Role of Echocardiography in Atrial Fibrillation
Ablation
Andrew C. Y. To MBChB, Allan L. Klein MD
CLEVELAND CLINIC, CLEVELAND, OH.
Radiofrequency catheter ablation is an increasingly adopted strategy for difficult-to-manage patients with atrial fibrillation. Echocardiography is the key imaging modality to assess left atrialstructure and function. In this review, the role of echocardiography in atrial fibrillation ablationbefore, during and after ablation is discussed. Currently established roles of echocardiography inpatient selection pre-ablation and peri-procedural guidance, as well as newer echocardiographic techniques including the assessment of atrial mechanics are reviewed in the context of atrial fibrillation ablation.
Correspondence to: Allan L. Klein, MD, Heart and Vascular Institute, Cleveland Clinic, 9500 Euclid Avenue, Desk J1-5,
Cleveland, OH 44195.
Atrial fibrillation (AF) is a common arrhythmia
associated with significant morbidity and mortality.
In recent years, radiofrequency catheter ablation
with the electrical isolation of the pulmonary veins is commonly performed for patients withparoxysmal and persistent AF who continue tobe symtomatic despite at least one Class I or
III antiarrhythmic medication.1 Restoration of
sinus rhythm after AF ablation significantly improvedsymptoms, exercise capacity, quality of
life and left ventricular (LV) function, even when
concurrent heart disease and ventricular rate
control had been adequate before ablation.2-3
Multimodality imaging is often employed to assess
patients undergoing ablation. However,
echocardiography remains integral in the assessment
of left atrial (LA) structure and function.
This review discusses the role of echocardiography
in AF ablation from pre-ablation, during and
post-ablation. This includes the initial evaluation
and patient selection, pre-procedural screening
for LA and LA appendage (LAA) thrombus, direct
visualization of anatomic landmarks during
ablation, assessment of ablation complications,
assessment of LA mechanics post-ablation
and risk stratification for thromboembolism.
Transthoracic echocardiography (TTE) is essential for the initial evaluation of patients with AF,
in most cases, before AF ablation is even consideredas a treatment option. The overall management strategy of AF depends on a variety of clinical factors, including the type and duration of AF, severity of symptoms, patient age, associatedcardiovascular disease and other concurrentmedical conditions. TTE provides information on the etiologies and predisposing factorsfor the AF, effect on the ventricular function,as well as prognostic information on the risk of recurrence and thromboembolic risk (Table 1).
Information on LV function impacts the choice
of appropriate pharmacological agents for both
rate- and rhythm-control strategies. Agents such
as beta-blockers including sotalol, and nondihydropyridine calcium channel antagonists should
be administered with caution in patients with severe LV dysfunction and heart failure. Impaired
LV systolic function is also an independent echcardiographic predictor of stroke in patients withAF, even after adjusting for other clinical features.4
Impact of LA Size and LV Function on Patient Selection for AF Ablation
Accurate assessment of both LA size and LV function provides essential information for patient slection and is an importantdeterminant of successful AF ablation
Marked LA dilation is associated with a lower
success rate of maintaining sinus rhythm after AF
ablation compared to patients with structurally
normal hearts.5 As a result, the lack of LA enlargement is an important component of the currentguideline recommendations for the use of AF ablation as an alternative to pharmacologic therapy in symptomic patients.3,6 Hence, accurate
measurement of LA size is crucial for the
decision-making on suitability for AF ablation.
LA size measurement is routinely performed by
TTE. LA anteroposterior dimension can be measured
by M-mode or 2D echo in the parasternal
long axis view. This method is convenient and
has been widely adopted in routine clinical practice.
