Electrophysiological Perspectives on Hybrid Ablation of Atrial Fibrillation
Faisal F. Syed, MBChB, Hakan Oral, MD
Cardiac Arrhythmia Service, University of Michigan, Ann Arbor, MI.
To overcome limitations of minimally invasive surgical ablation as a standalone procedure in eliminating atrial fibrillation (AF), hybrid approaches incorporating adjunctive endovascular catheter ablation have been proposed in recent years. The endovascular component targets residual conduction gaps and identifies additional electrophysiological targets with the goal of minimizing recurrent atrial arrhythmia. We performed a systematic review of published studies of hybrid AF ablation, analyzing 432 pooled patients (19% paroxysmal, 29% persistent, 52% long-standing persistent) treated using three different approaches: A. bilateral thoracoscopy with bipolar radiofrequency (RF) clamp-based approach; B. right thoracoscopic suction monopolar RF catheter-based approach; and C. subxiphoid posterior pericardioscopic (“convergent”) approach. Freedom from recurrence off antiarrhythmic medications at 12 months was seen in 88.1% [133/151] for A, 73.4% [47/64] for B, and 59.3% [80/135] for C, with no significant difference between paroxysmal (76.9%) and persistent/long-standing persistent AF (73.4%). Death and major surgical complications were reported in 8.5% with A, 0% with B and 8.6% with C. A critical appraisal of hybrid ablation is presented, drawing from experiences and insights published over the years on catheter ablation of AF, with a discussion of the rationale underlying hybrid ablation, its strengths and limitations, where it may have a unique role in clinical management of patients with AF, which questions remain unanswered and areas for further investigation.
Key Words : Atrial Fibrillation, Hybrid Ablation, Surgical Ablation, Rotors, Maze.
Correspondence to: Dr. Hakan Oral,
Cardiovascular Center, SPC 5853
1500 E. Medical Center Drive
Ann Arbor, MI 48109-5853.
The traditional invasive cut-and-sew maze procedure, pioneered by Dr. Cox1,2 and with subsequent revisions culminating in the Cox-maze III, has had a durably high success rate in treating atrial fibrillation (AF), with 80-90% of patients having maintained sinus rhythm without antiarrhythmic medications on long-term clinical follow-up.3,4 Since the simplification of this procedure using surgical catheter ablation technologies as in the Cox-maze IV,5 most maze procedures in the USA are facilitated with surgical catheter ablation.6 Subsequently, minimally-invasive surgical approaches utilizing endoscopically delivered epicardial ablation were developed, parallel to developments in percutaneous catheter-based ablation strategies and technologies,7-14 obviating the need for cardiopulmonary bypass and curtailing postoperative recovery, whilst maintaining a vantage for adjunctive interventions such as epicardial autonomic modulation and left atrial appendage (LAA) excision.15-21 These developments were accompanied by increasing number of patients having standalone surgery for AF, constituting 8% of all surgical AF ablations registered in the Society of Thoracic Surgeons Adult Cardiac Surgery Database between 2005 and 2010.22 However, whereas published outcomes from ablation-facilitated open surgical Cox-maze IV and the traditional cut-and-sew Cox-maze III have been comparable,4,23-26 patients treated with minimally-invasive epicardial surgical ablation have fared less well, in particular those with non-paroxysmal AF.27,28 On pooled analysis of published results, 75% of paroxysmal, 67% of persistent and only 43% of long-standing persistent AF patients are free of arrhythmia recurrence off antiarrhythmic medications.27 A recent systematic review estimated a 10-20% higher rate of recurrent atrial arrhythmias after minimally-invasive surgery as compared to open ablation-based surgery, and although there are no adequately controlled trials or registry data comparing the two approaches directly, this likely underestimates the difference as most open surgical AF ablations in published series have been in patients with long-standing persistent AF (56%, with 8% paroxysmal) whilst most minimally-invasive epicardial ablations were in those with paroxysmal AF (59%, with 8% long-standing persistent).28
Although the mechanisms underlying this observed difference in outcomes are not fully ascertained, electrophysiological observations during minimally invasive epicardial ablations or at the time of catheter ablation of recurrent atrial arrhythmias following such procedures29-33 suggest that these paradoxically inferior results often reflect the demonstrated limitations of current ablation tools in creating transmural lesions sets when applied endoscopically on the epicardium of the beating heart.34-36 Up to 40% of patients undergoing minimally invasive AF surgery have been reported to develop recurrent atrial flutter, with 50% of isolated pulmonary veins having reconnected at time of repeat ablation,30 which is significantly higher than rates of 5 to 10% reported following endocardial surgical ablation,37-39 and is responsive to further catheter ablation.20 By slowing conduction yet failing to impart conduction block, such lesions are not only ineffective at preventing fibrillatory wave propagation40 and AF from recurring41-43 but also establish the tissue substrate required for reentrant atrial tachycardia.44-54 With multiple, incomplete lines, reentrant atrial tachycardia circuits become complex and increasingly challenging to subsequently map and ablate.29
To overcome these limitations of minimally invasive surgical ablation as a standalone procedure in abolishing AF, hybrid ablation was developed, incorporating an adjunctive percutaneous catheter procedure to bridge conduction gaps in the anatomically-based surgical ablation lines as well as additional targets determined electrophysiologically.55-59 This paired utility of surgical and catheter based approaches has been advocated as providing the combined advantage of both, whilst allowing each to overcome the limitation of the other,55,57,59 Ensuring conduction block at the time of surgery significantly reduces recurrence rates; of 93 patients undergoing either open chest or minimally invasive surgical AF ablation, maintenance of AF off antiarrhythmic medications at 12 months was 87% with confirmation of conduction block vs 48% without.32
In this review, we critically appraise the published experience on hybrid ablation, placing it within the context of the experiences and insights attained over the years from catheter ablation of AF. In doing so, we provide a perspective on the rationale underlying hybrid ablation, its strengths and limitations, where it may have a unique role in clinical management of patients with AF, which questions remain unanswered and areas for further investigation.
Systematic Review of Published Literature on Hybrid Ablation of Atrial Fibrillation
Peer-reviewed publications reporting on 5 or more clinical cases undergoing adjunctive minimally invasive epicardial ablation and percutaneous endovascular catheter ablation were identified using Pubmed.gov (US National Library of Medicine, National Institute of Health) using the search term “atrial fibrillation AND (hybrid OR convergent) AND (ablation OR surgery)” (last updated 3/4/2015). This was supplemented by searches on Google Scholar and review of individual studies’ references. We identified 11 unique studies reporting on a total of 432 patients who have undergone standalone hybrid ablation at 11 centers (7 European, 3 North American, 1 Asian) and pooled available demographic, procedural and outcome data of 432 (Tables 1-3).33,56,57,59-66 We included 2 publications where we felt that duplication of case ascertainment was minimal on account of a limited data overlap in recruitment of a patient subset62,65 and excluded 5 publications with probably significant patient overlap selecting in preference those publications which were more recent with greater patient numbers.55,67-70 A further 4 studies (231 patients) were not included as they were published in journals not indexed by the US National Library of Medicine.71-74
Table 1. Systematic Review of Hybrid Ablation Studies – Patient Demographics
| First Author |
No. patients$ |
Publication Year |
Institution(s) |
Procedural Approach |
Energy source |
Age (mean±SD, years) |
PAF |
PrAF |
LSPrAF |
Lone AF only |
| Mahapatra57 |
15 |
2011 |
University of Virginia, Charlottesville, USA |
Thoracoscopic Clamp-based |
RF |
59.5±2.4 |
0 |
9 |
6 |
No |
| Lee56 |
7 |
2011 |
Northwestern Memorial Hospital, Northwestern University, Chicago, USA |
Thoracoscopic Clamp-based |
RF |
NA |
NA |
NA |
NA |
No |
| La Meir59 |
19 |
2012 |
University Hospital Maastricht, Maastricht, The Netherlands |
Thoracoscopic Encircling Catheter |
RF |
60.8±8.6 |
5 |
4 |
10 |
No |
| Pison33 |
26 |
2012 |
University Hospital Maastricht, Maastricht, The Netherlands |
Thoracoscopic Clamp-based |
RF±cryoballoon* |
57.2±8.6 |
15 |
0 |
1 |
No |
| Bisleri60 |
45 |
2013 |
University of Brescia Medical School, Brescia, Italy |
Thoracoscopic Encircling Catheter |
RF |
62.3±9.8 |
0 |
0 |
45 |
Yes |
| Gehi61 |
101 |
2013 |
FirstHealth Arrhythmia Center, Pinehurst and University of North Carolina at Chapel Hill, Chapel Hill, USA |
Subxiphoid Pericardioscopic (Convergent) |
RF |
62.9±9.6 |
17 |
37 |
47 |
No |
| La Meir62 |
35 |
2013 |
University Hospital Maastricht, Maastricht, The Netherlands |
Thoracoscopic Clamp-based |
RF |
57.1±9.5 |
16 |
8 |
11 |
No |
| Kurfirst63 |
30 |
2014 |
Hospital Ceske Budejovic, Ceske Budejovice, Czech Republic |
Thoracoscopic Clamp-based |
RF |
61±8 |
0 |
0 |
30 |
No |
| Lee64 |
10 |
2014 |
Samsung Medical Center, Seoul, South Korea |
Thoracoscopic Clamp-based |
RF |
56.1±7.6 |
1 |
0 |
9 |
No |
| Pison65 |
78 |
2014 |
University Hospital Maastricht, Maastricht, The Netherlands |
Thoracoscopic Clamp-based |
RF |
60.5±7.5 |
29 |
34 |
15 |
Yes |
| Gersak66 |
73 |
2014 |
Multicenter¥ (Slovenia, Poland, Germany, France) |
Subxiphoid Pericardioscopic (Convergent) |
RF |
56.3±10.5 |
0 |
22 |
51 |
No |
| TOTAL** |
432 |
|
|
|
|
mean 60.0 |
83 |
124 |
225 |
|
**Excludes 7 patients reported by Lee et al56 as results pooled with 18 patients undergoing non-hybrid minimally invasive AF surgery; $Additional 8 paroxysmal AF patients not included on account of excluding one study (8 paroxysmal AF and 28 long standing persistent AF)70 with significant overlap in reported patients with Bisleri et al.60; ¥University of Ljubljana Medical Center, Ljubljana, Slovenia; Silesian Center For Heart Diseases, Zabrze, Poland; Herz-und Gefaesszentrum, Bad Bevensen, Germany; L’Institut Mutualiste Montsouris, Paris, France PAF – Paroxysmal AF, PrAF – persistent AF, LSPrAF – long-standing persistent AF; NA - not available; LVEF - left ventricular ejection fraction; RF - radiofrequency
The 432 pooled patients had a mean age of 60 years (range, 56 to 63 years), mean CHADS2 scores (reported in 5 studies, n=250, 58%) 1 to 1.6, mean left atrial diameter (reported in all studies) 4.3 to 5.2 cm, mean left ventricular ejection fraction (reported in 11 studies, n=368, 85%) 47 to 62%, and mean AF duration (reported in all studies) 2.8 to 7.0 years (Table 1). AF was categorized in accordance with guidelines75 as paroxysmal (individual episodes lasting ≤7 days) in 19% (83/432), persistent (continuous AF >7 days) in 29% (124/432) and long-standing persistent (continuous AF > 12 months) in 52% (225/432). A history of prior AF ablation was present in 35% (112/319 with reported data). Four studies (n=163, 38%) included only persistent and/or long-standing persistent AF patients. No study reported inclusion of patients with valvular AF (i.e. associated with rheumatic mitral stenosis, prosthetic or bioprosthetic valve, or mitral valve repair75) or prior cardiac surgery, although these data were not specifically reported in 5 [n=245, 57%] and 4 [n=210, 49%] studies respectively, whilst 2 studies [n=123, 28%] included only lone AF patients.
