Very Long-Term Results Of Atrial Fibrillation Ablation Confirm That This Therapy Is Really Effective
Cristina Tutuianu,MD, Judit Szilagy MD, Robert Pap, MD, PhD, László Sághy, MD, PhD.
2nd Department of Medicine and Cardiology Center, Electrophysiology Division, University of Szeged, Szeged Hungary.
Catheter ablation -in general- is a highly effective and “curative” intervention for a broad spectrum of supraventricular and ventricular arrhythmias. After a successful procedure eliminating a simple arrhythmia substrate, the recurrence rate is low and the short term success correlates well with the long term freedom from the arrhythmia.
Correspondence to: Dr.Tutuianu Cristina,2nd Department of Medicine and Cardiology Center, Electrophysiology Division, University of Szeged, Szeged Hungary.
Since the identification of trigger activity in the pulmonary vein by Haissaguerre et al,2 catheter ablation of atrial fibrillation (AF) has became an established therapeutic modality for the treatment of patients with AF. Published data in the literature suggest that success rates following ablation of AF are relatively favorable (50-70%)3,4,5 but most studies have reported limited follow-up of 1 or 2 years after the first ablation and the long-term outcomes have not been fully elucidated.
Why do we need more information regarding the long term follow up data following AF ablation, in contrast with conventional ablation procedures?
First, the clinical significance of an AF recurrence is usually more pronounced than other arrhythmias because of the well known deleterious consequences of this arrhythmia, with special attention to thromboembolic complications.
Furthermore, the pathologic mechanism of AF is complex with a special interplay between the triggering structures and a continuously evolving left atrial substrate. Consequently, it is important to analyze the long term response and define the durability of different ablation techniques to achieve a better clinical outcome.
Pulmonary vein isolation (PVI) is the mainstay therapy of paroxysmal AF, but its success is suboptimal in the persistent population.5,6 Additional ablation techniques have been introduced during the last decade.5 The AF population is very heterogeneous, with respect to duration and type of arrhythmia, comorbidities etc. On top of that, ablation results may depend on different definition of success,and follow up methods. Consequently, a comprehensive discussion of long term outcome of catheter ablation should include parameters like type of AF, ablation strategies, the use of antiarrhythmic drugs after ablation, multiple procedures, success definitions, the frequency and intensity of arrhythmia monitoring. The aim of the current study is to review the literature and evaluate the very long term success of catheter ablation of AF.
Definition Of Long Term Follow Up
In the 2012 Expert Consensus on catheter ablation of atrial fibrillation,7 late recurrence of AF is defined as a recurrence after 12 months or more after AF ablation and the long term success is defined as freedom from AF following the 3 months blanking period through a minimum of 36 months There is also consensus that all patients who undergo catheter ablation of AF should be controlled every six months for at least two years. In our review, we defined very long term follow up to be longer than 3 years after the index procedure
Depending on whether patients have paroxysmal (PAF), persistent, or longstanding persistent AF, the outcome of ablation procedures differs considerably. A systematic review and meta-analysis including 17, mostly retrospective studies published by Ganesan et al8 demonstrated that the single procedure success for PAF was 68.6 % at 1 year, 61.1% at 3 years and 62.3% at 5 years. After multiple procedures (average 1.45 procedure per patient) 79% of patients were free from AF at 5 years follow-up. Comparing patients with persistent and long-standing persistent AF after a single procedure the results were less favorable, 50.8% at 1 year, and 41.6% at 3 years. After multiple procedures, the success was definitely more promising in this population, 77.8 % in the long term, but only few studies reported the outcome of AF ablation after more than 3 years suggesting that we need more data to definitively assess the very long term efficacy of ablation in persistent atrial fibrillation. The authors concluded that
both single and multiple procedure success rates showed adequate
stability over 3 years with a significant residual risk for a recurrence
and the paroxysmal cohort demonstrated a superior single procedure
efficacy. Tzou et al9 reported an AF freedom, off AAD, of 85% at 3
years and 71% at 5 years, with a 7% per year late recurrence after the
first ablation in a mixed paroxysmal and persistent AF population. In
a multivariate analysis, persistent AF was an independent predictor
for recurrence.
Recently, Steinberg et al.10 published a large prospective cohort
of AF population (72% paroxysmal, 28 % persistent) and followed
445 patients for even a decade after a 1 year complete success
following PVI. During a 62 months median follow up, 22 % of
patients developed very late arrhythmia recurrence, and the authors
demonstrated that the slope of the recurrence curve declined linearly.