However, LA volume measured by either
the ellipsoid model or the Simpson’s method is
a more reliable measure of true LA size than Mmode
LA dimension7 and is the recommended
method for the accurate assessment of LA size.8
Table 1. The role of TTE and TEE in the Pre-Ablation Assessment of Patients with AF
| Transthoracic Echocardiogram |
Transesophageal Echocardiogram |
| Underlying causes of AF:
• Valvular heart disease
• Ischemic heart disease
• Hypertensive heart disease
• Infiltrative disease
• Other cardiomyopathies
• Pericardial disease
• Congenital heart disease |
Exclusion of LA appendage thrombus:
• Prior to cardioversion
• Prior to AF ablation |
| Effect of AF on the LV:
• Tachycardia-induced cardiomyopathy |
Pulmonary vein anatomy and function:
• Variant PV anatomy
• Pulmonary vein stenosis |
| Guidance of treatment option:
• Rate control vs. rhythm control
• Anticoagulation |
|
| Prognostic information:
• Left atrial size |
|
To improve the accuracy of LA size measurement,
3-dimensional echocardiography (3DE), cardiac
computed tomography (CT) and cardiac magnetic
resonance imaging (CMR) have been studied. The
3DE measurements demonstrate favorable test-retest variability 9 and good agreement with CMR.
9-11 When these techniques are applied in the
context of AF ablation, LA size measurements by
3DE ,12-13 cardiac CT,14 and CMR15-16also show good correlation with subsequent proceduralsuccess. Among the newer techniques, 3DE
shows the most promise of adoption in routine
clinical practice as it is non-invasive, readily available,and can be added onto the routinely performed post-ablation 2DE examination. As will
be discussed later, 3DE also offers the possibility
of measuring LA volumes at different phases
of the cardiac cycle, yielding information on LA
phasic function. Nevertheless, it is worthwhile
to note that LA size measurements made by 2DE
tend to be lower than those of 3DE,9,17 cardiac
CT18 and CMR.19 The relative strengths
and weaknesses of various imaging modalities in
the valuation of LA size are outlined in (Table 2)
When AF ablation is first adopted, patients with
normal LV systolic function are initially selected.
However,there is increasing evidence that AF ablation benefits patients with impaired LV systolicfunction.2,20-22 Currently, task force consensus
guidelines suggest that selected symptomatic patients with heart failure and/or reduced ejection fraction could be considered for catheter AF abltion.1 In the aforementioned studies,the aveage pre ablation ejection fraction rangedfrom 33% to 41%. Several important observationscould be made including the fact that catheter AFablation is feasible without an increase in proceduralcomplication and that the efficacy of theprocedure in patients with impaired systolicfunc-tion is lower than in those with normal ventricularfunction with a higher recurrence rate. Nevertheless,AF ablation results in significant symptomaticrelief, improvement in quality of life, as wellas some recovery of cardiac function. Future studiesare likely to further clarify the relative efficacyand clinical benefits of ablation in patients withsignificant LA dilation and LV systolic dysfunction.
Table 2. Relative strengths and weaknesses of LA size assessment by various imaging modalities
|
Echocardiography |
Cardiac computed tomogra-
phy (CT)
|
Cardiac magnetic resonance
(CMR) |
| Strengths |
• Real-time imaging
• Widely available and low in cost
• Assessment of LA phasic volumes |
• Accurate assessment of true
LA volume
• Short scan duration |
• Accurate assessment of
true LA volume
• Assessment of LA phasic
volumes |
| Weaknesses |
• True LA volumes not obtained (unless
3D echo)
• Image quality limited by acoustic window |
• Radiation risk |
• Limited availability in
many centers
• Longer scan duration |
TEE and Exclusion of LA/LAA Thrombus
The pathophysiology of AF is complex and is iTransesophageal echocardiography (TEE) is a sensitiveand specific technique for detection of LAand LA appendage (LAA) thrombus23 and is currently the gold standard investigation for excluding thrombus prior to elective cardioversion and AF ablation24Fig.1. The sensitivity and the specificity of TEE for detecting LA thrombi are 93-100% and 99-100% respectively.25-26