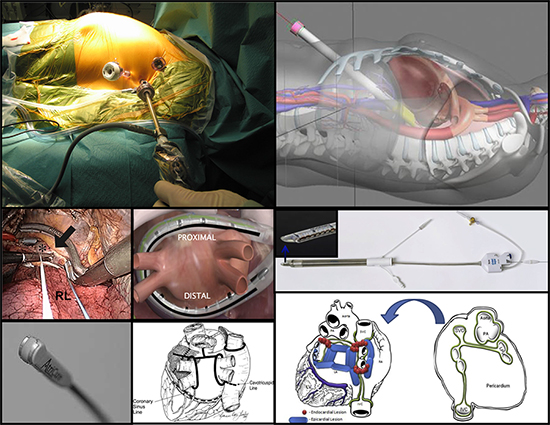
The published experience encompasses 3 different surgical approaches, each utilizing unique radiofrequency ablation tools (Table 2, Figure 1): bilateral thoracoscopy with circumferential and linear lesions (sometimes referred to as LAMP [La Meir, Ailawadi, Mahapatra, Pison] hybrid ablation) created using bipolar radiofrequency clamps and ablation pens (Atricure, West Chester, OH) respectively (6 studies, n=194, 45%); right-sided thoracoscopy with simultaneous isolation of pulmonary veins and posterior left atrium using a suction monopolar radiofrequency catheter (Estech Cobra Adhere XL, Atricure, West Chester, OH) designed to deliver an encircling linear lesion (2 studies, n=64, 15%); and subxiphoid posterior pericardioscopy (through laparoscopic incision of the central diaphragmatic tendon) with linear ablation using a vacuum irrigated unipolar radiofrequency device (Numeris Guided Coagulation System with VisiTrax, nContact Surgical, Inc, Morrisville, NC, USA) to isolate or debulk the posterior left atrium and partially isolate the pulmonary veins (2 studies, n=174, 40%, referred to as the convergent procedure). Pulmonary vein isolation (PVI) was a common end-point in all studies. One clamp-based study33 included 5 patients with severe COPD who underwent only right thoracoscopic radiofrequency epicardial ablation with adjunctive endovascular left-sided pulmonary vein cryoablation to avoid bilateral pneumothoraces.
Figure 1. Hybrid ablation: access, tools and lesions sets. Top and middle left: Left thoracoscopic access as part of bilateral clamp-based approach; lesion (large arrow) created by bipolar radiofrequency clamp (Atricure, West Chester, OH) at right pulmonary vein antrum (asterix). RL – right lung. From Pison, J Am Coll Cardiol 2012;60(1):54-61, with permission. Bottom left: Bipolar pen used for linear ablations in bilateral clamp-based approach. From Sakamoto, J Thorac Cardiovasc Surg 2008;136(5):1295–1301, with permission. Bottom middle: Lesion set in bilateral clamp-based approach, from Mahapatra, Ann Thoracic Surg, Volume 91 , Issue 6 , 1890 – 1898, with permission. Central: Suction monopolar radiofrequency catheter (Estech Cobra Adhere XL, Atricure, West Chester, OH) positioned over the posterior left atrium as used in the right-sided thoracoscopic approach. From Muneretto, Innovations (Phila) 2012;7(4):254-8), with permission. Top right: Transabdominal, transdiaphragmatic access used in convergent approach. From Gehi, Heart Rhythm 2013;10(1):22-8, with permission. Middle and bottom right: Vacuum irrigated unipolar radiofrequency device (Numeris Guided Coagulation System with VisiTrax, nContact Surgical, Inc, Morrisville, NC) used in convergent approach; epicardial (blue) and endocardial (red) lesion set in convergent approach. From Gersack, J Thorac Cardiovasc Surg 2014;147(4):1411-6, with permission.
In addition to the differences in epicardial lesions created by these very different strategies and tools, timing of the endovascular catheter component also varied widely, from being performed immediately after surgery in 5 studies (“immediate-staged”, n=259, 60%) or after a delay ranging from 4 days to 3 months in 4 studies (“delayed-staged, n=100, 23%), with 1 multicenter study (n=73, 17%) reporting an immediate-staged procedure in 2 centers, delayed at >2 weeks in 1 center, and 50:50 split between immediate and delayed at >2 months in 1 center (Table 2). The endovascular component itself varied significantly between studies, such as whether electroanatomical mapping was utilized, choice of linear ablation lesions and which patients these were performed in, whether physiological targets such as triggers and complex fractionated atrial electrograms (CFAE) were targeted, and selection of end-points including intraprocedural confirmation of conduction block and re-induction protocols. There was variation in ganglion identification and ablation, ligament of Marshall ablation, and LAA ligation or excision (Table 2). There was diversity in approaches to peri-procedural antiarrhythmic and anticoagulant management.
Table 2. Systematic Review of Hybrid Ablation Studies – Ablation Details
| First Author |
No. patients |
Ablation Technology |
Epicardial Atrial Ablation |
Intraprocedural Confirmation of Conduction Block: Epicardial |
Ganglion Ablation (identification method) |
LOM ablation |
LAA Intervention |
Endocardial Ablation: Staging |
Endocardial Ablation |
|
|
|
|
|
|
|
|
|
Electroanatomical Mapping |
Confirming Conduction Block |
Findings |
Intervention |
Reinduction |
Triggers |
Flutters |
CFAE |
| Thoracoscopic Clamp-based Approach (n=194, 45%)** |
|
|
|
|
|
|
|
|
|
|
|
| Mahapatra57 |
15 |
Bipolar clamp, bipolar linear RF pen (Atricure, West Chester, OH) |
Bilateral PVI, roof line, anterior line, mitral isthmus line, CS ablation, SVC isolation |
PVI: entrance ± exit; linear: none |
Yes (HFS) |
Yes |
Excision (staple) |
Delayed staged 4.3±1.3 days |
Yes |
PV bidirectional block, SVC isolation, bidirectional block across linear lesions, AF inducibility (isoproterenol) |
Gaps in 0 PVI and SVC lesions, 27% (4/15) of roof lines and 27% (4/15) of mitral isthmus lines |
Consolidation of surgical ablation lines, CTI line, CS ablation, mitral isthmus line and CFAE ablation if AF inducible, ablation of inducible flutters ablated |
Isoproterenol |
No |
Yes |
Yes |
| Lee56 |
7 |
Bipolar RF clamp, monopolar RF pen (Medtronic, Minneapolis, MN) |
Bilateral PVI |
PVI: entrance ± exit; linear: bidirectional |
Yes (HFS) |
No |
Excision (staple) |
Delayed staged >3 months if recurrent AF/flutter |
Yes (presumed) |
PV bidirectional block, criteria for block across lines not stated |
PV reconnections in all 7 patients (mean 2 per patient) at 6±3 months, all with confirmed entrance and/or exit block at time of surgery |
Consolidation of surgical ablation lines, roof and mitral isthmus line, CTI line if typical flutter |
Unknown |
Yes |
Yes |
No |
| Pison33 |
26 |
Bipolar clamp, bipolar linear RF pen (Atricure, West Chester, OH) |
Bilateral PVI, box lesion§, roof line§, mitral isthmus line§, CS ablation, intercaval line§, SVC isolation. Stepwise based on electrophysiological endpoint of non-inducibility of atrial arrhythmia. |
PVI: entrance + exit; linear: bidirectional |
No |
No |
Excision (staple)§ |
Immediate staged |
NoŦ |
PV bidirectional block, bidirectional block across linear lesions |
Gaps in 0 PVI lesions, 23% (5/22) of box and 100% (3/3) of mitral isthmus lines |
Consolidation of surgical ablation lines, CTI line if typical flutter (n=3) |
Rapid atrial pacing and isoproterenol |
No |
Yes |
No |
| La Meir62 |
35 |
Bipolar clamp, bipolar linear RF pen (Atricure, West Chester, OH) |
Bilateral PVI, box lesion, mitral isthmus line*, CS ablation, intercaval line*, SVC isolation* |
PVI: entrance + exit; linear: bidirectional |
Yes (HFS) |
No |
Exclusion (staple or clip)§ |
Immediate staged |
NoŦ |
PV bidirectional block, bidirectional block across linear lesions, AF inducibility (rapid atrial pacing) |
Gaps in linear ablation lesions in 14% (5/35) |
Consolidation of surgical ablation lines, additional linear ablation if AF inducible, CTI line if typical flutter (n=3) |
Rapid atrial pacing and isoproterenol |
No |
No |
No |
| Kurfirst63 |
30 |
Bipolar clamp, bipolar linear RF pen (Atricure, West Chester, OH) |
Bilateral PVI, box lesion, additional roof line |
PVI: entrance + exit; linear: bidirectional |
Yes (HFS) |
Yes (ligation + ablation) |
Exclusion (clips)§ |
Delayed staged 3 months |
Yes |
PV entrance block, unidirectional block across linear lesions, AF inducibility (rapid atrial pacing) |
Gaps in PVI lesions in 87% of right PV, 77% of left PV, 67% of roof lines, and 40% of inferior lines |
Consolidation of surgical ablation lines, CTI line and mitral isthmus line, ablation of inducible flutters |
Rapid atrial pacing |
No |
Yes |
No |
| Lee64 |
10 |
Bipolar clamp, bipolar linear RF pen (Atricure, West Chester, OH) |
Bilateral PVI, inferior line |
No |
Yes (HFS) |
Yes |
Excision (staple) |
Delayed staged 4 days in 8/10 |
Yes |
PV isolation (not detailed) |
Gaps in PVI lesions in 12.5% (1/8) |
Consolidation of surgical ablation lines, CTI line in 6/8 |
No |
No |
