Characterization of Left Atrial Tachyarrhythmias in Patients
Following Atrial Fibrillation Ablation:
Correlation of surface
ECG with Intracardiac Mapping
Sanjay Dixit
Cardiovascular Division, Hospital of The University of Pennsylvania, Philadelphia, PA.
With expected success rates in excess of 80% for achieving long term arrhythmia control, catheter based ablation has become a popular treatment strategy in the management of patients with atrial fibrillation (AF). However, the success of AF ablation has been tempered by the occurrence of post procedure left atrial tachycardias and / or flutters, which can be seen in up to 30% of the patients. These arrhythmias are perpetuated either due to abnormalities of impulse formation (abnormal automaticity / triggered activity), or abnormalities of impulse conduction (micro / macroreentry). Regardless of the underlying
mechanism, these tachycardias manifest distinct “P” or flutter waves on the surface ECG, recognition of which may facilitate their characterization / localization. However, because of the frequent overlap in the morphology of P waves, intracardiac mapping is often the only way to distinguish them apart. This
is accomplished using a combination of activation, entrainment and electroanatomic mapping techniques. Tachycardias resulting from abnormalities of impulse formation and / or microreentry are characteristically focal and usually confined in and around pulmonary vein (PV) segments which have
reconnected (septal aspect of right PVs and anterior aspect of left PVs). In contrast, macroreentrant tachycardias manifest a large circuit dimension involving zone(s) of slow conduction. These are most commonly seen to occur around the mitral valve but can develop in any part of the left atrium where
“gaps” across prior ablation lesion sets create altered conduction. Successful ablation of focal tachycardias is usually accomplished by isolating the reconnected PV segment(s). In case of macroreentrant arrhythmias however, a more extensive ablation approach is typically required in order to achieve
conduction block across isthmus of the circuit. Using these strategies, the majority of left atrial tachycardias occurring post AF ablation can be successfully cured with excellent long term results.
Correspondence to: Dr. Sanjay Dixit, M.D.Assistant Professor of Medicine, 9 Founders Pavilion, Hospital of the University of
Pennsylvania, 3400 Spruce Street Philadelphia, PA 19104.
Catheter based ablation has become a popular
treatment strategy in the management of patients with atrial fibrillation (AF). Although patients undergoing AF ablation can expect success rates in excess of 80%,1-3 the procedure is associated with a small risk of complications, the commonest of which is the development of organized atrial tachyarrhythmias i.e., atrial tachycardias (AT) and / or flutters.4 The latter includes both typical (isthmus dependent) and atypical (usually left atrial) flutter circuits. Common to all of these tachycardias is the presence of well defined, regularly occurring “P” waves which may help with localization as well as provide insights into arrhythmia mechanism(s). Ultimately this information has implications for successfully mapping and ablating the tachycardia. The purpose of this paper is to provide the readers with a concise overview on the various organized atrial tachyarrhythmias seen post AF ablation and discuss their ECG manifestations vis-à-vis information obtained from intracardiac mapping / ablation.
The incidence oforganized atrial tachyarrhythmias in patients undergoing AF ablationhas been reported as ranging from 2% – 30%.5-10 The mechanism(s) underlying development of organized atrial tachyarrhythmias in these patients as reported by various investigators remains inconsistent. One reason for this inconsistency is the use of terms atrial tachycardia (AT) and flutter interchangeably to describe these arrhythmias. By convention, AT implies abnormalities of impulse formation (triggered activity or abnormal automaticity) or a microreentrant circuit which creates the appearance of a focal arrhythmia origin where as flutter implies abnormalities of impulse conduction that results in the formation of a sizableand mappable macroreentrant circuit. The scarred atrium following AF ablation can support any / all of these possible mechanisms. An interesting observation in this context is that centers utilizing wide area circumferential PV ablation without necessarily confirming isolation report a higher prevalence (10- 24%) of macro-reentrant atypical LA flutters.2,5,9 In contrast centers that utilize PV isolation alone have observed a low overall incidence of organized atrial tachycarrhythmias and these have predominantly been focal, originating from in and around the reconnected PV segments.1,7,8,11 In a prospective randomized comparison of segmental PV isolation versus wide area circumferential anatomical PV ablation, Karch et al reported a significantly higher occurrence of organized atrial tacycardias in the latter group (18% versus 2%).5 The likely explanation for this discrepancy is that wide area anatomical ablation results in large scars with “gap” across incomplete lesion sets.
