Effect of High-dose Telmisartan on the Prevention of Recurrent Atrial Fibrillation in Hypertensive Patients
Shingo Maeda1,4, Mitsuhiro Nishizaki2, Noriyoshi Yamawake2, Takashi Ashikaga2, Kensuke Ihara2, Tadashi Murai2, Hiroyuki Fujii2, Harumizu Sakurada3, Masayasu Hiraoka4, Mitsuaki Isobe4
1Department of Cardiology, Musashino Red Cross Hospital, Tokyo, Japan.2Department of Cardiology, Yokohama-Minami Kyosai Hospital, Yokohama, Japan.3Depatment of Cardiology, Tokyo Metropolitan Hiroo Hospital, Tokyo, Japan.4Department of Cardiovascular Medicine, Tokyo Medical and Dental University Graduate School, Tokyo, Japan.
Telmisartan has been shown to exert an equivalent action as ramipril on the prevention of cardiovascular events, but the dose-dependent actions of telmisartan on the prevention of events remain unknown.
We investigated the dose-dependent effects of telmisartan on the prevention of AF in patients associated with risk factors.
One hundred hypertensive patients were randomized to take 40 mg (low-dose group: n=57) or 80 mg (high-dose group: n=43) of telmisartan for 24 months. The primary endpoints were defined as a new development and/or recurrence of atrial fibrillation (AF).
The mean values of the blood pressure in both groups decreased significantly and to similar degrees after 24 months, in the low-dose (p < 0.01) and high-dose (p < 0.01) groups. At the end of the follow-up, the incidence of AF was lower in the high-dose group than in the low-dose group (p < 0.05). Moreover, the proportion of AF recurrences in the patients with a past history of paroxysmal AF was lower in the high-dose group than in the low-dose group (p < 0.05). Further, using a logistic regression model, there were no risk factors associated with the incidence of AF.
The results indicated that telmisartan in low doses was as effective in controlling the blood pressure as in high doses, but high doses of telmisartan had beneficial effects on preventing the recurrence of AF in hypertensive patients.
Correspondence to: Shingo Maeda, MD, 1-26-1 Kyonancho, Musashino-city, Tokyo, 180-8610, Japan.
It is well known that angiotensin-converting enzyme (ACE) inhibitors and angiotensin-II type I receptor blockers (ARBs) are not only effective in treating hypertension but also in reducing the morbidity and mortality in various disease conditions including atrial fibrillation (AF),1 coronary artery disease (CAD),2 and congestive heart failure (CHF).3 The action of high-dose telmisartan was shown to be equivalent to that of highdose ramipril in preventing cardiovascular events in the Ongoing Telmisartan Alone in Combination with Ramipril Global Endpoint Trial (ONTARGET).4 It is not known, however, whether lowdose telmisartan can exert as effective an action as high-dose telminsartan in preventing cardiovascular events. Therefore, we investigated the dosedependent effects of telmisartan on the prevention of AF in patients associated with risk factors.
The patients were eligible for this study if they were older than 30 years old and had essential hypertension with a systolic blood pressure (SBP) of > 140 mmHg and/or diastolic blood pressure (DBP) of > 90 mmHg. Both treated and untreated hypertensive patients were included. Furthermore, each patient had more than one risk factor for cardiovascular disease in addition to hypertension. The risk factors included a past history of AF, CAD with vessel revascularization, CHF, renal disease (RD), stroke, diabetes mellitus (DM) and dyslipidemia (DL). The patients with a past history of AF were defined as patients who had either two or more episodes of symptomatic AF documented by an electrocardiogram (ECG), including 24-hour ambulatory ECG monitoring, in the previous 6 months before the enrollment into this study. Moreover, the patients with a past history of AF took antiarrhythmics or beta-blockers to maintain sinus rhythm for at least 8 weeks, a period considered long enough to ensure a steady state of the drug concentration, before the enrollment into this study. Further, according to the definition of the HRS/EHRA/ECAS, paroxysmal AF (PAF) is defined as recurrent AF (> 2 episodes) that terminates spontaneously within 7 dayse.5 Patients who had suffered from a cardiovascular event or stroke within the previous year were excluded from the study. Patients with CHF with an NYHA grade 3 or higher, or serum creatinine level higher than 3.0 mg/dL were also excluded. The use of other anti-hypertensives, antiarrhythmics, antiplatelet drugs, anti-coagulant drugs, statins and anti-diabetic drugs were allowed, but the doses of those drugs were kept unchanged during the study. RD was defined as an estimated glomerular filtration rate (eGFR) of less than 60mL/min/1.73m2. We calculated the eGFR using a modified Modification of Diet in Renal Disease (MDRD) equation:6 eGFR (mL/min/1.73m2) = 175 × (serum creatinine)-1.154 × (age)-0.203×0.741 (×0.742 if female). DL was defined as a low-density lipoprotein cholesterol (LDL-C) level of ≥ 140 mg/dl, high-density lipoprotein cholesterol (HDL-C) level of < 40 mg/dl or triglyceride level (TG) of ≥ 150 mg/dl. One hundred consecutive hypertensive patients, who met the above criteria, were randomized to take 40mg of telmisartan daily (low-dose group) or 80 mg daily (high-dose group), and were followed at the outpatient clinic for 24 months. The study protocol was approved by the ethic committees at Yokohama Minami Kyosai Hospital. A written informed consent was obtained from all patients before enrollment in the study.
