Very Elderly Patient
Gloria Santangelo1, Alfonso Ielasi1, Pasquale Antonio Scopelliti1, Francesco Pattarino1, Maurizio Tespili1
1Cardiology Division, Azienda Socio Sanitaria Territoriale Bergamo Est , Bolognini Hospital, Seriate (BG), Italy
.
A 86-year-old woman with first diagnosed atrial fibrillation (AF) underwent mitral valve annuloplasty 10 years before was admitted to our Unit due to congestive heart failure. Trans-thoracic echocardiogram (TTE) revealed a large fluctuant echogenic mass in the posterior wall of the left atrium. Trans-esophageal echo (TEE) showed the origin of the mass within the left atrial appendage. An adjusted dose of the novel oral anticoagulant (NOAC) apixaban, was prescribed. A complete disappearance was appreciated by examination at 12 weeks after the first drug administration. Although apixaban, resulted superior to warfarin in preventing stroke and thrombo-embolic events in patients with non valvular AF, while causing less bleeding, few data are actually available regarding the efficacy and safety of this drug in left atrium and appendage thrombosis management. Our report shows that this NOAC could be a simple and useful option to manage huge atrial thrombosis in very elderly patients.
Correspondence to: Cardiology Division, Azienda Socio Sanitaria Territoriale Bergamo Est, Bolognini Hospital, Via Paderno 21, 24068 Seriate (BG), Italy- gloriasantangelo@hotmail.it
Oral anticoagulant therapy (OAC) is used to prevent thrombo-embolic complications in atrial fibrillation (AF) patients and to resolve left atrial appendage (LAA) thrombosis[1]. OAC is potentially associated with major bleedings[2],requires regular monitoring of the INR and it is not easy to be controlled due to its narrow therapeutic range, food and drug interactions, and varying inter-individual response. At present, novel oral anticoagulants (NOACs) are indicated to prevent thrombo-embolic complications associated with non-valvular AF[3] but few data are actually available regarding the efficacy and safety of these novel drugs in left atrium and appendage thrombosis management, in particular in fragile patients with biological heart valves or prior valve repair.[4]
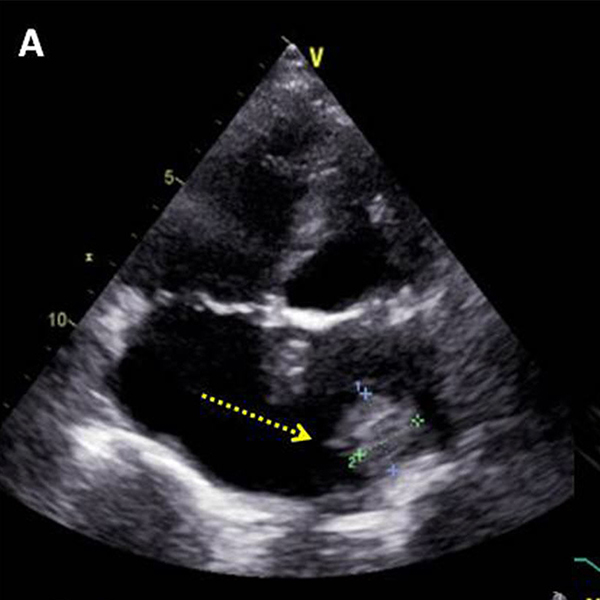
A 86-year-old fragile (height 155 cm, weigh 54 Kg, BMI 22.48) woman with first diagnosed AF, underwent mitral valve annuloplasty 10 years before, admitted to our hospital because of peripheral oedema, and pulmonary congestion with pleural effusion at X-ray evaluation. EKG showed atrial fibrillation with ventricular heart rate of 150 bpm. Blood tests revealed a creatinine (Cr) level of 0.82 mg/mL (eGFR, 41.98 mL/min) and a D-dimer level of 6 μg/mL. Transthoracic echocardiography (TTE) demonstrated a mobile large echogenic mass (1.9x2.3 cm) in the posterior wall of the left atrium ([Figure 1]) and moderate left ventricular dysfunction (ejection fraction 40%). No significant valve heart disease was observed. Trans-esophageal
Figure 1. Transthoracic echocardiography (TTE) shows a mobile large echogenic mass (1.9x2.3 cm) in the posterior wall of the left atrium.