No |
No |
| Pison65 |
78 |
Bipolar clamp, bipolar linear RF pen (Atricure, West Chester, OH) |
Bilateral PVI, box lesion, mitral isthmus line§, CS ablation, intercaval line§, SVC isolation§ |
PVI: entrance + exit; linear: bidirectional |
Yes (unknown)§ |
No |
Exclusion (staple or clip)§ |
Immediate staged |
NoŦ |
PV bidirectional block, bidirectional block across linear lesions, AF inducibility (rapid atrial pacing) |
Gaps in 0 PVI lesions and 36% (28/78) of box lesions |
Consolidation of surgical ablation lines, CTI line if typical flutter (n=11), mitral isthmus line completion if perimitral flutter (n=10) |
Rapid atrial pacing and isoproterenol |
No |
No |
No |
| Thoracoscopic Encircling Catheter-based Approach (n=64, 15%)** |
|
|
|
|
|
|
|
|
|
|
| La Meir59 |
19 |
Encircling suction monopolar RF catheter (Estech Cobra Adhere XL, Atricure, West Chester, OH) |
Encircling lesion set - bilateral PVI and box lesion |
No |
(as part of box lesion)# |
No |
No |
Immediate staged |
NoŦ |
Entrance and/or exit block across linear lesions |
Gaps in 89% (17/19) of PVI lesions and 100% (19/19) box lesions |
Consolidation of surgical ablation lines, mitral isthmus line in persistent AF patients (n=3), CTI line if typical flutter seen (n=3) |
No |
No |
No |
No |
| Bisleri60 |
45 |
Encircling suction monopolar RF catheter (Estech Cobra Adhere XL, Atricure, West Chester, OH) |
Encircling lesion set - bilateral PVI and box lesion |
PVI: entrance ± exit; linear: unidirectional |
No |
No |
No |
Delayed staged 30–45 days |
Yes |
PV bidirectional block, bidirectional block across linear lesions, AF inducibility (rapid atrial pacing) |
PV reconnections (7%, 3/45) representing 3/4 with only exit block and 0/41 with bidirectional block immediately after surgical ablation |
Consolidation of surgical ablation lines, CFAE if AF inducible (n=20), CTI line if typical flutter (n=11) |
Rapid atrial pacing |
No |
Yes |
Yes |
| Subxiphoid Convergent Approach (n=174, 40%)** |
|
|
|
|
|
|
|
|
|
|
|
|
| Gehi61 |
101 |
Vacuum irrigated unipolar RF device (Numeris Guided Coagulation System with VisiTrax, nContact Surgical, Inc, Morrisville, NC, USA) |
Non-encircling bilateral antral lesions, box lesion, additional roof line, mitral isthmus line*, CS ablation |
PVI: none; linear: unidirectional |
No |
Yes (undissected) |
No |
Immediate staged |
Yes |
PV bidirectional block, unidirectional block across linear lesions, AF inducibility (rapid atrial pacing) |
Gaps in PVI lesions in 4% (4/101) |
Consolidation of surgical ablation lines, additional roof line (n=90), CS ablation (n=73), mitral isthmus line (n=84), CTI line (n=99), CFAE ablation (n=29). Stepwise based on electrophysiological endpoints of termination to sinus rhythm with no re-inducibility of AF or termination to atrial flutter/tachycardia |
Rapid atrial pacing |
No |
No |
Yes |
| Gersak66 |
73 |
Vacuum irrigated unipolar RF device (Numeris Guided Coagulation System with VisiTrax, nContact Surgical, Inc, Morrisville, NC, USA) |
Non-encircling bilateral antral lesions, box lesion |
No |
No |
Yes (undissected) |
No |
Mixed₸ |
Mixedǁ |
Entrance and/or exit block across linear lesions and PV |
Gaps in all PVI at sites of pericardial reflections - superior margins bilaterally and inferior margin of right inferior pulmonary vein antrum. |
Consolidation of surgical ablation lines |
No |
No |
No |
No |
**Excludes 7 patients reported by Lee et al56 as results pooled with 18 patients undergoing non-hybrid minimally invasive AF surgery; §Selected patients only; *Persistent and/or long-standing persistent AF patients only; #Dissection of ganglion fat pads prior to box lesion application and HFS confirmation of all except right inferior ganglion; ₸Immediate staged in 2 centers, delayed at >2 weeks in 1 center, 50% immediate and 50% delayed >2 months in 1 center; ǁElectroanatomical mapping was not utilized in Slovenia; ŦSites of epicardial ablation identified with fluoroscopic visualization of ablation device in situ. N/A - not applicable - performed as part of box lesion; CS - coronary sinus; CFAE: complex fractionated atrial electrograms
Such diversity in approach is not surprising given the relative infancy of minimally-invasive surgical AF ablation and the novel ablation tools used,27,76 as well as lack of consensus within the ablation community itself on optimal strategies for persistent and long-standing persistent AF.77 An appreciation of electrophysiological principles underlying AF mechanisms and ablation approaches is central to understanding the role of these various approaches as therapeutic strategies for AF and their relative shortcomings.
Electrophysiological Perspective 1 – Heterogeneity of Atrial Fibrillation Mechanisms and Implications for Tailored Therapy
The pathogenesis of AF is often multifactorial. Applying the same therapy as a panacea may risk overtreating some and not addressing underlying mechanisms in others. Whilst the success of the maze procedure is consistent with the principle that a critical mass of atrial tissue is required to sustain fibrillatory conduction,116-118 the cumulative experience from catheter ablation suggests both initiating triggers and arrhythmogenic substrate need to be addressed,119,120 particularly in patients with persistent AF,48,79,80,82-89,91,92,94,121-129 and underlying risk factors are identified and treated.104,105
Electrophysiological Perspective 2 – Insights from Catheter Ablation of Paroxysmal and Persistent Atrial Fibrillation
A major breakthrough in catheter ablation of AF was the finding that myocardial extensions into the pulmonary veins, previously recognized anatomically132 and present in almost all human hearts (Figure 2),133 are a dominant and progressive source of AF triggers amenable to ablation.134,135 The mechanistic cogency of this approach was supported by studies demonstrating that isolating arrhythmogenic veins acutely terminates AF and prevents AF reinduction140 even when tachycardia persists within the vein,140,144-146 and also reduces arrhythmia recurrence compared to focal ablation147 likely by addressing recurrent triggers from elsewhere in the pulmonary veins148 or inter-connected veins.149,150 Once it was realized that atrial myocardium adjacent to the pulmonary ostia, i.e. in the pulmonary vein antra, is a critical source of triggers leading to recurrence after ostial PVI,151 in keeping with its histological and electrical homogeneity with the venous myocardial sleeves,152 the approach was further modified to incorporate these areas (antral PVI or wide-area circumferential ablation [WACA]) with a further reduction in arrhythmia recurrence than with ostial PVI.153-157 In addition to isolating venous146,158-160 and antral arrhythmogenic foci,151,161,164 proposed mechanisms have included disrupting pulmonary ostial anchors for AF drivers (discussed below)128,165,166 and interrupting neuronal connections.81,167,168 A number of randomized clinical trials have demonstrated the efficacy of this approach as a therapeutic strategy for paroxysmal AF,7,9,10,169,174 and of consecutive patients undergoing radiofrequency PVI, approximately 75% and 90% are rendered arrhythmia-free off antiarrhythmic therapy after 1 and 2 ablation procedures, respectively,99 and at 10 years, 75% of patients are arrhythmia free, although 40% require repeat ablation and there have been evolving approaches and technologies over this time.100,175 In addition to symptomatic benefit and quality of life improvement, there is a significantly lower rate of progression to persistent AF (0.5-0.6% per year)100,176,177 compared with pharmacological therapy (8.6% per year).178
Figure 2. Thoracic venous sources of atrial fibrillation triggers. Top: pulmonary vein and vena cavae. Arrows and asterexis identify myocardium in venous structures adjoining the left and right atria. Bottom: Diagram depicting location of the ligament (or vein) of Marshall, the remnant of the left-sided superior vena cava, which has varying degrees of patency in adult life. From Desimone, J Cardiovasc Electrophysiol 2012;23(12):1304-9, with permission. LAA – left atrial appendage; LIPV/RIPV/RSPV – left/right inferior/superior pulmonary vein; IVC/SVC – inferior/superior vena cava.