When they analyzed the differences in outcome on the basis of the
arrhythmia pattern before the index ablation procedure, the results
were strikingly different. The recurrence rates at 2, 5, an 10 years
were 3%, 11%, and 27 % vs 13%, 29%, and 62% for paroxysmal
and persistent AF patients, respectively (P< .0001). The authors
concluded that the majority of AF patients did quite well over the
time, and the ablation results are sustainable even for the long term
as well, but using multivariate analysis, persistent AF (hazard ratio
3.08; P< .0001) was an independent risk factor for recurrence of AF.
An interesting question concerning the long term recurrence and
efficacy of the ablation procedure whether these interventions can
prevent progression of the arrhythmia from paroxysmal to persistent
form. In the study of Takigawa et al3 during a median follow up
of approximately 48 months, AF progressed from paroxysmal
to persistent in 1.2 % of patients in accordance with previous
investigations where the AF progression rate was similar (1.5%
-3%).11,12 In contrast, the results of pharmacologic therapy are
definitely worse, the reported rates vary between 5.5% and 15%/
year.13,14 These observations suggest that the interventional therapy
is better than drugs alone for preventing AF progression, which is
an important aspect of long term consequences of the arrhythmia.
Impact of Ablation Techniques
Whereas a consensus has been reached on the suitable approach for
ablation of patients with paroxysmal AF,7 no such consensus exists
for patients with persistent and long lasting persistent AF regarding
the optimal technology of treatment.
Numerous clinical trials demonstrated that the main mechanism of AF recurrence after PVI in the paroxysmal population is the
resumption of electrical conduction between the veins and left atrial
muscle. This statement is true for either the short or the long term
recurrences (see below).8,15 Based upon these observations we should
assume that at least in PAF, the durability of venous isolation and
therefore permanent electrical disconnection plays a crucial role in
maintaining procedural effectiveness in the long term. Accordingly,
any kind of procedural tool or technique which can facilitate the durable isolation of pulmonary veins can be useful.
Segmental PV ablation or wider continuous circumferential
antral ablation, two different procedures which have been used most
commonly in clinical practice showed different outcomes. Sawhney
et al16 reported that 86% of the patients were free from AF at 1
year follow up after segmental pulmonary vein isolation, with 79%,
and 56% free at 2 and 5 years respectively. A meta-analysis done by
Proietti at al17 including12 studies that compared the effectiveness of
wide antral versus segmental pulmonary vein isolation concluded
that PVI performed with a wide antral approach is more effective
than ostial PVI in achieving freedom from atrial tachyarrhythmia
recurrence at long-term follow-up (OR, 0.33; 95% CI, 0.24-0.46; P<
.00001). They excluded the studies in which electric isolation was not
assessed or if different catheter technologies were used. Ganesan et
al8 also investigated if there is a statistical difference in outcomes of
segmental PV isolation compared with wide antral circumferential
ablation. The conclusion here was no, but they included also the
studies with wide circumferential ablation without assessing the
isolation of the pulmonary veins.
An alternative energy source that has been developed to overcome
some of the disadvantages of radiofrequency ablation is cryoenergy
using a balloon based technology. A comparison (1:1 propensity
score match) between cryoballoon and radiofrequency ablation
showed similar long term success rates with a recurrence rate of 45
% in both groups after a two-year follow-up 18. Neumann et al19
reported freedom from AF in 74% of patients with paroxysmal AF
and 42% with persistent AF, but the follow up time was shorter.
Cryoablation is a new technology and it is under continuous
development, but whether it can improve very long term outcomes
has to be investigated in the future.
As mentioned earlier, in patients with persistent and longstanding
persistent AF the data concerning the outcomes are considerably less
favorable than for PAF. The wide contrast in PVI success rates between
paroxysmal and persistent AF suggested that the mechanisms can be
substantially different, and probably related to electrophysiological
and structural remodeling of left atrial substrate. Not surprisingly,current approaches designed to target persistent AF are mainly
based on modification of the atrial substrate, but exhibit remarkable
differences, and a widely accepted uniform strategy is missing.
Different ablation strategies, including the ablation of complex
fractionated atrial electrograms (CFAEs),20 linear lesions in the left
atrium,21 ablation at the maximal high dominant frequency spots22,
rotor ablation23 have been developed as an add-on to pulmonary
vein isolation to improve the outcome in this group. PVI alone can
be sufficient to maintain sinus rhythm in 21% of patients after a
single procedure and in 43.2% after 1-3 procedures in a retrospective
analysis.6 The same 21-22% success with a single procedure and 37-
43% success rate after repeat procedures was published by Brooks
at al5 in a review of 32 studies. They also reported the success rate
of other techniques: linear ablation in addition to PVI (11-74%),
posterior wall isolation (42-50%) CFAE ablation (36-68%) or
“stepwise” ablation approach (38-62%). The integration of repeat
procedures and addition of previously ineffective antiarrhythmic
drugs further improved clinical success. The variation in the success
rate suggests that the best approach in this group is still unclear.