TEE features associated with thromboembolism
include the finding of a LA or LAA thrombus,
reduced LAA flow velocity, severe spontaneous
echo contrast in the LA or LAA, and atheromatousdisease of the aorta.27-28 The finding of severe
spontaneous echo contrast, which is seen as echogenic swirling blood flow, reflects red cell and clottingfactor aggregation with slow moving bloodwithin the atrium. This, by itself, is not an absolutecontraindication to cardioversionorAFablation,29 althoughitisassociatedwithLAthrombusfomation,ahigherrisk ofthromboembolism,and increased cardiovascular mortality.30
LA and LAA thrombus is an especially impor-
tant issue for AF ablation because the procedure
not only involves manipulation of multiple cathetersinside the LA with the potential of dislodging
in situ thrombus, but also leads to substantial
areas of denuded LA endothelium that may becomea nidus for thrombus formation in the days
or weeks post-ablation. A recent study found a
prevalence of LA thrombus and sludge of 0.6%
and 1.5% respectively on routine of pre-ablation
TEE. The prevalence of spontaneous echo contrast
was as high as 35%. In this population, the
predictors of LA thrombus were found to be high
CHADS 2score, history of congestive heart failure,and left ventricular ejection fraction <35%.31 While it remains contentious whether TEEshould be routinely performed in all patients because of the low incidence of thrombus,32 the
recent task force consensus guidelines stated that
patients with persistent AF who are in AF at the
time of ablation should have a TEE performed
to screen for LA/LAA thrombus, regardless of
the adequacy of pre-ablation anticoagulation.1
Figure 1 Use of transesophageal echocardiography in diagnosis of left atrial appendage thrombus. A 49-year-old patient with severe mitral regurgitation from mitral valve prolapse. LAA thrombus (green arrow) is found on TEE (A, B), with surrounding spontaneous echo contrast (red asterisk) in the LAA (C).

Since cardiac CT is commonly performed immediatelybefore AF ablation to use the 3D dataset
in image integration with real-time electroanatomicdata during ablation, attempts have
been made to use CT to screen for LA thrombus.
Retrospective single centre trials have suggested
that a negative CT has a high negative predictive
value making it a potential alternative for excludingLAA thrombi before ablation.33-35 This issue
will need to be clarified in future studies.
TEE and Pulmonary Venous Anatomy
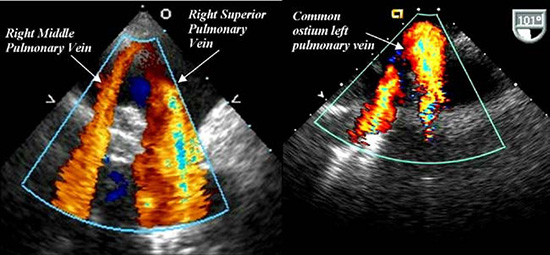
The accurate imaging of LA and pulmonary venous(PV) anatomy is important for understandingthe anatomic relationships between the PVs,LA and LAA. The most commonly seen pattern of PV anatomy is that of two separate right PVs and 2 separate left PVs. The right middle PV drains into the right superior PV before entering the LA.However, variations in PV anatomy are common.Supernumerary right PVs have an incidence of 1829%.36-41Common antrum of the left PVs results in a broad PV-LA junction and is found in6-35% of patients.42-43 Moreover,morphological remodeling of the PVs and LA can also be observed in patients with AF.StudieshavefoundthatPVostia are larger in AF versus non-AF patientsand those with persistent versus paroxysmal AF.36,40,44 The accurate uerstanding of these anatomicvariations is importantforlocalizationofthePV-LAinterfaceand the ridge between the PV and the LA appendage, so that variations in PV anato-my do not result in a higher recurrence risk.45
Cardiac CT and CMR are the gold standard investigationsfor accurate imaging of LA and PV
anatomy. TEE is not the first-line investigation for
this purpose mainly due to patient comfort, although TEEdoes excel in that it lacks radiationexposure and has a lower cost. Nevertheless, whenever TEE is performed pre-ablation for another
reason, valuable information on PV anatomy and
its variations could be gained, and all PVs should
be interrogated in detail as baseline information.