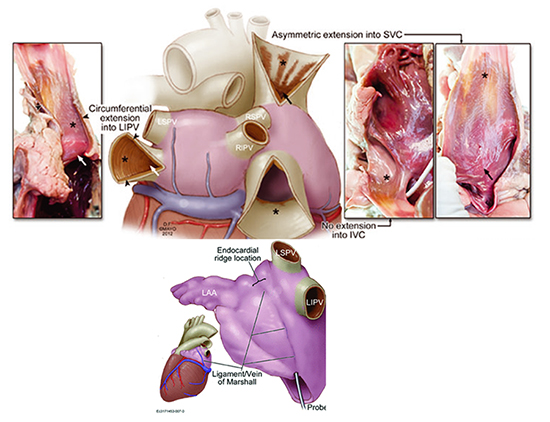
The catheter ablation experience allowed for additional insights into the pathophysiological significance of non-pulmonary thoracic venous myocardium. Atrial myocardium extending into the superior vena cava, seen in 80% of human hearts (Figure 2),133 has similar electrophysiological characteristics to pulmonary venous extensions and can be a source of AF triggers.179,180 It is also present in the coronary sinus, ligament of Marshall and, least commonly, azygous vein (6%).133 Myocardium within the coronary sinus may be a source of rapid repetitive electrical activity during AF and electrically disconnecting it from the left atrium reduces sustained AF induction, suggesting a role in perpetuating AF.181 The ligament of Marshall (Figure 2) is an epicardial remnant of the left superior vena cava, which maintains 3-French probe patency in 70% of hearts and consistently overlies the endocardial left lateral ridge between the pulmonary veins and left atrial appendage.133 It contains both autonomic nerves and muscle fibres, the density of which varies along its length,182 implicated in triggering or sustaining AF183 and providing electrical continuity between the coronary sinus and pulmonary veins.184
Through experience with ablation, there has also been improved understanding on mechanisms and management of post-ablation atrial arrhythmia. Although early arrhythmia recurrence (<3 months) is a powerful predictor for long-term recurrence,185-190 a significant proportion (30%) may go on to be arrhythmia free in the long-term without repeat ablation,185,187 and early restoration of sinus rhythm during this period reduces long-term recurrence rates,192 although additional antiarrhythmic use does not add incremental value to cardioversion.192-195 For late recurrence (>3 months), repeat ablation is superior, as demonstrated by one randomized trial of paroxysmal AF patients with recurrence after antral PVI, with reduced AF burden, symptoms and progression to persistent AF (4 vs 23% at 36 months) compared to antiarrhythmic therapy.196 This is mechanistically consistent with studies demonstrating that recurrence after PVI for paroxysmal AF is usually related to reconnected pulmonary vein conduction,43,47,146,158,177,197-201 likely due to reversible ablation injury with absent circumferential scar on MRI,202-205 or the presence of extrapulmonary ectopic AF triggers.151,158,162 Extrapulmonary triggers are noted spontaneously in about 10% of patients undergoing AF ablation, being several fold more frequent with increasing AF burden and duration (3% of paroxysmal, 8% of persistent and 19% of long-standing persistent patients),99 and in up to 45% following induction with pacing or isoproterenol infusion, most commonly arising from the posterior left atrial wall (20-40%), left atrial appendage (30%), or superior vena cava (30-40%), with a minority from the left atrial roof (8%), ligament of Marshall (8%), crista terminalis (5-10%), coronary sinus (1-10%), and interatrial septum (1-5%).151,163,206-210 It is unknown whether routinely targeting these regions improves outcomes when they are not evident sources of triggers during ablation. For instance, routinely isolating the SVC as a dominant site of extrapulmonary venous triggers has been advocated,180 whilst randomized trials testing this approach have reported conflicting results.211-213
To summarize, in keeping with the predominant trigger-based mechanism underlying paroxysmal AF, catheter ablation studies have demonstrated that an anatomically guided approach to PVI leads to sustained improvement off antiarrhythmic drugs in the majority of patients and offers a definite end point of electrical isolation of the pulmonary vein. Although the extent of atrial fibrosis correlates weakly with clinical phenotype,78 with some paroxysmal AF patients having high atrial fibrosis burden, systematic substrate modification offers no incremental benefit,214-222 even with late recurrent paroxysmal AF requiring re-ablation,223 and may even predispose to macroreentrant atrial tachycardias.216,224
This contrasts with insights gained from catheter ablation of persistent and long-standing persistent AF, where dominant fibrillating frequency shifts away from the pulmonary veins to other left or even right atrial sites144,161 with PVI offering limited success on its own225-228 and additional substrate modification becoming necessary to improve ablation outcomes,8,131,157,229,230 all in keeping with the underlying transition from a predominant trigger-based paradigm to one with increasing influence from extrapulmonary drivers and atrial substrate.128,209,231 However, there is mechanistic overlap, such that in persistent AF there is evidence of ongoing dynamic interplay between pulmonary vein triggering and atrial activation144 and PVI may acutely reduce left atrial dominant activation frequency,232 partially organize AF without necessarily affecting dominant frequency,233 or acutely terminate AF.121,144,227 Accordingly, atrial substrate modification alone without PVI results in inferior outcomes.228,234,235 Nonetheless, atrial substrate, no matter how defined, is a strong predictor of recurrence after catheter ablation of persistent AF78,201,236-238 and outcomes have been better with more extensive atrial substrate modification.124,230 To what extent this reflects current uncertainty over how best to identify pathogenic versus bystander substrate and appropriate end-points for ablation are areas of ongoing investigation.131
Electrophysiological Perspective 3 – Successful Substrate Modification and Ablation End Points in Persistent Atrial Fibrillation
An intriguing finding from the PRAGUE-12 randomized trial is that restoration of sinus rhythm was significantly higher with increasingly persistent AF comparing maze to no maze in patients undergoing cardiac surgery (paroxysmal 62 vs. 58%, persistent 72 vs. 50% and long-standing persistent AF 53 vs. 14%, P < 0.001).239 The ability to observe in real time the effects of progressive substrate modification on atrial activation locally, remotely and globally whilst correlating this with structural, functional, and outcome data have allowed for novel insights into mechanism underlying arrhythmia and ablation efficacy in persistent and long-standing persistent AF. Improved catheter ablation outcomes have been reported when additional substrate modification is incorporated in an individualized, stepwise fashion to either reduce AF dominant frequency (>11%)240 or terminate AF,129,238 with adjunctive ablation of spontaneous and inducible atrial tachycardias.127,241,242 With this approach, long-term freedom from AF off antiarrhythmic medication has been reported in 65-75% of patients,129,238,240,242 and though 15-30% of patients with long-standing AF may require 3 or more procedures, recurrences are more likely to be from reentrant atrial tachycardia rather than recurrent AF,129,238 albeit the benefits of AF termination decline with longer AF duration (>3 years in one study).243 There is currently no consensus on what constitutes optimal substrate modification in persistent AF, with reported benefit from an anatomical approach through creating point-by-point ablation lines (linear ablation) following the success of the surgical maze procedure;46,51,229,232,244-246 isolating the posterior left atrium in this manner,247,248 ablating sites with complex fractionated atrial electrograms (CFAE) during fibrillatory conduction as a strategy to modify electrical substrate;217,219,226,234,249-251 identifying and ablating focal drivers;109,113,123,126,128,252,253 and ablating autonomic ganglia as AF modulators.82,84,86,88,91,92,254
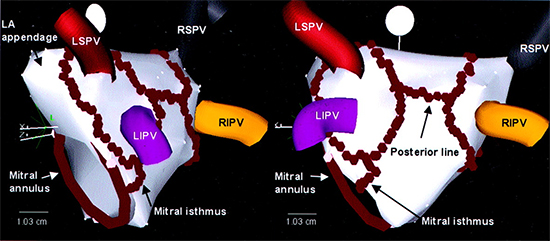
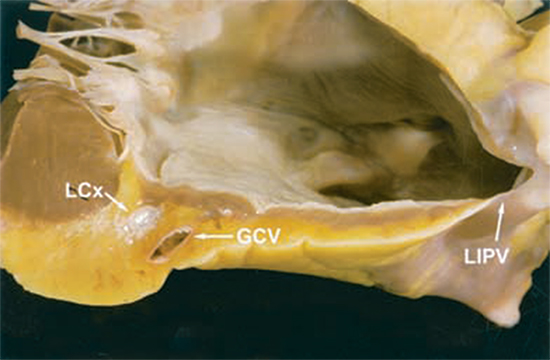
The most extensively investigated linear ablation lesions during catheter ablation are the roof line, which connects the superior pulmonary veins (to mitigate risk of atrio-esophageal fistula from ablating over the esophagus posteriorly), and mitral isthmus line connecting the left inferior pulmonary venous antrum to the mitral annulus (Figure 3).48,153,232 When such ablation is successful, it results in dominant activation frequency reduction and cycle length prolongation, which may progress with further ablation to AF termination, often to a macroreentrant atrial tachycardia circuiting around the left atrial roof, mitral isthmus, or cavotricuspid isthmus.48,232 Of those still in AF on completion of antral PVI, 60% are left non-inducible for AF after one linear lesion and 95% after two.121 Analyzing frequency-domain transformed activation signaling during linear ablation reveals that acute reductions in dominant activation frequency do not occur until completion of conduction block and coincide with disappearance of discreet lower frequency sources, characteristics of which were consistent with reentrant drivers, an effect not seen after PVI or CFAE ablation in this study.232 Linear ablation may therefore work by disrupting localized reentrant drivers. Results from whole atrial phase and organization index mapping also suggest this.128,166,255 In addition, linear ablation may reduce subsequent macro-reentrant atrial tachycardia by creating lines of conduction block across critical anatomical isthmi, yet predispose to it when conduction block is not achieved.51,54 The major limitation of linear ablation is therefore difficulty in achieving sustained conduction block,50 particularly at the mitral isthmus (Figure 4) where 40-70% of patients require additional epicardial ablation from within the coronary sinus and 10-35% are left without conduction block,256-258 especially in areas with anatomical irregularity (such as with a pouch), or interpositioned coronary vessels presumably causing a heat sink.257-259 Even if successful conduction block is achieved at index procedure, late recovery of mitral isthmus conduction is seen in 75% of instances (much higher than after cavotricuspid isthmus block [25%]) and predisposes to perimitral flutter.260 The incidence of perimitral flutter is higher after routine mitral isthmus ablation and requires further reablation to achieve lasting freedom from recurrence.53
Figure 3. Ablation lines created during left atrial ablation represented on a 3D electroanatomical mapping system (CartoTM). Individual ablation lesions are represented by red tags. From Oral, Circulation. 2003;108(19):2355-2360, with permission.