This causes the development of zones of slow conduction that in turn can sustain macroreentrant circuit(s). The usual locations of macroreentrant circuits include, 1) around mitral annulus, 2) around ostia of ipsilateral PVs 3) along the LA roof between the superior veins and, 4) around the fossa ovalis2,12-14 On the other hand focal ATs typically originate from PV ostial segments that have partially recovered conduction to the LA, the most common location being the septal aspect of right sided veins and anterior aspect of left sided veins.7,8 The mechanisms underlying these focal tachycardias include abnormal automaticity, triggered activity and / or microreentry. Typical cavo-tricuspid isthmus dependent right atrial (RA) flutter can also develop in patients post AF ablation, with a reported incidence of 16-23%.7,15 Although this entity is easily recognized, sometimes the flutter wave morphology can be altered due to the presence of ablation related left atrial scarring and thus on the ECG, typical flutter can masquerade as atypical atrial flutter.15
Electrocardiographic Manifestations
The presence of well defined P waves or flutter waves is a characteristic of organized atrial activity and all of these tachyarrhythmias manifest them. The ECG morphology of P waves can facilitate tachycardia localization, not unlike the approach that is frequently used when confronting ventricular tachycardias. However, unlike the latter, characterizing P waves during organized atrial tachyarrhythmias can be challenging for a variety of reasons including, 1) QRST complex overlap, 2) reduced amplitude due to atrial scarring and, 3) similarity in morphology amongst the tachycardias. Despite these limitations, various organized atrial tachyarrhythmias manifest unique features on the surface ECG which can be helpful in distinguishing them apart.
Pulmonary Vein Tachycardias
As discussed above, these tacycardias typically originate from reconnected segment(s) of previously isolated PVs, the typical locations being septal aspect of right sided veins and anterior aspect of left sided veins. In general, because of the posterior location of PVs, these tachycardias manifest positive forces in the precordial leads (V1 – V6). However, P wave morphology in lead V1 can distinguish between right and left PV tachycardias with the former manifesting tall narrow peak with or without a preceding isoelectric segment whereas the latter typically manifests an “M” shaped morphology. Limb leads I and aVL can also be helpful. Typically right PV tachycardias manifest positive forces in lead I and aVL although the latter can sometimes be isoelectric or biphasic. In contrast, for left PV tachycardias, lead I is usually isoelectric or biphasic and lead aVL is
frequently negative (Figure 1). Distinguishing tachycardias originating from ipsilateral PVs (superior versus inferior) is more challenging. In general these tachycardias manifest positive P waves in the inferior leads (II, III, aVF) except when they
originate from the bottom of the inferior veins in
which case these leads may demonstrate either initial small negative forces or predominantly negative complexes (Figure 1,Table 1).16-18
Figure 1.
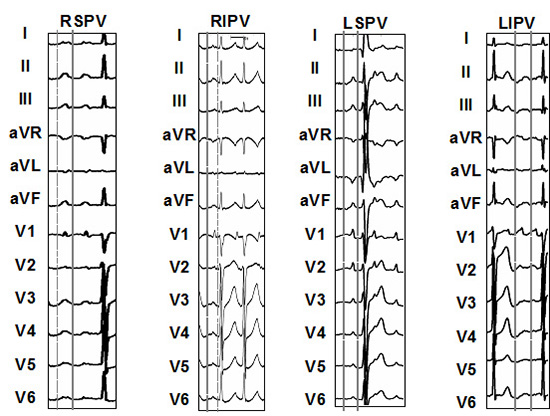
Table 1. Characteristic P wave morphology of organized atrial tachycardias / atypical flutter originating from various locations in the left atrium. RPV = right pulmonary veins, LPV = left pulmonary veins, MA = mitral annulus, CCL = counterclockwise, CL = clockwise
|
RPV |
LPV |
MA
CCL |
MA
CL |
| I |
+ |
+/- |
- |
+ |
| aVL |
+/- |
- |
- |
+ |
| II, III, aVF |
+ |
+ |
+ |
- |
| V1 |
+ |
+
“M“ |
+ |
+ |
| V2-V6 |
+ |
|
+ |
-/+ |
|
|
+ |
|
|