46-48 While some studies report that TEE can
only visualize two-thirds of superior and inferior
veins with experienced operators,49 the superior
and inferior PVs can be identified in over 94% of cases.47-48 The identification of PV anatomical
variations, such as common left PV antrum
and supernumerary right PVs, is slightly more
challenging compared to cardiac CT.47 In our
experience, careful rotation of the probe with the
veins in view should permit the visualization of
most veins. Useful techniques include imaging
the right PVs at 45-60° with a clockwise rotation
of the transducer and imaging the left PVs at 110°
with a counterclockwise transducer rotation.50
Figure 2 Examples of variant PV anatomy shown on TEE. Separate ostium for the rightmiddle and superior PV are noted in (a). Common ostium of the left superior and inferiorpulmonary veins is noted in (b). Reproduced with permission from Gabriel and Klein.75
Use of ICE During Ablation
During AF ablation, intraoperative TEE dramatically improves the visualization of anatomic landmarks over that of fluoroscopy. However,it is limited by patient discomfort and more importantly,
the need for airway management during
a prolonged procedure.51-53 Advances in
intracardiac echocardiography (ICE) performed
by electrophysiologists have improved both the
efficacy and safety of the procedure (Table 3).
Available ICE systems include those with mechanicalsingle-element transducers and phased-arraymulti-element transducers. A mechanical transducercontains a rotational single-element and produces high quality images but only at shallow
depths. To visualize LA structures, the transducer
has to be inside the LA. Phased-array multi-elementtransducers image at frequencies from 5.5-10MHz,providing 2D images with a deeper penetrationand allowing an RA-located ICE probe to imagethe LA without an additional transseptal puncture.
During an ablation procedure, ICE accurately
identifies key anatomic locations, such as the fossa ovalis, LAA, valve apparatus, pulmonary veins
and extracardiac structures. It facilitates transseptal
puncture, which is often challenging in
clinical scenarios, such as large septal aneurysm,
lipomatous atrial septal hypertrophy, double
membrane septum, prior cardiac surgery distorting anatomy, and previous surgical or percutaneousclosure of atrial septal defect or patent foramen
ovale. It determines the exact position of the
transseptal sheath by the tenting of the interatrial
septum and confirms access to the LA by the injectionof agitated saline. With ICE guidance, it is
possible to aim for a transseptal puncture in the
posterior region of the fossa ovalis. This is believed
to be safer than the more anterior portions as the
pulmonary veins are posterior structures.54
ICE provides real-time images of PV anatomy and
is far more sensitive to small movements of the
circular mapping and the ablation catheters than
fluoroscopy alone. Tissue contact is traditionally
monitored by stability of the ablation catheter on
fluoroscopy and stability of the electrical recording.The detection of microbubbles during ablation
with ICE indicates tissue superheating and
has been used to optimize ablation catheter placement.This strategy has been used to prevent tissue damage and scar formation, reduce the risk
of tissue superheating, optimize radiofrequency
energy delivery, and increase the number of lesions with optimal contact and energy delivery.55 Recent development in open irrigation platforms has lessened the importance of ICE in this
regard.56-57 However, recent research has investigated using ICE to monitor the relationship
between the catheter tip and adjacent structures,
such as the esophagus. This strategy may reduce
the incidence of esophageal injury.58-59
ICE is able to detect intra-procedural complica-tions promptly, similar to intraoperative TEE;
however, potential complications include cardiac
perforation and tamponade, thrombus formation
on the transseptal sheath and other catheters, as
well as pulmonary vein stenosis (PVS), which maybe predicted by an increase in PV flow velocitywith Doppler measured during the procedure.55
Table 3. The role of Intracardiac Echocardiography during AF Ablation
| Intracardiac Echocardiography
|
| Identification of key anatomic locations:
• Guidance of transseptal puncture
• Diagnosis of variant PV anatomy
Optimization of ablation catheter placement:
• Enhanced catheter-tissue interface
• Avoidance of tissue damage
• Visualization of the relationship between catheter tip ad esophagus
Diagnosis of intra-procedural complications:
• Cardiac perforation and tamponade
• Thrombus formation
• Early signs of Pulmonary vein stenosis |
Patients are followed clinically with varying use ofroutine imaging studies post-ablation amongst institutions.A summary of the role of TTE and TEE in
thepost-ablation patients is outlined in (Table 4).PVS is routinely screened for in some practices by cardiacCT,CMR,and/orTEE.TTEisalsosometimes
performed to document the degree of atrial remodeling and changes in LV function post-ablation.