As with antral PVI, gaps in conduction block in linear lesions resulting in reentrant atrial tachycardias is the most common cause for arrhythmia recurrence,45,46,50,52-245 and may explain why the recently published STAR AF II randomized trial,261 in which linear ablation resulted in acute conduction block in only 74% of patients and intraprocedural AF termination in 22%, failed to demonstrate benefit of linear ablation over antral PVI, and also why a recent meta-analysis demonstrated a significant reduction of AF recurrence with linear ablation but not with more extensive linear lesion sets.235 In addition, although patients may manifest with perimitral flutter following persistent AF ablation, they still stand to benefit from confirmation of PVI and ablation of extra-pulmonary triggers, which may by itself result in more patients having reduced arrhythmia recurrence than if the mitral isthmus alone is ablated and blocked, indicating that triggering may underlie some macroreentry post-ablation flutters.252 As for routinely creating linear lesions in the right atrium, cavotricuspid isthmus ablation during AF ablation does not reduce long-term arrhythmia recurrence262,263 unless typical atrial flutter is demonstrated either clinically or during the ablation procedure.264,265 These principles also extend to effective surgical lesion sets.29 Limiting lesion sets also reduces the likelihood of complications, as illustrated by a recent meta-analysis comparing left atrial and biatrial maze which reported equivalent long-term success but with increased pacemaker implantation with biatrial maze.266
Figure 4. Human heart demonstrating cross-section of the mitral isthmus. The thickness of the atrial myocardium, epicardial fat and associated vasculature are demonstrated. From Becker, J Cardiovasc Electrophysiol 2004;15(7):809-812, with permission. LCx – left circumflex artery; GCV – great cardiac vein; LIPV – left inferior pulmonary vein.
In a prior study CFAE ablation was reported to significantly improve ablation outcomes as an adjunct to PVI, but as standalone therapy the results were inferior to PVI (1 year arrhythmia-free rates 74 vs. 48 vs. 29% after one procedure in the STAR AF trial).234 In about 20% of patients, AF terminates whilst ablating a CFAE267,268 and an acute decrease in dominant frequency with CFAE ablation predicts reduced recurrence of AF.269 Certain CFAEs are more likely to terminate AF or reduce its dominant activation frequency than others, such as those with greater duration of continuous activity or complexity,270-273 whilst other CFAEs may represent bystander activation as suggested by studies demonstrating a reduction in CFAE number and location immediately following PVI or linear ablation.268,271,274 Judicious selection of target sites is therefore needed, whilst identifying appropriate CFAE targets based on grading complexity is somewhat subjective and can be erroneously overestimated at overlapping structures including the interatrial septum. This may explain why, when guided by automated software protocols, CFAE ablation was reported to offer no additional benefit to antral PVI by the STAR AF II trial261 and, as reported by another randomized trial, have inferior outcome to linear ablation despite more extensive lesions with greater cardiac enzyme release.275 Further evidence of the importance of strategic CFAE ablation comes from a trial demonstrating no added benefit when right atrial CFAE ablation is routinely added to left atrial CFAE ablation.114 The three published randomized studies directly comparing linear with CFAE ablation have reported either inferior performance of CFAE ablation,275 as noted above, or equivalence of the two procedures,261,276 though with CFAE ablation resulting in higher rates of intra-procedural AF termination261 and recurrences which are less likely fibrillation and more likely atrial tachycardia.276
The observation that terminating or slowing AF by ablation at discreet sites modifies atrial substrate in a manner which renders the atrium significantly less likely to fibrillate suggests that the influence of even advanced substrate surrogates in determining recurrence can be overcome by focal ablation.128,166,245,255,267-273 Whole atrial activation, phase, frequency and organizational index mapping has identified the presence of rotor-like activity and focal high-frequency sources driving AF.111-113,123,126,128,166,277-283 Ablation of these domains acutely terminates AF,128,255 though with longer durations of AF these drivers become more numerous and acute termination is less frequent (75% and 15% of persistent and long-lasting AF terminated, respectively, >6 months cutoff).128 Though their location varies between individuals,123,128,255,282 they are predominantly left atrial (70%), with the rest being right atrial (30%),128,255 and demonstrate relative spatiotemporal stability with most meandering over 5-10 cm2 areas around the pulmonary antra, antrally-associated septum and appendage, or left inferior wall/coronary sinus,128 consistent with earlier data identifying these as sites where ablation is most likely to terminate AF.245 What determines the observed relationship to these critical areas is unknown284 and likely involves interplay between individual variation in atrial and pulmonary ostial geometry,285 fiber orientation and anisotropy,286-288 fibrosis,289-291 regional variation in autonomic innervation and tissue response to autonomic input,83,85,86,292 and geometrically governed variability in exposure to mechanical stress and pressure.293-295 By imaging fibrosis using MRI, the likelihood of recurrent arrhythmia after ablation has been correlated to the extent of fibrosis left unablated, indicating that substrate modification works best when it targets such fibrotic areas, likely by converting proarrhythmic tissue with heterogenous fibrosis to homogenous inert scar.230 A stepwise ablation approach also effectively reduces intrinsic scar burden,296 indicating that both electrophysiologically and anatomically defined targets are likely co-localized. An approach tailored to targeting low voltage (<0.5mV) sites during sinus rhythm as areas representing fibrosis was recently shown to be feasible and associated with comparable outcomes to patients without any atrial scar.297
These data provide a mechanistic link between substrate, clinical characterization of AF and the observed responses to ablation. By identifying individual-specific mechanistic targets, providing novel insights into the role of atrial structural changes,286-288,291,297,298 better understanding why the currently established substrate modification strategies of linear and CFAE ablation sometimes demonstrate greater effect128,232,271,280,299,30 than at other times,261,274,298,301-303 these approaches raise the possibility that successful persistent AF ablation need not necessarily depend on standardized, extensive atrial compartmentalization or debulking by providing novel patient-specific ablation end-points,126,128,230,281,297,304 though this remains an area of ongoing investigation.
Electrophysiological Perspective 4 – Creating Effective Ablation Lesions: Endocardial vs. Epicardial Approaches
As with the endocardial approach, demonstrating effective conduction block across linear lesions is key to successful epicardial AF ablation.29,32 With viable myocardial strands as thin as 1 mm allowing for electrical propagation,40 creating contiguous transmural lesions is the goal with both approaches and dependent on choice of ablation energy,305 electrode and catheter design, interplay of biophysical response characteristics of targeted tissue and its related anatomy,306,307 including variation in atrial wall thickness regionally (thickest at the roof, mitral isthmus and left lateral ridge308) and between individuals (posterior wall 0.9 to 7.4 mm in one study),309 atrial and pulmonary venous morphology257,310,311 and associated vasculature.257 The published hybrid ablation experience has thus far exclusively incorporated radiofrequency ablation (Table 2), which relies on current flow alternating at radiofrequency causing resistive tissue heating and depends fundamentally on electrode-tissue contact.312,313 Additional variables affecting lesion depth include power and duration of ablation,314 electrode size and orientation,315-317 electrode tip cooling to prevent surface char and coagulum allowing for deeper lesions,318,319 electrical tissue impedance,314 and tissue heat sinks.35,306,307,320 Monitoring electrode contact force, temperature rise, impedance fall, and electrogram diminution allows real-time monitoring of lesion evolution surrogates and safe ablation,313 though none of these parameters obviate the need for confirming conduction block.29
Despite these measures, and documentation of block acutely, conduction may recover and whether this is from tissue regeneration or incomplete ablation and reversible injury is unknown.284 The latter is supported by data demonstrating that common locations of late recovery after endovascular catheter ablation are sites with known difficulty in maintaining catheter tissue contact (close to the pulmonary veins, left lateral ridge, mitral isthmus, accessory pulmonary veins or a common left pulmonary vein ostium);50,311,321-323 electroanatomical correlation of gaps with measured tissue contact force;322,323 echocardiography324 and contrast MRI showing evidence of reversible injury with edema which resolves on serial scans205 with recovery over days to weeks, and incomplete scarring at ablation sites with conduction recovery;203,204 and histological evidence of non-transmural lesions in pulmonary veins that reconnect late after PVI.325 In addition, outcomes are better when areas with reversible injury are re-ablated once identified after a 60-90 minute wait period326 and/or adenosine,326-328 ablating to unexcitability as a superior tissue endpoint to conduction block,329 measuring and maintaining tissue contact force to deliver more effective lesions,322,330-332 and visually identifying gaps after electroanatomically tagging ablation lesions.333,334
The specific additional challenges with an epicardial approach include constraints from mediastinal anatomy and pericardial reflections335 in accessing individual-specific arrhythmogenic triggers and substrate; the increased proximity and risk of collateral injury to great vessels, coronary arteries, lungs, mediastinum, esophagus, liver, diaphragmatic vessels, and phrenic nerves;335 how well suited catheter design is for navigation, maintaining tissue contact over the smooth epicardial convexity of the beating heart and safe delivery of ablation energy; how well matched the selected ablation energy is for the local tissue environment and characteristics;305,336 how to overcome endolumenal and intramural arterial heat sinks,35,306,307,320 the presence of epicardial coronary vessels at key linear lesion sites (mitral and cavotricuspid isthmus), and presence of epicardial fat which limits energy delivery to underlying myocardium305,306,337 as well as independently influencing AF pathophysiology and recurrence after endocardial ablation.338
To overcome these challenges, minimally invasive surgical approaches have incorporated versatile access and catheter designs to facilitate controlled tissue manipulation and ablation. The bipolar radiofrequency clamp (Atricure, West Chester, OH) which is utilized for PVI with the bilateral thoracoscopic hybrid approach has favorable preclinical results,36,339 though a variable number of repeat applications (at least 3 and often more in clinical studies29,31) are required to achieve block and reconnection gaps are increasingly prevalent over time from none when tested immediately33,65 to 12.5% after 4 days64 and 87% of right and 77% of left pulmonary veins at 3 months.63 Bipolar sources have been reported to create better lesions than monopolar sources with epicardial ablation.340 Additional linear lesions created with the bipolar radiofrequency pen (Atricure, West Chester, OH), which again has good preclinical efficacy data,34,341 resulted in reconnection gaps in 14-36% of box lesions at immediate staged endovascular testing,62,65 27% of roof and mitral isthmus lines at 4.3±1.3 days,57 and 63% of roof and 40% of inferior lines at 3 months63 even when bidirectional block was confirmed during epicardial ablation. To overcome limitations in mitral isthmus linear ablation from attempts to avoid coronary arterial injury,58 some investigators connected the left fibrous trigone to the mitral annulus.29 However, whether this has similar efficacy and propensity to disrupt focal drivers or reentrant flutters is unknown. Similarly, ablation lines across Bachmann bundle are hard to establish due to atrial thickness and results in inter-atrial dyssynchrony.63 The bilateral thoracoscopic approach additionally allows visualized access to the epicardial ganglia, ligament of Marshall, and left atrial appendage, can protect or maneuver away from critical anatomical structures, but requires collapsing the lung and opening the pericardium on each side.