Measured Parameters and Endpoints
The blood pressure (BP) was measured with a mercury sphygmomanometer in the sitting position after 10 minutes of rest in a quiet room, and all caffeine-containing drinks that might influence the BP were withheld for 12 hours before the BP measurement. The SBP and DBP were measured twice by a single investigator, each separated by ≥ 5 minutes. The higher BP value was taken into the database. Phase І and the loss of the V Korotkoff sounds from the brachial artery were used as the systolic and diastolic pressures, respectively, and the heart rate was measured using the ECG. We compared the following parameters between the two groups: clinical characteristics, past medical history, baseline concomitant medications, BP, heart rate, laboratory data, echocardiographic findings and hospital outcomes defined as the incidence of AF, CAD, CHF, RD, strokes, DM, DL or death. All the parameters except for the BP and heart rate were measured at the beginning and during the 24-months of the follow-up study. The BP and ECG were measured each month of the follow-up at the outpatient clinic. To identify the frequency and duration of asymptomatic AF episodes, all patients underwent 24-hour ambulatory ECG monitoring every 4 weeks using a SEER Light Holter recorder (GE Healthcare Inc., Milwaukee). The recording was always started after the drug intake and was performed throughout a full 24-hour period, during which the subjects were allowed to follow their normal daily routine, after they had left the laboratory. The patients were also asked to report any episodes of palpitations, take their pulse and, in the presence of irregular beats, receive an ECG as early as possible. Only AF episodes documented by ECG recordings were considered a new onset or recurrence. Palpitations alone were not taken into consideration since they were the patients’ subjective appraisal. The primary endpoints of the study were defined as the new development and/or recurrence of AF. The outcome of CAD was defined as the need for vessel revascularization for coronary events, and that of CHF as hospitalization due to cardiac decompensation.
Statistical analyses were performed using SPSS version 10.0 software (SPSS Inc., Chicago, Illinois). The potential risk factors were assessed by the association and incidence of AF. Data are expressed as the mean ± SD for continuous variables. The continuous variables of the baseline data were examined by a Student’s t test, and the comparisons between that data obtained before and after the treatment were analyzed by a paired t test. The Fishers exact test was used for categorical variables. The endpoints were analyzed on an intention- to-treat basis. A p value of < 0.05 was considered significant. We used standard methods for the analysis of the case-control data and used logistic regression models to estimate the odds ratio (OR) as a measure of the relative risk. We presented the results from the univariate and multivariate models that were controlled for the incidence of AF, age, sex, history of CHF, taking ACE inhibitors or beta-blockers, left atrial dimension (LAD), left ventricular ejection fraction (LVEF) and BNP (brain natriuretic peptide) level. The event-free curves of AF were illustrated using a Kaplan-Meier analysis. A p value of < 0.05 was considered significant.
Table 1 presents the baseline clinical characteristics of the low-dose (n = 57) and high-dose groups (n = 43). There were no statistical differences between the two groups in terms of the clinical characteristics, past medical history, use of baseline concomitant medications, data of the BP and heart rate, and CHADS2 score. In the low-dose group, 6 patients (11%) had PAF, and 4 (9%) in the high-dose group had PAF at baseline. In the patients with a past history of PAF, there were no differences in the frequency of AF episodes (0.6 ± 0.3 vs. 0.5 ± 0.3 times / month, p = N.S.) between the low-dose and high-dose groups at baseline.