TEE and the Diagnosis of PVS
Thermal injury to PV musculature results in PV
stenosis. The incidence of post-ablation severe
PV stenosis has been reported to be 3.4%.60
Symptoms of PV stenosis include shortness of
breath, cough, hemoptysis, chest pain, and recurrent lung infections.60-61 With the evolution
of techniques, the incidence of PV stenosis
has declined due to the avoidance of delivering
radiofrequency energy within the PV, together
with the increasing use of ICE and complementary image integration systems with pre-ablation
cardiac CT and real-time electroanatomical data.
While some institutions routinely screen for PVS
post-ablation, others perform imaging tests when
symptoms dictate them. It remains unclear whether early diagnosis and treatment of asymptomatic PVS provide long-term advantage, although asymp-tomatic PVS has the potential to cause progressivehypoplasia of the entire pulmonary vein proximal to the stenosis.62 Such pulmonary vascular occlusivedamage may not be fully reversible and may lead to difficulties with subsequent percutaneous
treatment should symptoms develop in the future.
The diagnosis of PVS is most commonly made
by tomographic modalities such as cardiac CT or
CMR, because they quantify the degree of PVS withexcellent reproducibility and demonstrate the relationship of the stenosis to the rest of the PV anatomyso percutaneous treatment can be planned.TEE, on the other hand, plays a supplementaryrole in the diagnosis of PVS and offers both anatomicaland functional information.PVscanbevisualizedin the great majority of patients studied,and PV ostial diameters at the venoatrial junctioncan be determined and compared with reference
vessel diameters to quantify the degree of narrowing.47 PV stenosis severity is defined according
to the percentage reduction in luminal diameter,
with a >70% luminal diameter reduction commonlyconsideredseverePVS.1 Anabsolutediameter
of<7mm mayalsobe sufficient to diagnosesignificant
PVS on TEE. When comparing TEE and cardiac
CT,two important aspects arenotable.Firstly,PVsare elliptical in shape with a larger diameterin the cranio-caudal axis than the transaxial axis;this is not as readily recognized by TEE. Secondly,TEE has the tendency to systematically underestimateostial diameters compared to CT. These aspects should be taken into account when serialstudies across different modalities are compared.
The unique feature of TEE in the diagnosis of PVS
is that it provides functional assessment of the PVs.
The use of color and pulsed Doppler assessment
of PV flow confirm the presence of hemodynamicallysignificant stenosis by detecting turbulence
and aliasing of the color Doppler signal as well as
an increase in pulsed wave Doppler diastolic flow
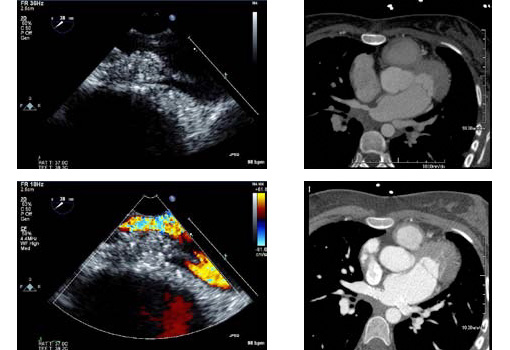
velocities (Fig.3). The optimal cutoff velocity for defining stenosis is currently unknown, althoughstudies have shown that a peak diastolic velocity of>100cm/s has a 86% sensitivity and 95% specificity for diagnosing PVS compared to the gold standard investigation of cardiac CT.63 It is important toremember that such comparison may not be valid,as functional information from TEE is not equivlent to anatomical information from cardiac CT,andthetwo modalities may supply incremental valuein selected cases. For instance, functional informationmay be important in assessing patients withequivocal symptoms and a moderate degree of stenosis.Information on the functional significance of stenosis may also be helpful over that of sizealone in determining the necessity of intervention.