Macroreentrant Flutter Circuits
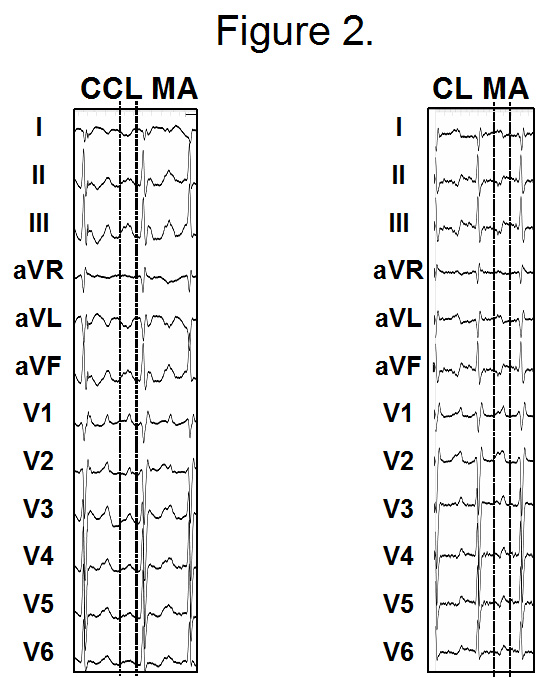
Mitral annular (MA) flutter (counterclockwise-CCL or clockwise-CL) is the most common macroreentrant arrhythmia encountered in patient post AF ablation. CCL MA flutter typically manifests positive forces in the inferior limb leads, completely negative or predominantly negative forces in leads I and aVL and positive flutter wave morphology in the precordial leads (V1 – V6), although lead V2 may manifest a small initial negative component and this is an important characteristic that distinguishes it from left PV tachycardias (Figure 1) and Figure 5A). In contrast, CL MA flutter manifests negative forces in the inferior
leads, positive forces in leads I and aVL and predominantly positive complexes in the precordial leads, although leads V5-6 may manifest initial negative forces (Figure 2).
Figure 2. Shows ECG morphologies of mitral annular (MA) flutter. Counterclockwise (CCL) MA flutter typically manifests positive forces in the inferior limb leads, completely negative or predominantly negative forces in leads I and aVL and positive flutter wave morphology in the precordial leads (V1 – V6), although lead V2 may manifest a small initial negative component. In contrast, clockwise (CL) MA flutter manifests negative forces in the inferior leads, positive forces in leads I and aVL and predominantly positive complexes in the precordial leads,although leads V5-6 may manifest initial negative forces.
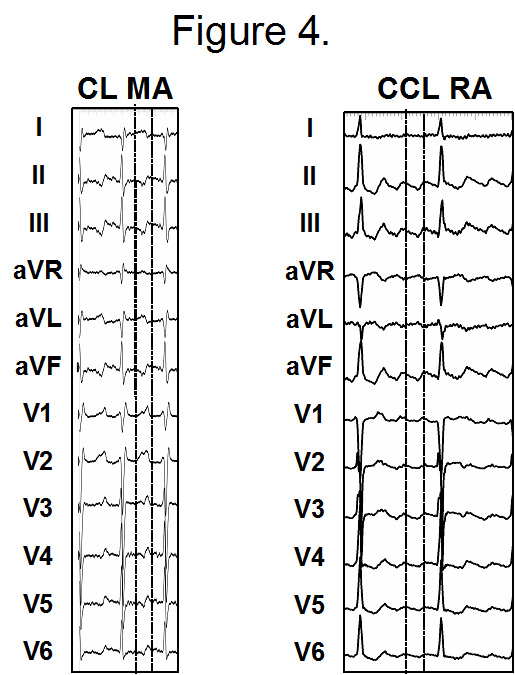
MA and cavotricuspid isthmus dependent RA flutters do share similarities in their ECG manifestations. However, there are some features that can distinguish them apart. So the ECG morphology of CCL MA flutter can be identical to CL RA flutter except lead V1 which is predominantly or completely negative in the latter (Figure 3). Similarly CL MA flutter can mimic CCL RA flutter except lead I which is positive in the former and either biphasic or negative in the latter. Lateral precordial leads (V5-6) can also be helpful in distinguishing between the two – in the latter they manifest predominantly negative forces as compared with CL MA flutter where these leads are predominantly positive (Figure 4).16,18 Other less common circuits that are encountered post AF ablation include reentry around individual or ipsilateral PVs or more complex reentry (figure of “8” or double loop) involving the posterior LA and the roof (between the ly as positive forces in inferior leads, biphasic or negative complexes in leads I / aVL and precordial leads demonstrate some transition. In contrast, for reentry involving the posterior LA, precordial leads manifest positive complexes that lack transition and the limb lead morphology varies based on the proximity of the exit site to the right or left sided veins (see above). Rarely focal tachycardias can originate in the scarred posterior LA, and in that scenario, the ECG morphology follows the same principles outlined above
(Figure 6). In addition to the P wave or flutter wave morphology, some other ECG clues can also be helpful in determining the underlying arrhythmia mechanism. We have previously shown that in patients developing organized atrial tachyarrhythmias post AF ablation, macroreentrant circuits are characterized by the lack of isoelectric intervals between the flutter waves on the 12 lead ECG and faster cycle length (239±7 msec) as compared with focal PV tachycardias which are slower (259±34 msec) and manifest isoelectric segments between the P waves.16 Despite these differences, there remains considerable overlap in the ECG manifestations of these two arrhythmia mechanisms, hence the need for intracardiac mapping.