Table 1. Patient Characteristics
| Variable |
Low-dose group (n = 57) |
High-dose group (n = 43) |
p value |
| Clinical characteristics |
|
|
|
| Age (years) |
70 ± 12 |
71± 13 |
N.S. |
| Gender (M/F) |
34 / 23 |
25/18 |
N.S. |
| Body mass index (kg/m 2) |
3.9 ± 5.1 |
25.4 ± 4.2 |
N.S. |
| Medical history variables |
|
|
|
| Paroxymal atrial fibrillation |
6 (11%) |
4 (9%) |
N.S. |
| Atrial fibrillation episodes (per month) |
0.6 ± 0.3 |
0.5 ± 0.3 |
N.S. |
| Chronic atrial fibrillation |
2 (4%) |
2 (5%) |
N.S. |
| Coronary artery disease |
19 (33%) |
15 (35%) |
N.S. |
| single-vessel disease |
5 / 19 (26%) |
5 / 15 (33%) |
N.S. |
| multi-vessels disease |
14 / 19 (74%) |
10 / 15 (67%) |
N.S. |
| Congestive heart failure |
10 (18%) |
3 (7%) |
N.S. |
| Renal dysfunction |
24 (42%) |
22 (51%) |
N.S. |
| Stroke |
5 (9%) |
4 (9%) |
N.S. |
| Diabetes mellitus |
9 (16%) |
10 (23%) |
N.S. |
| Dyslipidemia |
28 (49%) |
26 (60%) |
N.S. |
| Baseline concomitant medication use |
|
|
|
| ACE inhibitors |
4 (7%) |
1(2%) |
N.S. |
| Beta-blockers |
15 (26%) |
13 (30%) |
N.S. |
| Ca-blocker |
30 (53%) |
26 (60%) |
N.S. |
| Diuretics |
12 (21%) |
7 (16%) |
N.S. |
| Anti-arrhythmic drugs |
2 (4%) |
3 (7%) |
N.S. |
| Antiplatelet drugs |
24 (42%) |
20(46%) |
N.S. |
| Anticoagulant drugs |
8 (14%) |
5 (12%) |
N.S. |
| Statins |
22 (38%) |
21 (49%) |
N.S. |
| Diabetic drugs |
7 (12%) |
9 (21%) |
N.S. |
| Presentation variables |
|
|
|
| Systolic blood pressure (mmHg) |
148 ±17 |
153 ±12 |
N.S. |
| Diastolic blood pressure (mmHg) |
82 ± 13 |
80 ± 13 |
N.S. |
| Heart rate (bpm) |
71 ± 13 |
69 ± 9 |
N.S. |
| CHADS2 score |
1.8 ± 1.0 |
2.0 ± 0.8 |
N.S. |
| 0 |
0 (0%) |
0 (0%) |
N.S. |
| 1 |
25 (44%) |
15 (35%) |
N.S. |
| 2 |
20 (35%) |
20 (46%) |
N.S. |
| 3 |
7 (12%) |
6 (14%) |
N.S. |
| 4 |
5 (9%) |
2 (5%) |
N.S. |
Data are presented as the mean ± SD or percent. The body mass index was calculated as the weight in kilograms divided by the square of the height in meters. ACE inhibitors = angiotensin-converting enzyme inhibitors; Ca-blocker = calcium-channel blockers
Blood Pressure and Heart Rate
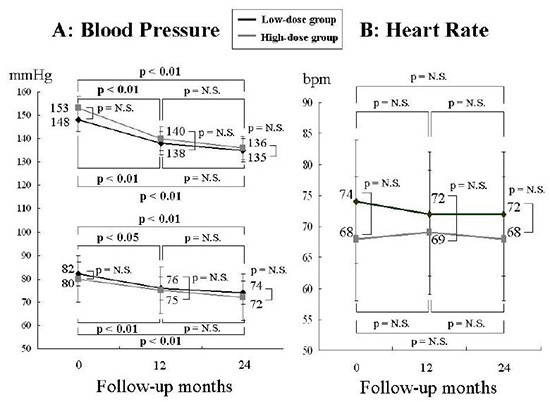
At baseline, 91% of the patients in the low-dose group and 97% in the high-dose group had undergone antihypertensive therapy other than telmisartan before the enrollment in the study. The ratio of those taking other hypertensive drugs did not differ between the two groups Table 1. Figure 1 shows the changes in the BP (A) and heart rate (B) during the study. There was a substantial reduction in the SBP and DBP values 12 months after the treatment in both groups. At the end of the followup, the SBP decreased by 13 mmHg (p < 0.01; versus baseline) in the low-dose group and by 17 mmHg in the high-dose group (p < 0.01; versus baseline). The degree of the SBP decrease did not differ between the two groups. The DBP also decreased by a mean of 8 mmHg in both groups at the end of the 24 months. The heart rate did not change at baseline, or 12 or 24 months after the treatment.