Table 4. Role of Transthoracic and Transesophageal Echocardiography in the Post-Ablation Assessment of Patients with Atrial Fibrillation
| Transthoracic Echocardiogram |
Transesophageal Echocardiogram
|
| Atrial mechanics:
• Prediction of AF recurrence
• Assessment of post-ablation thromboembolic risk |
Pulmonary vein stenosis:
• Anatomical diagnosis
• Functional diagnosis – detection of turbulence, increased
flow velocities |
Atrial Mechanics – Prediction of Recurrence
AF results in electrical and structural remodeling
of the atrium 64-66 that can be considered part of
a rate-related atrial cardiomyopathy. The termination of arrhythmia may, as a result, lead to a degree of reverse remodeling of the atrial cardiomyopathy. The documentation of atrial reverse remodeling post-ablation may not routinely be performed in clinical practice, but studies have recently suggested a potential role in predicting recurrence postablation and stratifying thromboembolism risk.
Understanding atrial mechanics extends our current interest from simply measuring the maximum
LA volume at end-ventricular systole to measuring LA phasic functions (Table 5). Analyzing events at various phases of the cardiac cycle can supply information on the dynamic LA reservoir (atrial filling), conduit (passive atrial emptying) and contractile (active atrial contraction) functions
Although studies are sparse at the moment,it is likely that AF ablation has varying effects on the different components of LA phasic function.
Marsan et al. studied 57 patients with AF,43 ofwhom had paroxysmal AF.12 Atrial volumeswere studied at various phases of the cardiac cycle to assess LA phasic functions. In the patients who maintained sinus rhythm at 3 months, there was asignificant reduction in overall LA volume, with improvement in LA active contractile and resevoir functions. LA conduit function, or passiveemptying, was relatively unchanged, highlighting that LA phasic function analysis can study the effect of AF ablation on the LA in detail. Such changes were not observed in studies performed immediately after AF ablation, but rather took several weeks to occur. In the group that reverted back to AF, the changes of atrial reverse remodeling were not observed, illustrating that changes in atrial mechanics post-ablation could be used to predict future AF recurrence. Other studies using 3D echocardiography12-13 or CMR67-68 have also demonstrated post-ablation atrial reverse remodeling. The magnitude of change of the various
parameters is in the range of 10-20%. A lack of demonstrated atrial reverse remodeling has been
associated with post-ablation recurrence.12-13,68
Figure 3 PV stenosis on TEE. In this 22-year-old patient who underwent pulmonary vein isolation for AF, moderate ostial thickening is identified at the ostium of the right superior pulmonary vein (green arrow). (A) Turbulence is identified on color Doppler imaging suggesting functional significance. (B) Cardiac CT confirms the presence of severe PV stenosis of the right superior pulmonary vein (C), which is subsequently stented (D). In addition, the common antrum of the left pulmonary veins was also stenosed and stented (red arrow)
In addition to measuring phasic volumes, LA mechanics could also be studied with Doppler echocardiography. Traditionally, the measurement of
pulsed Doppler derived mitral A wave velocity and a’ from mitral annular tissue Doppler velocity
gives some insight into LA contractile function.Studies have found that a’ decreases immediately
after AF ablation but subsequently improves, suggesting that LA contractile function deterioratesimmediately post-ablation but recovers later.69
Recent research applies strain and strain rate imaging to study LA mechanics using either color tissue Doppler imaging techniques or 2-dimensional speckle tracking techniques.70-72 Using these techniques, changes in LA phasic functions pre- and post-ablation can be accurately quantified. Schneider et al.72 studied 118 patients with paroxysmal and persistent AF before and 3 months after AF ablation. Color tissue Doppler imagingmeasured the LA strain and strain rates at the reservoir,conduit and contractile phases of the atrial cardiac cycle, and was feasible in 97%. Changes in atrial myocardial properties post-ablation differed significantly between patients with paroxysmal and persistent AF. Recurrence is predicted by a lower post-ablation strain and strain rate during the LA reservoir phase, as well as a lower strain rate during the LA contractile phase. Such difference in atrial mechanics is not detected by conventional parameters of Doppler echocardiography, suggesting that strain and strain rate analysis appears more sensitive in investigating changes in LA mechanics after AF ablation. Studies have used 2-dimensional speckle tracking techniques to measure LA mechanics,70-71 although they have yet not been applied to the AF ablation population.