The right-sided thoracoscopic approach and convergent (posterior pericardioscopic) approaches utilize specially designed linear ablation monopolar RF catheters incorporating suction to increase tissue contact and optimize catheter stability (Estech Cobra Adhere XL, Atricure, West Chester, OH, and Numeris Guided Coagulation System with VisiTrax, nContact Surgical, Inc, Morrisville, NC, USA, respectively), allowing for less invasive access than the bilateral thoracoscopic approach. Both of these catheters performed less well than the bipolar clamp in preclinical studies.34 However, with the encircling suction catheter (Estech Cobra Adhere XL), when applications were repeated until entrance and/or exit block in conduction to/from the posterior left atrium, block was maintained after 1 month at endovascular in all with bidirectional block and 25% with unidirectional block at epicardial ablation.60 In contrast, when block is not tested for during epicardial application, almost all had conduction gaps during immediate-staged endovascular study.59 The ablation line also abolished standardized ganglionic responses except at the right inferior ganglion, which was located outside the box lesion.59 A limitation with the unilateral right-sided approach is lack of access to the left atrial appendage. The convergent approach avoids thoracoscopy altogether, utilizing laparoscopy to guide subdiaphragmatic posterior pericardioscopy.55,68 Space constraints limits placement of additional catheters for simultaneous electrophysiological monitoring and, although inferior and posterior left atrial surfaces are well visualized, the superior and anterior lesions need to be made without direct visualization and rely on knowing catheter angulation and orientation. Pericardial reflections lead to discontinuous lesions at both superior and right inferior pulmonary veins, necessitating routine endocardial touch-up lesions at these sites, whilst access to the ligament of Marshall, appendage and ganglia is limited and the esophagus is left more vulnerable than with the bilateral thoracoscopic approach.55,68 Although the other hybrid approaches have isolated the posterior left atrium, the convergent approach has focused on debulking this region. There are no data comparing the two approaches directly.
When electroanatomical mapping was not utilized to register lesions during epicardial ablation, techniques to correlate with the endovascular component during immediate staging involved leaving the epicardial ablation catheter in situ to correlate fluoroscopically or gently prodding epicardially at the ablation line whilst correlating endocardial catheter position with intravascular ultrasound.
Electrophysiological Perspective 5 – Cardiac Autonomic Ganglia as Targets during Atrial Fibrillation Ablation
An autonomic etiology for AF was first recognized with description of vagally-induced AF in 1978.342 Pulmonary vein isolation has reduced efficacy in treating paroxysmal vagotonic AF,80 whereas atrial vagal denervation can abolish it.88 The importance of autonomic influences on AF is also evident from a reduction in AF recurrence following antral PVI when vagal responses (bradycardia, atrioventricular block, hypotension) are fortuitously elicited during radiofrequency ablation and abolished,81 the increase in late AF recurrence in those with high serum titres of autoantibodies against the beta-1 adrenoceptor and M2 muscarinic receptor at the time of cryoballoon PVI,96 and in the post cardiac transplantation population, whose denervated recipient hearts are relatively resistant to AF with 70% lower AF incidence than matched patients undergoing cardiac surgery with left atrial maze.90
The atria are richly innervated by autonomic nerves343 and between 700-1500 epicardial ganglionated autonomic neuronal plexi are associated with the heart, though numbers decline by up to 50% with age, with complex circuits involving both parasympathetic and sympathetic components.344 The atrial ganglia are primarily clustered at the superior right atrium, superior left atrium, posterior right atrium, posteromedial left atrium, and the inferolateral aspect of the posterior left atrium.344 Following the demonstration in dogs that ganglionic stimulation induces calcium-mediated pulmonary vein triggers345 and enhances trigger-induction of AF, with the opposite effects with ganglionic block,292 studies began to focus on modifying local autonomic atrial input by targeting epicardial ganglia to improve outcomes of catheter AF ablation82 and surgical maze.346 After validation of the technique in dog experiments, eliciting bradycardic responses and atrioventricular block at sites of high frequency atrial burst pacing has been used to map ganglionic cluster sites from the endocardium82 with descriptions of five common left atrial sites (superior left, inferior left, ligament of Marshall, anterior right, inferior right).86 Although some ganglionic sites may not elicit such a response yet still exert modulatory influence,84 whilst surgical approaches are able to directly visualize these ganglia, elimination of the high frequency stimulation response may serve as a useful ablation end-point. Such ganglionic responses were shown to be present in 86% of 216 patients after antral PVI and predicted arrhythmia recurrence in patients with paroxysmal AF (51 vs 8% at >6 months) but not persistent AF (40 vs 39%), even though a higher proportion of persistent AF patients had positive ganglionic responses.94 Ganglia may also co-localize with CFAE although the mechanism is not fully explained.83,85,86
There is currently no consensus on whether to routinely perform ganglion ablation during catheter ablation of AF.347 A meta-analysis of six randomized trials (342 patients) concluded that ganglion ablation improves the results of catheter PVI or surgical maze in reducing freedom from AF recurrence, but as standalone therapy the outcome is inferior to PVI,348 with similar results in a recent trial of 242 patients with paroxysmal AF (at 2 years, freedom from recurrence 74 vs 56 vs 46%, respectively).92 In persistent AF, even though retained ganglionic responses after antral PVI may not predict AF recurrence,94 trials of ganglionic ablation during both catheter ablation91 and surgical maze346 have reported positively on efficacy. Long-term outcomes are unknown, with dog data demonstrating the reappearance of ganglionic responses with time,349 presumably due to axonal regrowth, whilst isolated ganglionic ablation (i.e. without PVI) may be paradoxically proarrhythmic.350
Electrophysiological Perspective 6 – Stroke Prevention and Left Atrial Appendage Closure
Stroke mechanisms in AF are complex and demonstrating a role for fibrillation independent to atrial myopathy and vascular disease is challenging as both not only predispose to AF but also to stroke risk with AF.351 There are at present no randomized data demonstrating that AF ablation, whether surgical or catheter-based, reduces stroke risk. Although Cox et al reported a low incidence of stroke (0.7%) after the cut-and-sew maze procedure in 265 patients followed for 11.5 years,352 the majority had low stroke risk at baseline and the study was non-randomized. The PRAGUE-12 trial randomized 224 patients undergoing cardiac surgery to concomitant maze or no maze, and reported 1-year stroke rates of 2.7 vs. 4.3% (p=0.319).239 Overly aggressive atrial compartmentalization and debulking may paradoxically increase stroke risk by rendering the atrium without contractile activity despite restoration of sinus rhythm, mitigating any benefit.353 In a large, unselected catheter ablation cohort, 2% developed stroke after 1,347 patient-years follow-up, with no significant difference when sinus rhythm was maintained, though the study was probably underpowered as most patients had low baseline stroke risk.175 A study of 4,212 patients who underwent AF ablation reported reduced risk of stroke, death and dementia compared to 16,848 age-gender matched controls with AF but no ablation, with similar rates to 16,848 age-gender matched controls without AF.354 The results of the CABANA trial (clinicaltrials.gov/ NCT00911508), which aims to study the effects of catheter ablation on mortality, stroke and bleeding as compared to drug therapy, are awaited.