Figure 3. Shows similarities and differences in the ECG manifestations of counterclockwise (CCL) mitral annular (MA) and clockwise (CL) typical right atrial (RA) flutter. The ECG morphology of CCL MA flutter can be identical to CL RA flutter except lead V1 which is predominantly or completely negative in the latter.
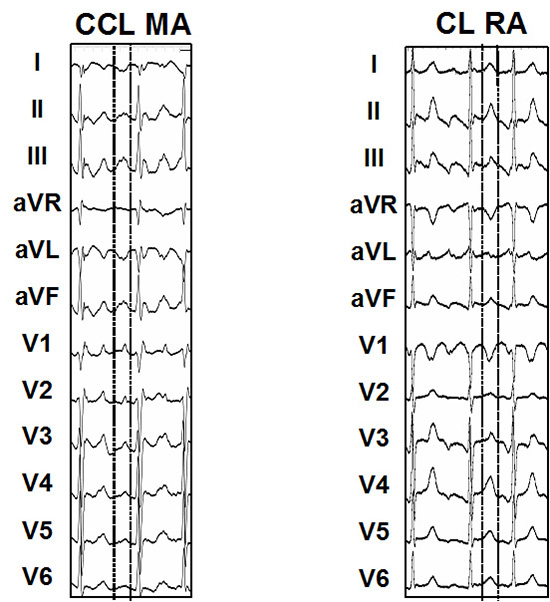
Figure 4. Shows similarities and differences in the ECG manifestations of clockwise (CL) mitral annular (MA) and counterclockwise (CCL) typical right atrial (RA) flutter. The ECG morphology of CCL MA flutter can be identical to CL RA flutter except lead V1 which is predominantly or completely negative in the latter. The ECG morphology of CL MA flutter can be identical to CCL RA flutter except lead I which is positive in the former and either biphasic or negative in the latter. Lateral precordial leads (V5-6) can also be helpful in distinguishing between the two – in the latter they manifest predominantly negative forces as compared with CL MA flutter where these leads are predominantly positive.
Intracardiac Mapping and Ablation
This is typically accomplished by constructing an electroanatomic shell during ongoing arrhythmia in order to characterize the substrate and performing entrainment / resetting maneuvers to determine the underlying mechanism (Figure 5). For macroreentrant rhythms, entrainment mapping is the gold standard to define critical components of the circuit. Upfront, it is important to establish whether the RA participates in the arrhythmia. Thus after deploying multipolar catheters in the RA / coronary sinus (CS) the recommended initial step is to perform entrainment from specific RA locations (cavotricuspid isthmus, lower lateral, mid lateral, posterior wall and high septal sites). Intracardiac fusion with post-pacing intervals (PPI) ≥30 msec of the tachycardia cycle length (CL) at these sites proves lack of RA participation (Figure 5B). Rarely these maneuvers may cause complete RA dissociation during ongoing tachycardia. After excluding RA participation thus, we generally perform entrainment from the proximal and distal poles of the multiploar catheter deployed in the CS (Figure 5C). If the PPI at these 2 locations is ≤20 msec of the tachycardia CL then this suggests strongly that the arrhythmia is likely macroreentrant MA flutter and vice-versa.7 Following this maneuver, the next step is to perform transseptal puncture (preferably twice) in order to access the LA. Some centers deploy two lasso catheters8 and others use a duo-decapolar (Halo) catheter (personal communication). Our practice is to use the Lasso catheter for sampling individual veins. This allows us to establish upfront the extent and distribution of PV reconnections. A separate ablation catheter is utilized to create the detailed LA shell which can depict intracardiac activation pattern and / or the voltage distribution. Points of special interest (areas showing double potentials, sites with PPI ≤20 msec of tachycardia CL with our without concealed entrainment, etc) are tagged and can be displayed on the shell (Figure 6). Using this approach, different tachyarrhythmias (focal versus macroreentrant) manifest unique activation patterns, which can facilitate their recognition.