Atrial Mechanics – Thromboembolic Risk
The study of atrial mechanics may also be important for the prediction of thromboembolic risk. Currently, studies are sparse and the effect of changes in atrial mechanics post-ablation onthromboembolic risk is uncertain. Many patients
may opt for AF ablation as an alternative to longterm anticoagulation with warfarin therapy.73
However, this strategy cannot be recommended
at this stage because the impact of AF ablation on
thromboembolic risk remains unknown. While
some studies demonstrate an improvement in
LA function using 3-dimensional echocardiographic measurements,12-13 other studies have
shown that post-ablation LA reservoir and contractile functions remain significantly impaired,
especially when compared to patients undergoing
cardioversion and control subjects.74 Further
studies are required both to understand the
effect of AF ablation on LA mechanics and how
the changes in LA mechanics impact on thromboembolic risk. Such changes are likely to differ between patients with paroxysmal vs. persistent AF,
as well as with the number of prior AF ablations.
Current guideline recommendations for anticoagulation rely on pre-ablation risk factors. Postablation LA function changes have not been incorporated into the decision making process due to the lack of evidence. The guideline recommends that discontinuation of anticoagulation with warfarin therapy be avoided in patients with congestive heart failure, history of high blood pressure, age ≥75years, diabetes, prior stroke or transient CHADS2 score ≥2. In those with a CHADS2 score of 1 post AF-ablation, either aspirin or warfarin is thought to be appropriate.1
Table 5. Potentially Useful Measures of LA Mechanics
| LA phasic volumes |
LA maximum volume (end-ventricular systole)
LA pre-atrial contraction volume (start of atrial systole)
LA minimum volume (end-atrial systole) |
|
|
| LA ejection fraction |
Total LA emptying fraction (LA reservoir function)
Passive LA emptying fraction (LA conduit function)
Active LA emptying fraction (LA contractile function) |
| Doppler echo |
Mitral inflow E velocity
Mitral inflow A velocity
E’ mitral annulus tissue Doppler velocity
A’ mitral annulus tissue Doppler velocity |
| Strain (ε) |
εtotal (LA reservoir function)
εpositive (LA conduit function)
εnegative (LA contractile function) |
| Strain rate (SR) |
SRpositive(LA reservoir function)
SRearly negative(LA conduit function)
SRlate negative(LA contractile function) |
Echocardiography plays a central role in decision
making for patients undergoing AF ablation—preablation,during ablation and post-ablation. The role of echocardiography pre-ablation is now well established, in patient selection, screening of patients for LA/LAA thrombus prior to ablation, and the use of ICE in the guidance of catheter ablation.Emerging echocardiographic roles include the identificationof variant pulmonary vein anatomy, diagnosisof PVS, as well as the use of data from atrialmechanics studies in documenting atrial reverse remodeling and in prognosticating for AF recurrence and future thromboembolic events. The role of echocardiography will continue to evolve with the increasing use of AF ablation in AF management.
Dr. Andrew To acknowledges the support from the Overseas Fellowship Award from the National Heart Foundation of New Zealand. Both authors acknowledge secretarial support from Marie Campbell.
2DE: 2-dimensional Echocardiography
3DE: 3-dimensional Echocardiography
AF: Atrial Fibrillation
CMR: Cardiac Magnetic Resonance
CT: Computed Tomography
ICE: Intracardiac Echocardiography
LA: Left Atrium / Left Atrial
LAA: Left Atrial Appendage
LV: Left Ventricle / Left Ventricular
PV: Pulmonary Vein(s) / Pulmonary Venous
PVS: Pulmonary Vein Stenosis
TEE: Transesophageal Echocardiography
TTE: Transthoracic Echocardiography