Figure 1. Changes in the blood pressure (Left, A) and heart rate (Right, B) at baseline, during treatment with 40 mg (Low-dose group) and 80 mg (High-dose group) of telmisartan. P = between-group differences; N.S. = not significant; bpm = beats per minute
Changes in the Laboratory Data and Echocardiographic Parameters
Table 2 shows the laboratory data and echocardiographic parameters at baseline and after 24 months of follow-up. There were no differences in any of the laboratory data at baseline or 24 months both in the low-dose and high-dose groups (A). As for the echocardiographic parameters, there was no difference in the LAD or LVEF at baseline in the two groups as well as between the baseline and after 24 months in each group (B).
Table 2. Laboratory Values and Echocardiographic Findings After 24 Months
| Variable |
Low-dose group |
High-dose group |
|
Baseline |
24 months |
p value |
Baseline |
24 months |
p value |
| A: Laboratory values |
|
|
|
|
|
|
| Creatinine (mg/dl) |
0.9 ± 0.3 |
0.9 ± 0.3 |
N.S. |
0.9 ± 0.4 |
0.9 ± 0.3 |
N.S. |
| eGFR(mL/min/1.73sqm) |
60 ± 17 |
63 ± 17 |
N.S. |
61 ± 21 |
65 ± 20 |
N.S. |
| Potassium (mEq/l) |
4.2 ± 0.3 |
4.2 ± 0.4 |
N.S. |
4.1 ± 0.4 |
4.1 ± 0.4 |
N.S. |
| Glucose (mg/dl) |
109 ± 24 |
120 ± 46 |
N.S. |
122 ± 43 |
132 ± 45 |
N.S. |
| HbA1c (%) |
5.8 ± 1.1 |
6.0 ± 1.0 |
N.S. |
5.9 ± 0.9 |
6.0 ± 1.0 |
N.S. |
| T-CHO (mg/dl) |
184 ± 26 |
188 ± 32 |
N.S. |
186 ± 30 |
179 ± 34 |
N.S. |
| LDL-C (mg/dl) |
110 ± 21 |
115 ± 27 |
N.S. |
109 ± 27 |
104 ± 31 |
N.S. |
| HDL-C (mg/dl) |
48 ± 13 |
52 ± 8.9 |
N.S. |
53 ± 15 |
51 ± 14 |
N.S. |
| TG (mg/dl) |
118 ± 57 |
127 ± 61 |
N.S. |
129 ± 68 |
122 ± 46 |
N.S. |
| BNP (μg/ml) |
103 ± 140 |
70 ± 93 |
N.S. |
56 ± 85 |
53 ± 63 |
N.S. |
| B: Echocardiographic findings |
|
|
|
|
|
|
| LAD (mm) |
40± 8 |
40 ± 6 |
N.S. |
40 ± 7 |
42 ± 7 |
N.S. |
| LVEF (%) |
68 ± 10 |
69 ± 9 |
N.S. |
68 ± 11 |
69 ± 8 |
N.S. |
Data are presented as the mean ± SD or percent. eGFR = estimated glomerular filtration rate; HbA1c = hemoglobin A1c; T-CHO = total cholesterol; LDL-C = low-density lipoprotein cholesterol; HDL-C = high-density lipoprotein cholesterol; TG = triglyceride; BNP = brain natriuretic peptide; LAD = left atrial diameter; LVEF = left ventricular ejection fraction
Incidence of Endpoints During the Study
Various cardiovascular events and other outcomes were observed in both groups during the study, however, the number of patients developing such events were less than 7 Table 3,4. There was a tendency toward a lesser incidence of events in the high-dose group than in the low-dose group, but a statistical difference was achieved only for the incidence of AF Table 3. The incidence of AF at 24 months was 0 / 41 patients (0%) in the high-dose group and 5 / 55 patients (9%) in the low-dose group (p < 0.05). Four patients with chronic AF at baseline in the low-dose and highdose groups were excluded from the analysis. Among the 5 patients with AF, 4 had a recurrence and the remaining one had a new onset. The recurrence rates of AF in the patients with a history of paroxysmal AF were lower in the highdose group than in the low-dose group (0 / 4 pts [0%] vs. 4 / 6 pts [67%], p< 0.05). Table 5 shows the clinical characteristics in the patients with a history of paroxysmal AF. In 3 of 4 patients with recurrence of documented AF using the 24-hour ambulatory ECG monitoring in the low-dose group, the AF episode duration tended to be shorter at 24 months (43 ± 42 to 30 ± 34 minute, p = N.S.). In the remaining patient the AF changed to chronic AF during the follow-up period. In addition, one patient had a past history of CHF, however, and other 5 had no new CHF in the follow-up. Moreover, the mean level of the BNP was 44 ± 37 μg/ml Table 5.