However, persistent and long-standing persistent AF can be treated
with a relatively high success rate during rather a medium term
follow up, since really long term data are still lacking.
Our approach is wide area antral circumferential ablation
for paroxysmal and persistent patients as well, with complete
isolation of pulmonary veins, without creating additional lesions
in the left atrium. During the procedures we use open irrigation
radiofrequency catheters and a combination of EAM and intracardiac
echocardiography
(Figure 1) to enhance the anatomical orientation
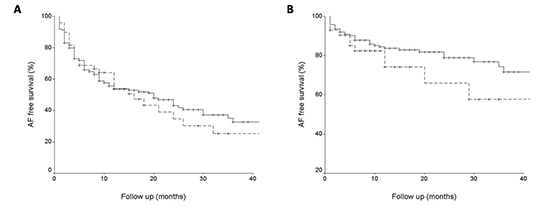
and the monitoring of catheter-tissue contact. After a mean of 18
months follow up time the recurrence rate after single procedure
was 52% and 61%, after multiple procedures was 19% and 29%, in a
paroxysmal and persistent cohort respectively
(Figure 2).
Figure 1. Antral isolation of the left and right pulmonary veins guided by intracardiac echocardiography. Panel A: Lasso catheter was placed in the left common ostium between the left inferior and superior pulmonary vein (white arrow). Panel B: Ablation catheter (white arrow) is touching the right venous carina next to the right inferior pulmonary vein. LSPV: left superior pulmonary vein, LIPV: left inferior pulmonary vein, RIPV: right inferior pulmonary vein, Sept: interatrial septum. Images are originating from the database of Szeged University.
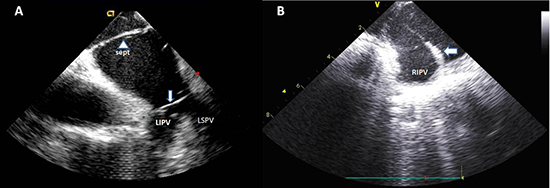
Figure 2. Kaplan-Meier curve representing the arrhythmia free survival after single ablation procedure (Panel A) and following multiple ablation procedures (Panel B) in patients with paroxysmal (solid lines) vs persistent atrial fibrillation (broken lines). Data are originating from the database of Szeged University
Impact of Follow up Techniques
Apart from the above mentioned factors, the varying results reported by those studies could be attributed to substantial differences in follow up methods. During the first year, the majority of studies performed clinical examination, electrocardiogram and 24-hour Holter monitoring or event recorders at 3, 6, and 12 months. Beyond the first year, the intensity of follow up is usually reduced to 1 or 2 outpatient visits per year or even based on data from referring clinicians.24 There is a clear positive correlation between the duration and intensity of the follow-up and the arrhythmia detection rate.25 For the short term follow up, 7 day Holter and transtelephonic monitoring are proven to be effective to detect asymptomatic AF episodes. Piorkowski et al.25 showed that using serial 7 day Holter
and transtelephonic monitoring, the „real” procedural success rate decreased from 70% to 50% and 45 % respectively.
The definition of long term ablation success remains controversial
because current post ablation rhythm monitoring strategies are
based on symptom and/or intermittent ECG recordings and thus
probably underestimate the real rate of AF recurrences.26 Continuous
monitoring like implantable loop recorders are useful tools27 but to
put these devices into an everyday practice is limited by cost, patients
compliance and high burden of false detection.
Predictors And Mechanism Of Recurrence
As we suggested earlier, the success of catheter ablation may
depend on technical aspects of the procedure but also on patient related factors. Patients in whom AF recurred, exhibit specific clinical
characteristics which can be considered as independent predictors of
late AF recurrence. Some studies reported history of persistent AF
as a predictor of very late recurrence8,9,10 while other studies found
that there was no significant association between the AF type and
risk of recurrence.15,28 The heterogeneity in results across the studies
can be explained by the heterogeneous definition of AF type and
the differences in terminology pertaining to “long term” follow up.