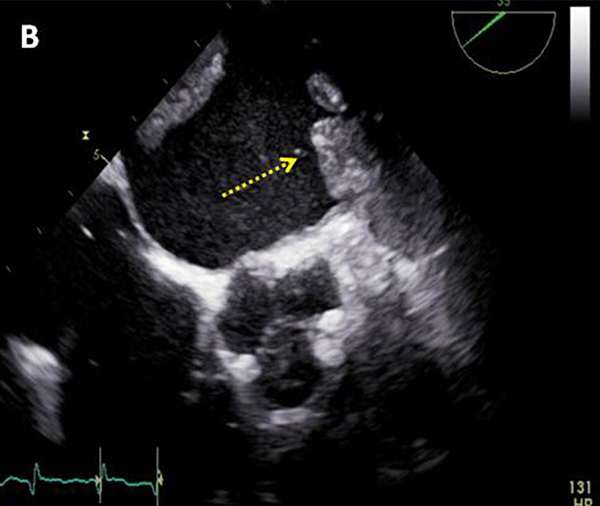
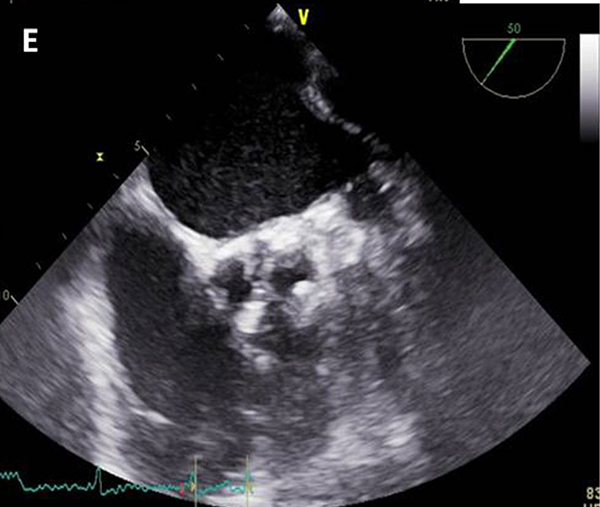
echocardiography (TEE) confirmed the presence of a large homogenous mobile mass in a dilated left atrium coming from the left atrial appendage: diagnosis of thrombus was made ([Figure 2]). No hypercoagulability conditions (hematologic diseases, infections, cancer) were reported. Intravenous furosemide was administered to treat the congestive symptoms while bisoprolol (10 mg daily) plus digoxin (0.125 mg daily) were given orally to achieve a lower ventricular response rate. Because of the very old age and the potential
Figure 2. Trans-esophageal echocardiography (TEE) confirms the presence of a large homogenous mobile mass in a dilated left atrium coming from the left atrial appendage.
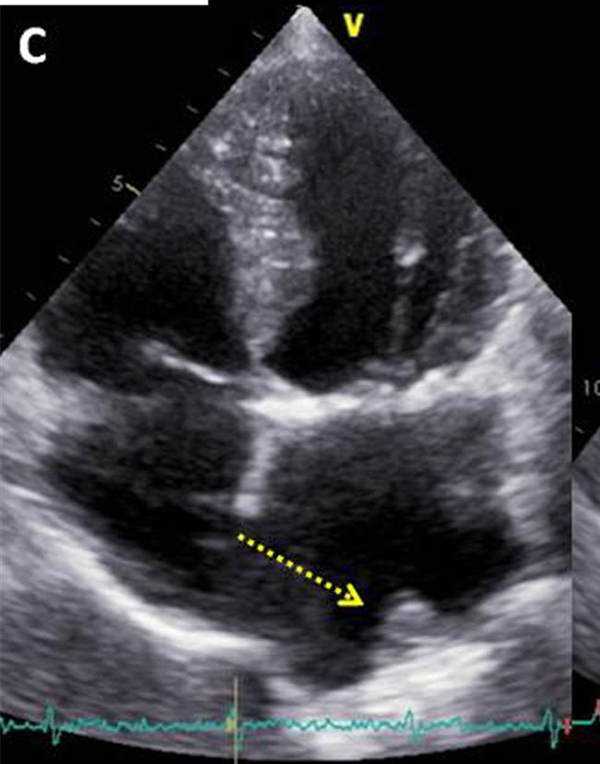
associated difficulties to manage a conventional oral anticoagulant therapy (i.e. warfarin, dicumarol etc.), we decided to treat the massive left atrial thrombosis with the novel oral anticoagulant (NOAC) apixaban (CHA2DS2VASC score: 5, HAS-BLED score: 3). According to the current guidelines, an adjusted (age ≥80 years, weight ≤60 kg) dose of 2.5 mg twice daily was given[5]. A progressive reduction in thrombus size was appreciated by TTE examination 30 days ([Figure 3]) after the first apixaban administration. The NOAC therapy was continued for 12 weeks more without any serious bleeding or thrombo-embolic
Figure 3. Transthoracic echocardiography (TTE) shows reduction in thrombus size at 30 days.
complications, while TTE and TEE finally confirmed the complete thrombus resolution. ([Figure 4] and [Figure 5])Oral anticoagulant therapy (OAC) is used to prevent thrombo-embolic complications in AF patients and to resolve LAA thrombosis[1].