Table 3. Incidence of Endpoints During the Study
| Outcome |
Low-dose group(n = 57) |
High-dose group(n = 43) |
p value |
| Atrial Fibrillation |
5/55(9%) |
0/41(0%) |
<0.05 |
| New Atrial Fibrillation |
1/49(2%) |
0/37(0%) |
N.S. |
| Recurrent Atrial Fibrillation |
4/6(67%) |
0/4(0%) |
<0.05 |
A p<0.05 was considered statistically significant
Table 4. Other Outcomes During the Study
| Outcome |
Low-dose group
(n = 57) |
High-dose group(n = 43) |
p value |
| Coronary artery disease |
7(12%) |
2(5%) |
N.S. |
| Congestive heart failure |
4(7%) |
0(0%) |
N.S. |
| Renal dysfunction |
1(2%) |
1(2%) |
N.S. |
| Stroke |
1(2%) |
0(0%) |
N.S. |
| Diabetes mellitus |
1(2%) |
1(2%) |
N.S. |
| Dyslipidemia |
6(11%) |
3(7%) |
N.S. |
| Death |
1(2%) |
0(0%) |
N.S. |
Patients could have multiple events in this category.
There were no differences between the low-dose group and high-dose group in regard to the incidence of other outcomes Table 4. One patient died due to a stroke in the low-dose group, and there was no difference in the number of deaths between the two groups. By using a logistic regression model, there were no risk factors associated with the incidence of AF Figure 2. In the Kaplan-Meier analysis, the patients in the low-dose group had a higher risk for AF than those in the high-dose group (p < 0.05) Figure 3 at 24 months. However, there was no difference in the incidence of events at 12 months.
Figure 2. Logistic regression analysis of the various parameters. The corresponding values of each parameter are presented for atrial fibrillation. CHF = congestive heart failure; ACE = angiotensin-converting enzyme; LAD = left atrial dimension; LVEF = left ventricular ejection fraction; BNP = brain natriuretic peptide
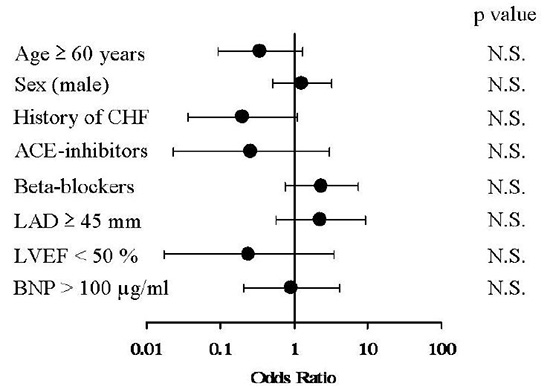
Figure 3. Kaplan-Meier analysis of atrial fibrillation. The patients in the low-dose group had a higher risk for AF than those in the high-dose group at 24 months. However, there was no difference in the incidence of events at 12 months