The duration of AF history is a very important predictor of AF
recurrence,3 but other studies could not find a significant association
between AF duration and AF recurrence.29,30 A possible explanation
is that duration of AF does not necessarily correlate with the length of
the AF episodes and may not reflect the extent of atrial remodeling.31
Other commonly identified predictors of AF recurrence are age >
65 years, left atrial diameter >24mm/m²,31 left ventricular systolic
dysfunction, heart failure, structural or valvular heart disease,8
hypertension and hyperlipidemia.15 These observations indicate the
role of enhanced vulnerability of left atrial myocardium induced
by these factors beyond the importance of trigger mechanism.
Aggressive medical treatment of these conditions and risk factors
reduction32 may improve the efficacy of AF ablation. Pathak et
al32 reported in a recent publication that risk factor management
according to American Heart Association/American College of
Cardiology guidelines significantly improved the outcome of AF
ablation in terms of AF burden and also generated favorable changes
in cardiac remodeling.
The main mechanism of the early recurrence following atrial
fibrillation ablation is the reconnection of previously isolated
pulmonary veins. In contrast, in patients with very late recurrence
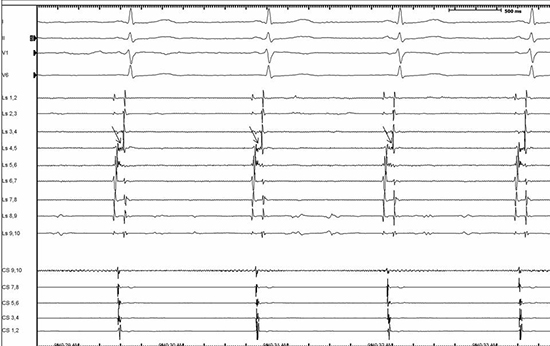
the mechanism is not completely elucidated. Lin et al33 found that
the majority of patients with recurrent AF undergoing a 3rd or more
procedure after a mean follow up of 36±22 months (range 12 to 119
months) had reconnected pulmonary veins with triggers originating
from the culprit PVs. (Figure 3) . However, in 20% of patients, new
non-PV triggers were identified at the time of 3rd or 4th procedure and the majority of non-PV triggers were mapped in the right
atrium or coronary sinus. Steinberg at al10 also found that in patients
undergoing reablation for very late AF recurrence, just 4% of PVs
were completely isolated. Conversely, Sotomi at al34 found that the
prevalence of PV reconnections and trigger PV reconnection were
significantly lower in the very late recurrence group (>12 months,
69%) than in the late recurrence group (3-12 months, 90%) and also
more patients required non-PV trigger ablation. In accordance with
this observation, Kurotobi at al35 demonstrated that the presence of
residual arrhytmogenic non-PV foci are associated with an increased
long term recurrence rate after successful isolation of PVs and left
atrial linear lesions in a long-standing persistent AF population.
Figure 3. Late reconnection of the right inferior pulmonary veins in a 56 years old patient with PAF following 32 months the index PVI. Single ablation attempt at the level of earliest PV potentials on Lasso,4-5 bipoles (arrow) resulted immediate isolation of the vein. All of the other pulmonary veins were isolated. Surface ECG leads I, II, V1 and V6, together with intracardiac recordings from the Lasso catheter (Lasso) placed in the right inferior pulmonary vein, and from the proximal to distal coronary sinus bipoles (CS). Tracing is originating from the database of Szeged University
During the last decade, numerous data became available regarding
the long term efficacy of the interventional treatment of atrial
fibrillation. These data can be especially important for estimating
prognosis, evaluation of currently available ablation techniques,
and last but not least for the reimbursement policy of procedures.
If we summarize the results of mostly retrospective analyses, we
can conclude that long term freedom from AF is achievable and
maintainable over 2-3 years or even more with mild increases in
arrhythmia recurrence over the time. This statement is especially true
for the paroxysmal AF population, following initial PVI procedures.
Single procedure success rate is definitely lower in the long term, so
for achieving a durable result, multiple procedures have to be taken
into account. The success of an ablation procedure is less encouraging
in the persistent population, moreover there is no real consensus
regarding the best ablation strategy beyond PVI, to improve the long
term efficacy rate.
It is likely that the main mechanism behind very late recurrences
of AF is the PV reconduction and recurrent pulmonary vein triggers,
but progressive remodeling of left atrial substrate as well as non-
PV triggers can play an important role over time, especially in the
persistent AF population.
It should be noted that strict AF free success rates in both groups
probably underestimate the real long term clinical benefit of the
procedures if we focus on symptomatic improvement or fewer
hospitalizations. Furthermore, it can not be overemphasized that
studies demonstrating very different results regarding the outcome
of procedures are showing significant heterogeneity in terms of the
definition of success, methodology of follow up, and the applied
ablation technologies.