Figure 4. Transthoracic echocardiography (TTE) shows complete thrombus resolution in left atrium.
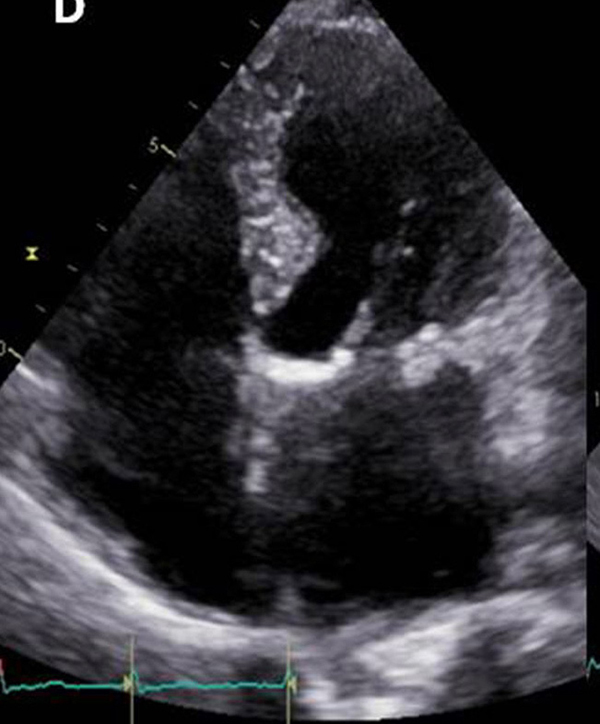
Figure 5. Trans-esophageal echocardiography (TEE) shows complete thrombus resolution in left atrial appendage.
Although OAC is of paramount importance to reduce the stroke rate in AF patients, however it is potentially associated with major bleedings.[2] Furthermore, it requires regular monitoring of the INR and it is not easy to be controlled due to its narrow therapeutic range, food and drug interactions, and varying inter-individual response.
At present, novel oral anticoagulants (NOACs) are indicated to prevent thrombo-embolic complications associated with non-valvular AF (that occurs in case of the absence of mechanical prosthetic heart valves and the absence of moderate to severe mitral stenosis) in patients at high risk of thrombo-embolic and bleeding events[3]. Apixaban is a rapidly absorbed novel oral anticoagulant that inhibits the direct factor Xa (FXa), while has a lower half-life and percentages of renal excretion compared to other NOACs. This novel drug has been shown to be associated in non-valvular AF patients with lower stroke, thrombo-embolic events, bleedings and mortality rates compared to warfarin.[6] However, few data are actually available regarding the efficacy and safety of these novel drugs in left atrium and appendage thrombosis management, in particular in fragile patients with biological heart valves or prior valve repair.[4] Atrial fibrillation in patients with biological valves or after valve repair (conditions that by itself do not require oral anticoagulation) constitute a grey area, and were included in some trials on ‘non-valvular AF’ but no prospective data are available except for the few hundred patients in ARISTOTLE (both types, but without information on how many patients with bioprosthesis) [8] and ROCKET-AF (only valvuloplasty) [9]. Current American Heart Association (AHA) guidelines do not recommend NOAC administration in patients with biological heart valves or prior valve repair. [9] In the case we described, apixaban was chosen as a first line therapy because the surgical intervention was performed 10 years before hospital admission with full preservation of the native mitral valve leaflets while an adjusted dose was preferred because of the patient’s features (old age and low body weight). Recent report has demonstrated that dose reduction to 2.5 mg bd may resolve left atrial thrombi. [10]
The present case shows how apixaban could be an useful drug to resolve left atrial and appendage thrombi within a manageable time period and without major complications in very old patients with limited therapeutic options, late after valve repair. Further, larger data are needed to confirm our anecdotal finding.