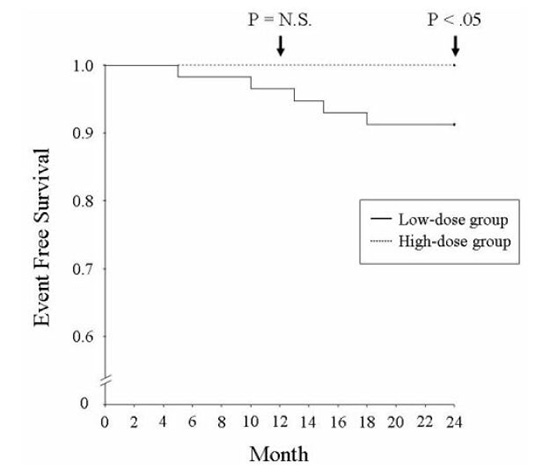
Table 5. Clinical Characteristics in Patients with a History of Paroxysmal Atrial Fibrillation
|
Low-dose group (n=6) |
High-dose group (n=4) |
| Case |
1 |
2 |
3 |
4 |
5 |
6 |
1 |
2 |
3 |
4 |
| Age |
58 |
66 |
78 |
74 |
64 |
72 |
65 |
66 |
71 |
77 |
| Sex |
male |
female |
male |
female |
male |
female |
male |
male |
female |
female |
| Past history of CHF |
no |
no |
no |
yes |
yes |
yes |
no |
no |
no |
no |
| Beta-blocker use |
no |
no |
yes |
yes |
yes |
yes |
no |
no |
no |
yes |
| Anti-arrhythmic use |
yes |
yes |
no |
no |
no |
no |
yes |
yes |
yes |
no |
| BNP (μg/ml) |
20 |
8 |
56 |
90 |
9 |
59 |
8 |
72 |
49 |
32 |
| LAD (mm) |
40 |
32 |
45 |
42 |
35 |
41 |
35 |
44 |
33 |
40 |
| LVEF (%) |
63 |
60 |
72 |
58 |
68 |
81 |
69 |
63 |
73 |
76 |
| Systolic BP mmHg (0M) |
156 |
146 |
140 |
164 |
140 |
174 |
150 |
142 |
150 |
160 |
| Systolic BP mmHg (24M) |
138 |
125 |
135 |
133 |
138 |
130 |
135 |
118 |
138 |
136 |
| Diastolic BP mmHg (0M) |
90 |
76 |
80 |
91 |
65 |
80 |
90 |
80 |
75 |
90 |
| Diastolic BP mmHg (24M) |
70 |
65 |
70 |
76 |
78 |
70 |
75 |
64 |
70 |
80 |
| HR bpm (0M) |
69 |
60 |
70 |
70 |
74 |
60 |
64 |
68 |
61 |
61 |
| HR bpm (24M) |
66 |
61 |
75 |
70 |
78 |
64 |
69 |
72 |
66 |
60 |
| AF recurrence |
yes |
yes |
yes |
yes |
no |
no |
no |
no |
no |
no |
| AF episodes per month (0M) |
0.5 |
0.8 |
1 |
0.5 |
0.25 |
0.33 |
0.2 |
0.8 |
0.4 |
0.4 |
| AF episodes per month (24M) |
0.5 |
0.5 |
1 |
CAF |
0 |
0 |
0 |
0 |
0 |
0 |
| AF duration min (0M) |
18 |
20 |
92 |
25 |
9 |
5 |
16 |
4 |
8 |
21 |
| AF duration min (24M) |
9 |
12 |
70 |
CAF |
0 |
0 |
0 |
0 |
0 |
0 |
CHF = congestive heart failure; BNP = brain natriuretic peptide; LAD = left atrial diameter; LVEF = left ventricular ejection fraction; BP = blood pressure; M = month; HR = heart rate; AF = atrial fibrillation; CAF = chronic AF.