Recent advances in cardiac imaging have allowed an appreciation that morphological complexity of the LAA significantly influences thromboembolic risk, supporting a structural approach to thromboprophylaxis.355 The efficacy of this approach was demonstrated by the WATCHMAN trial of percutaneous LAA occlusion.356 A meta-analysis of 7 studies including 3,653 patients undergoing appendage closure (n = 1716) versus not (n = 1937) at the time of cardiac surgery reported a significantly reduced stroke incidence with closure (0.95 vs 1.9% at 30 days, 1.4 vs 4.1% at last follow-up) and reduced mortality (1.9 vs 5%).357 Surgical approaches, however, have been limited by incomplete closure, with surgical amputation and oversewing yielding highest maintained closure rates.351 Results of the LAAOS III trial (clinicaltrials.gov/ NCT01561651), which plans to randomize 4,700 patients undergoing cardiac surgery to LAA occlusion or no occlusion, are awaited. A number of minimally invasive approaches have been developed, using either suture or clip exclusion or staple excision, though none have yet been proven to reduce stroke.351 In addition, LAA exclusion may not be regarded as a panacea for stroke reduction in AF, as vascular mechanisms may coexist and thrombi are more likely to be extra-appendicular in valvular AF patients.358 There are also hemodynamic sequelae which are in keeping with loss of its compliance and atrial booster function.359,360 In addition to modulating stroke risk, appendage ligation or excision results may serve as a form of substrate modification361 by reducing atrial mass118 and eliminating appendage triggers and drivers,362,363 whereas electrical isolation without mechanical closure may paradoxically increase stroke risk through appendage blood stagnation.364
Electrophysiological Perspective 7 – Hemodynamic Impact of Atrial Fibrillation Ablation
In the majority of individuals, restoration of sinus rhythm with ablation leads to significant improvement in left ventricular function, effects that extend beyond rate control,11,365,366 even when baseline ejection fraction is normal,367 with improvements also reported after surgical maze.368 Restoration and maintenance of sinus rhythm results in reverse atrial remodeling8,369,370 and similar effects are seen after surgical maze,371 although with time these effects can subsequently reverse372 and it is unclear whether this is due to the maze procedure itself or persistent risk factors leading to progressive atrial myopathy. Without the expected benefits of reverse atrial remodeling from immediate restoration of sinus rhythm, such as those with paroxysmal AF and low arrhythmia burden, a reduction in atrial contractile function is seen after maze, more so with more extensive ablation (new left atrial dysfunction 8.5% after PVI compared to 30% after additional linear ablation).373 Surgical maze may result in reduced atrial compliance which can cause severe, symptomatic pulmonary hypertension (“stiff left atrial syndrome”).374 This has also been reported after catheter ablation in 1.4% of 1,380 patients, predisposing factors being smaller pre-procedural left atrial size (≤45mm), preexisting left atrial hypertension, increased baseline left atrial fibrosis, diabetes mellitus and obstructive sleep apnea.375
Electrophysiological Perspective 8 – Critical Appraisal of the Role of Hybrid Ablation in Improving Outcomes from Atrial Fibrillation Ablation
Outcome from Hybrid Ablation of Atrial Fibrillation: Results of Systematic Review
Published success rates from hybrid ablation (Table 3), defined as maintained sinus rhythm off antiarrhythmic medications at 12 months, are 74.3% overall (data available for 81% [350/432]), 76.9% for paroxysmal (data available for 76% [65/83]) and 73.4% for persistent / long-standing persistent AF patients (data available for 62% [218/349]). Methods used to detect recurrence varied from a 24-hour Holter monitoring at prespecified follow-up intervals to continuous ECG monitoring using implantable loop recorders or pacemakers and defibrillators (Table 3). Success rates differed significantly among the three approaches (Table 3), with highest rates reported with the bilateral thoracoscopic clamp-based approach (88.1% [133/151]), intermediate with the unilateral thoracoscopic suction encircling catheter-based approach (73.4% [47/64]) and lowest with the convergent approach (59.3% [80/135]), p<0.001). The difference in the proportion of patients with long-standing persistent AF (37% [72/205]), 86% [55/64] and 56% [98/174] respectively, p<0.001) may partly account for some of this difference in outcome (Table 3). However, when data were available, success rates in patients with persistent and long-standing persistent AF were similar to overall success rates (88.2% [82/93], 74.6% [44/59] and 51.5% [34/66] respectively, p<0.001). There was limited separately reported 12-month data for paroxysmal AF patients (78.2% [47/60], 60.0% [3/5], no data for convergent procedure, p=0.325).
Table 3.
| First Author |
No. patients |
AF type: PAF/PrAF/LSPrAF |
Procedure time (min) |
Hospital stay (days)* |
Death (N) |
Death or Major Complication (N) |
Acute non-fatal thromboembolism (N) |
Major Surgical Complications (non-embolic, non fatal) (N) |
No. with minimum 12-month FU |
Confirmation of AF recurrence |
12-month AAD-free SR maintanance – All (N) |
12-month AAD free FU for PAF (N) |
12-month AAD free FU for PrAF/LSPrAF |
| Thoracoscopic Clamp-based Approach |
|
|
|
|
|
|
|
|
88.1% |
78.3% |
88.2% |
| Mahapatra57 |
15 |
0/9/6 |
Both components: mean 450±20 |
median 5.0 (IQR 5.0–5.5) |
0 |
0 |
0 |
None |
14 |
7 day event monitor, AF >30 secs |
13/14 |
- |
13/14 |
| Lee56 |
7 |
NA |
NA |
median 5 (IQR 4-6)* |
0 |
1 |
0 |
1 prolonged ventilation postop* |
NA |
Continuous ECG monitoring (duration and criteria not stated) or pacemaker/ICD monitoring |
(12/23)$ |
NA |
NA |
| Pison33 |
26 |
15/10/1 |
Both components: mean 280±84 |
mean 7±2 |
0 |
2 |
0 |
1 pleural effusion requiring drainage, 1 surgical incision pain prolonging hospital stay |
24 |
7-day Holter monitoring, AF/AT >30 secs |
20/24 |
11/15 |
10/11 |
| La Meir62 |
35 |
16/8/11 |
Both components: median 268 (IQR 186–477) |
median 3.4 (IQR 2.6–4.1) |
0 |
0 |
0 |
None |
35 |
7 day Holter, AF/AT >30 secs |
32/35 |
14/16 |
16/19 |
| Kurfirst63 |
30 |
0/0/30 |
Surgical component: mean 210±30 |
mean 4.5±3 |
0 |
5 |
0 |
2 left pulmonary artery bleeding requiring sternotomy, 2 phrenic nerve palsies persistent at 12 months, 1 tamponade postop day 24 with overanticoagulation |
0 |
7 day Holter, AF/AT >30 secs |
(27/30 at mean 208±29 days) |
- |
(27/30 at mean 208±29 days) |
| Lee64 |
10 |
1/0/9 |
Surgical component: mean 221 |
median 12 |
0 |
3 |
1 stroke |
1 reexpansion pulmonary edema and pneumonia, 1 pericardial effusion |
0 |
Holter (duration not specified) AF/AT >30 secs |
(10/10 at median 7.6 months [range 6.7 - 11.6]). |
NA |
NA |
| Pison65 |
78 |
29/34/15 |
NA |
median 6 (IQR 5.5-8) |
0 |
6 |
0 |
1 reoperation for bleeding, 1 bleeding not requiring reoperation, 2 pneumonia, 2 complete heart block requiring pacemaker implantation |
78 |
7 day Holter, AF/AT >30 secs |
68/78 |
22/29 (76%) |
43/49 |
| Thoracoscopic Encircling Catheter - based Approach |
|
|
|
|
|
|
|
73.4% |
60.0% |
74.6% |
| La Meir59 |
19 |
5/4/10 |
Both components: median 216 (IQR 132–391) |
median 3.6 (IQR 2.7–4.3) |
0 |
0 |
0 |
None |
19 |
7 day Holter, AF/AT >30 secs |
7/19 |
3/5 |
4/14 |
| Bisleri60 |
45 |
0/0/45 |
Epicardial component: mean 85±9 |
mean 3.9±1.4 |
0 |
0 |
0 |
None |
45 |
ILR, AF>5 min or overall AF burden >0.5% |
40/45 |
- |
40/45 |
| Subxiphoid Convergent Approach |
|
|
|
|
|
|
|
|
59.3% |
- |
51.5% |
| Gehi61 |
101 |
17/37/47 |
NA |
mean 4.4 |
2# |
7 |
1 TIA |
2 retroperitoneal bleeding, 2 tamponade |
69 |
24 hour Holter, AF/AT >30 secs |
46/69 |
NA |
NA |
| Gersak66 |
73 |
0/22/51 |
Surgical component: 112±38 |
NA |
0 |
8 |
1 stroke |
2 bleeding requiring sternotomy, 2 bleeding not requiring reoperation, 1 tamponade, 1 pericardial effusion, 1 pleural effusion |
66 |
ILR (n=48/73) or Holter (24 hours or 7 days), criteria not stated |
34/66 |
- |
34/66 |
| TOTAL** |
432 |
83/124/225 |
|
|
2 |
32 |
3 |
27 |
350 |
|
260 |
50 |
160 |
| % of TOTAL |
|
|
|
0.5% |
7.4% |
0.7% |
6.3% |
81.0% |
|
74.3% |
76.9% |
73.4% |
Major complications (Table 3) were death (n=2, both with convergent approach), thromboembolic (n=3, of which 2 were with convergent approach, none fatal) and non-thromboembolic complications (n=27), consisting of 10 thoracic or retroperitoneal bleeds with or without rescue sternotomy, 6 tamponade/pericardial effusion, 2 complete heart block requiring pacemaker implantation, 2 phrenic nerve palsy, 2 pleural effusion, 4 respiratory complications and 1 with incisional pain delaying hospital discharge. Rate of death or non-fatal major complications were 7.4% overall, 8.5% with the bilateral thoracoscopic clamp-based approach, 0% with the thoracoscopic suction encircling catheter-based approach and 8.6% with the convergent approach (Table 3). Average length of hospital stay, when reported, was between 3.6 and 7 days (average for the three different approaches 5.6 vs. 3.8 vs. 4.4 days respectively, Table 3).