ACE inhibitors and ARBs are known to prevent various cardiovascular events in high risk hypertensive patients.1-3 The Losartan Intervention For Endpoint reduction in hypertension (LIFE) study1 and the Valsartan Antihypertensive Long-term Use Evaluation (VALUE) trial7 demonstrated that ARBs prevented cardiovascular morbidity and death in patients with hypertension more effectively than beta-blockers or Ca channel blockers. Moreover, those studies indicated that the angiotensin II receptor blockers prevent the development of AF in hypertensive patients. Furthermore, a recent report on the ONTARGET study4 indicated that 80 mg of telmisartan daily was equivalent to the ACE inhibitor ramipril, and was effective in preventing relapses of lone AF.8 Further, with a dose of 10 mg daily, not only did it have an antihypertensive action but it also prevented atrial fibrillation. It is not known, however, whether low-dose telmisartan can exert as effective an action as high-dose telminsartan in preventing cardiovascular events. Therefore, we examined the antihypertensive and preventive effects of telmisartan in low and high doses in hypertensive patients with risk factors. It was reported that treatment with 40 and 80 mg of telmisartan achieved a similar degree of a BP reduction with the two different doses.9 Our results confirmed a similar time course and degree of antihypertensive effects on the BP reduction with the 40 and 80 mg doses of telmisartan. Several studies also indicated that dose-dependent actions of telmisartan were observed for other parameters than a BP reduction.10 In our study, different effects of the 40 and 80 mg doses of telmisartan on the cardiovascular complications were noted only for the recurrence rate of AF and not for the other parameters. A beneficial action against AF was observed after 24 months of treatment, while the antihypertensive effects had already been noted after only 12 months of treatment. In the GISSI-AF trail,11 no significant reduction was found in the incidence of recurrent AF among the patients receiving valsartan compared with those receiving a placebo at one year. At least more than one year may be necessary to prevent the development of AF with the effects of the ARBs in this study. Thus, in contrast to the antihypertensive effects, the preventive effects against cardiovascular risk factors seemed to be a time consuming process. While the prevention of AF recurrences was achieved in the high dose group, no other differences in the parameters were apparent between the 80 mg and 40 mg groups. This may partly be related to the study protocol involving a relatively short follow-up period of 24 months. ACE inhibitors and ARBs seem to prevent AF by reversing the changes in the cardiac structure and function. Left ventricular hypertrophy and left atrial enlargement are important factors for cardiac remodeling associated with hypertension and heart failure as well as the development of clinical AF.12 As to the basis of the structural remodeling involving an increased susceptibility to the development and maintenance of AF, atrial fibrosis is an important feature of the substrate, which alters the function of the slow and inhomogeneous conduction. Slow and inhomogeneous conduction is a pre-requisite for the development of reentrant tachyarrhythmias such as AF. A variety of signaling systems seem to be involved in the promotion of atrial fibrosis, and angiotensin II and related mediators are supposed to play a central role in this process.13 Actually, Kumagai et al.14,15 studied the chronic effects of ARBs on the rapid-pacing AF model in dogs. They demonstrated that the AF duration was significantly shortened after 5 weeks of treatment with ARBs as compared to the control with improvement in the conduction but no effects on the refractory period, another determinant of reentry. Improvement in the conduction could be achieved through the prevention of fibrosis leading to the attenuation of the structural remodeling caused by angiotensin II and related mediators. Thus, prevention of AF by ARBs may, at least in part, be explained by the anti-fibrotic effects of the drugs. Moreover, telmisartan is the only ARB, which has a unique property of activating peroxisome proliferators-activated receptor-γ (PPAR-γ) .16,17 An activator of PPAR-γ, pioglitazone, has recently been shown to attenuate both atrial fibrosis and AF promotion in rabbit models with CHF.18 Therefore, telmisartan may have a direct action on the process of atrial reverse-remodeling and, furthermore, the blockade of angiotensin-II may suppress not only AF promotion by preventing structural remodeling, but also AF recurrence, by improving the arrhythmogenic substrate.
Our study had several limitations. First, this study was a single-arm study without any controls, and was not a double-blinded, cross-over trial. The numbers of the study population were rather small and there was a low incidence of serious adverse events. Multicenter studies with large numbers of participants are necessary to confirm the beneficial dose-dependent effects of telmisartan in hypertensive patients. Second, in order to assess the frequency and duration of arrhythmias in either silent or symptomatic AF episodes, we might have to use memory-loop ECG recording instead of 24-hour ambulatory ECG monitoring. Third, the follow-up in this study of a period of 24 months was relatively shorter than that in the other clinical trials, which were usually conducted for at least five years.
The present results indicated that telmisartan in low doses was as effective for controlling the blood pressure as high doses, but high-dose telmisartan had beneficial effects on preventing the recurrence of AF in high-risk hypertensive patients/