Hybrid Ablation vs. Sequential Catheter Ablation
For endovascular catheter ablation of paroxysmal AF, 18-month freedom from arrhythmia recurrence and antiarrhythmics was reported in 75% of 9,590 patients in a worldwide survey of 182 centers from 24 countries treated between 2004-6.376 Results at 5 years are 47-78% after the first procedure99,176,177 and 75-92% after repeat procedures.99,100,176,177 In most cases, recurrence is due to recovered conduction at a prior ablation site.99,177 A 12- to 24-month success rate of 73-92% has been reported from contemporary catheter ablation techniques to prevent late reconnection of pulmonary veins, which include using a force-sensing catheter (SmartTouch, Biosense Webster, Inc., Diamond Bar, CA) to ensure adequate contact force during ablation, a second generation cryoballoon catheter designed for better contact and surface temperature distribution (Arctic Front Advance, Medtronic, Minneapolis, MN), using failure to capture as an ablation endpoint, and incorporating a wait period and adenosine to identify reversible injury and unmask latent conduction.326,329,331,377-379 It is unknown whether these strategies will be subject to similar rates of late attrition in success seen with earlier approaches.177
With persistent and long-standing persistent AF, endovascular catheter ablation yield sinus rhythm maintenance off antiarrhythmic medication in 35-77% at 12 months after a single procedure122,129,238,240,242 and 64-79% at 18-24 months after repeat procedures.129,242,243,376 Patients with persistent and long-standing persistent AF have a higher rate of late attrition than with paroxysmal AF,380 with reported 5 year success rates of 45-81%.99,129,381,382
Complications of endovascular catheter AF ablation were seen in 6.3% of an estimated 93,801 procedures performed between 2000-10 in the National Inpatient Sample database.383 Complications were cardiac in 2.5%, including 1.5% pericardial and 0.3% requiring rescue cardiac surgery, respiratory in 1.3%, postoperative hemorrhage in 3.4%, vascular complications in 1.5%, and neurological (thromboembolic) in 1%. In-hospital mortality was 0.5%. In the California State Inpatient Database, complications after first AF ablation between 2005-8 were seen in 5% of 4,156 patients, most commonly vascular.384 The world-wide survey reported major complications in 4.5% of 20,825 catheter ablation procedures on 16,309 patients between 2003-6.376 Complication rates were low in other large cohorts with patients undergoing multiple procedures (3.3% of 1,404 patients, 20% had repeat ablation;99 5.2% of 1,220 patients, 27% had repeat ablation176). Rates of pulmonary vein stenosis are 0.3-1.3% and atrio-esophageal fistula are 0-0.04%.99,176,376 Studies reporting on the second generation cryoballoon ablation have reported higher rates of right phrenic nerve palsy (3.5-5.6%) than catheter radiofrequency ablation.378,379 Cost-effectiveness analyses of endovascular catheter ablation in various developed countries’ healthcare models have demonstrated reasonable cost-effectiveness in patients who have paroxysmal AF, with improved quality of life and avoidance of future health care costs,385,386 including when utilized as a first-line approach in younger patients,387 although are sensitive to AF recurrence rates and impact on stroke risk.388-393
The FAST trial compared bilateral thoracoscopic epicardial ablation to endovascular catheter ablation, randomizing 124 patients with drug-refractory non-valvular AF (67% paroxysmal, 33% persistent, CHADS2 of 0 or 1 in 90%) to either surgical PVI using a bipolar radiofrequency clamp with intraoperative confirmation of block, LAA staple excision, ganglionated plexi ablation, ligament of Marshall transection and optional additional linear ablation (31%), or endovascular antral radiofrequency PVI with optional additional linear ablation (50%).394 More patients in the surgical group were free from recurrent atrial arrhythmia off antiarrhythmics at 12 months (overall: 66 vs 37%, p=0.002; paroxysmal AF: 69 vs 35%, p=0.005; persistent AF: 56 vs 36%, p=0.341). It is unclear whether the difference in success was due to more durable lesions or the more diverse ablation targets with surgical ablation, but the results should be interpreted in light of the higher proportion with persistent AF in the endovascular catheter ablation group (41 vs 21%) and lower success rate of catheter ablation in comparison to the published contemporary data above, particularly with paroxysmal AF. There were more frequent procedural complications (23 vs 3.2%) and fewer thromboembolic events at 12 months (0/61 vs 2/63), with surgical ablation preventing an arrhythmia recurrence for every 3.4 and causing an additional complication for every 5.1 procedures.394 The procedural complication rate was higher than that of the published hybrid ablation literature summarized above (7.4%).
To compare hybrid ablation with repeat catheter ablation, Mahapatra et al57 matched their hybrid ablation group of 15 persistent and long-standing persistent AF patients to a control group of 30 long-standing persistent AF patients undergoing repeat catheter ablation, matching for left atrial size, duration and type of AF, lack of prior cardiac surgery, left ventricular ejection fraction and use of antiarrhythmic medications. The hybrid group had bilateral thoracoscopic clamp-based approach with delayed staged endovascular ablation at 4.3±1.3 days, multiple linear ablation sets, ganglion ablation, ligament of Marshall ablation, LAA excision, coronary sinus ablation and CFAE ablation. The catheter ablation group all had antral isolation, roof line, cavotricuspid isthmus line and optional mitral isthmus line (17 cases), coronary sinus ablation (9 cases), SVC isolation (11 cases) and CFAE ablation (12 cases). After a mean follow-up of 21 months, 87% (13/15) of hybrid ablation and 53% (16/30) of catheter-alone patients were free of atrial arrhythmia off antiarrhythmics. Repeat ablation was performed in 0/15 hybrid ablation and 3/30 catheter-alone patients.
In summary, the fundamental principle underlying hybrid ablation in assessing the eletrophysiological effects of lesions and ensuring that targets are ablated to specific endpoints to improve outcomes is incontrovertible. However, there is limited evidence supporting the concept that a multidimensional intervention targeting all possible arrhythmia mechanisms for all patients in the same sitting will result in superior results, even when these lesions are reinforced from both epicardial and endocardial sides to maximize the chances of sustained conduction block. Hybrid ablation procedures are associated with increased complications and longer post-procedural hospital stay, whilst cost-effectiveness studies have been limited by the lack of long-term outcome data.395 Studies directly comparing hybrid with endovascular catheter ablation have had small numbers, differences in patient characteristics and ablation targets, variable periprocedural antiarrhythmic and anticoagulant management, different methods for identifying recurrence arrhythmia, and have not incorporated recent advances in endovascular ablation practice offering more durable lesions or better identifying individual-specific mechanistic targets, an understanding of which has implications on long-term tailored approaches. Outcome data from contemporary endovascular catheter approaches suggest similar success rates to hybrid ablation, both for paroxysmal and persistent patient groups, particular when repeat catheter ablations are accounted for. When considering the hybrid approach, matching intervention to mechanism is key for identifying targets, ablation endpoints, and the specific advantage over the endovascular approach for the patient at hand, balanced against the increased procedural complexity, more complications some of which are life-threatening, and longer hospital stay.
Hybrid Ablation vs. Cut-and-Sew Maze
Since the first description of the ablation-assisted open surgical maze yielding similar short-term outcomes to the traditional cut-and-sew technique, 5 others have reported that the traditional approach yields superior long-term outcomes, with hazard ratio for recurrent arrhythmia of 0.40 up to 5 years and 0.23 beyond 5 years.396 In a meta-analysis of 16 randomized trials, the cut-and-sew approach was associated with higher sinus rhythm prevalence and lower stroke rates outcome compared to ablation-assisted approaches.397 Lee et al compared 25 hybrid ablation patients (bilateral thoracoscopic clamp-based) to 38 cut-and-sew maze patients and reported 1 year freedom from AF and antiarrhythmic medication in 52% and 87.5%, respectively (p=0.004), even though the cut-and-sew group had more with long-standing persistent AF (40 vs 16%).56 However, in their hybrid group, only 7 patients followed through with the endovascular catheter ablation component. There were more frequent complications in the cut-and-sew group (18 vs 4%). A systematic review comparing minimally invasive endocardial Cox-maze, minimally invasive epicardial ablation and hybrid ablation reported operative mortality at 0%, 0.5% and 0.9%; perioperative permanent pacemaker implantation in 3.5%, 2.7% and 1.5%, rescue median sternotomy in 0%, 2.4% and 2.5%, reoperation for bleeding in 1.0%, 1.5% and 2.2%, mean length of stay of 5.4, 6.0 and 4.6 days, and 12-month maintenance of sinus rhythm off antiarrhythmics in 87%, 72% and 71%, respectively.28
Immediate vs. Delayed Staged Hybrid Ablation
There is limited published data allowing direct comparison of immediate to delayed staging of the endovascular component of hybrid ablation. Immediate staging requires a laboratory hosting both surgical and electrophysiological setups, careful management of intraprocedural anticoagulation with transeptal and endoscopic accesses, and the available time and resources to complete both interventions in the same sitting. Delayed staging, where endovascular testing and ablation has been performed days to months after minimally invasive epicardial ablation, allows healing of the surgical wounds and time for reversible injury from ablation to abate and reconnections to establish, and has been shown to increase the likelihood of discovering PV reconnection during endocardial mapping versus a same day procedure (48% vs 14%).398 It can be performed in separate surgical and electrophysiological laboratory setups. Patients may prefer a procedure where both components are completed in the same sitting or during the same hospitalization.
Atrial fibrillation ablation offers considerable benefits to patients towards symptom control and quality of life improvement.75 The multiplicity and progressive nature of AF mechanisms and recovery of conduction may account for progressive attrition in maintaining sinus rhythm with long-term follow-up.129,380 The pioneering developments that have led to the various hybrid ablation approaches are an opportunity in properly selected patients without having to recourse to open heart surgery. The choice of procedural approach utilized for hybrid ablation is important, given the difference in possible lesion sets, success rates, complications, adjunctive LAA closure and access to adjunctive ablation targets. However, randomized trial data are lacking and long-term efficacy is unproven. The PRHACA (Prospective, Randomized Comparison of Hybrid Ablation vs. Catheter Ablation) trial (clinicaltrials.gov/ NCT02344394) is an investigator sponsored trial which is currently recruiting patients with persistent AF to test the nContact system (convergent approach). The CONVERGE (Epi/Endo Ablation For Treatment of Persistent Atrial Fibrillation) trial (clinicaltrials.gov/NCT01984346) is an industry sponsored trial which is also recruiting persistent AF patients to test the nContact system. The SCALAF trial (clinicaltrials.gov/NCT00703157), which aims to compare efficacy of minimally invasive surgical and catheter-based PVI, is underway. Another active trial (clinicaltrials.gov/NCT02392338) is comparing hybrid ablation with minimally invasive thoracoscopic ablation alone in persistent AF.
A promise of progress comes from an improved understanding of how anatomical substrate relates to electrophysiological observations, better catheters and mapping technologies, novel energy sources, adequate management of recurrences, and identifying and treating underlying clinical risk factors. Whether hybrid ablation will add to this remains to be seen. In the absence of robust efficacy data, and given the increased risk of complications, associated morbidity and length of hospital stay as compared to catheter ablation, caution should be exercised in adopting this approach universally. The present data suggest that, perhaps, with appropriate patient selection, accurate identification of patient-specific mechanisms and targets, and selection of optimal access to maximize anatomical vantage to these targets, this novel approach may have a role in specific situations. It may be better suited as a concomitant procedure during cardiac surgery for other reasons, for example patients requiring thrombectomy or LAA closure. Alternatively, it may help translate novel therapeutic pathways to practice, such as controlled delivery of genetic vectors influencing arrhythmia mechanisms399-401 or humeral mediators governing response to injury.402-404