Figure 5A. Panel A represents the electroanatomic shell of the left atrium in left anterior oblique projection showing the macroreentrant circuit of counterclockwise mitral annular (MA) flutter circuit (arrows). Panel B shows shows the typical ECG morphology of this rhythm. MA flutter typically manifests positive forces in the inferior limb leads, completely negative or predominantly negative forces in leads I and aVL and positive flutter wave morphology in the precordial leads (V1 – V6), although lead V2 may manifest a small initial negative component.
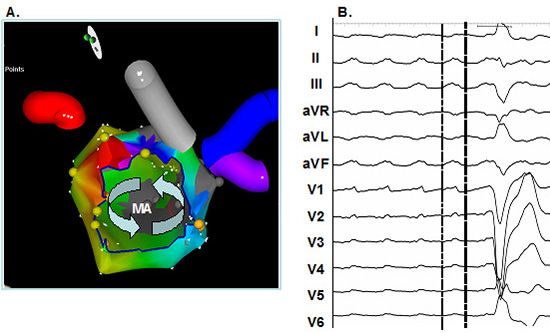
Figure 5B. Represents typical example of response to entrainment from the right atrium during counterclockwise mitral annular (MA) flutter. From top to bottom the recordings are arranged as follows: ECG leads I, aVF and V1, 10 bipoles of circular mapping (Lasso) catheter located in the common ostium of the left sided veins, distal (MAPD) and proximal (MAPP) bipoles of mapping catheter located at lateral MA, 5 biploes of decapolar catheter located in the coronary sinus (cs) and 5 bipoles of decapolar catheter located in the right atrium (RA) along the crista terminalis (CT). Aactivation pattern in the CS is proximal to distal. Following termination of pacing drive from the RA catheter (CT) the postpacing interval is ≥30 milliseconds (ms) longer than the tachycardia cycle length (225ms) which proves that RA is not is not participating in the circuit.
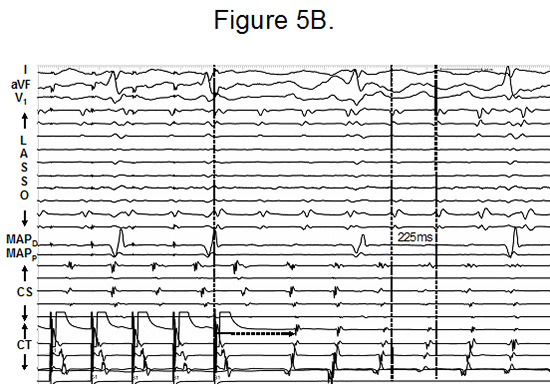
Figure 5C. Represents the same patient as in Figure 5B with identical arrangement of recordings. Following termination of pacing drive from the proximal bipoles (near ostium) of the decapolar catheter located in the CS, the post-pacing interval is identical to tachycardia cycle length (225ms) which proves that proximal CS is in the circuit.
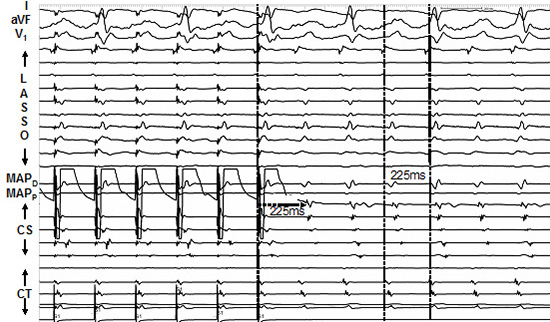
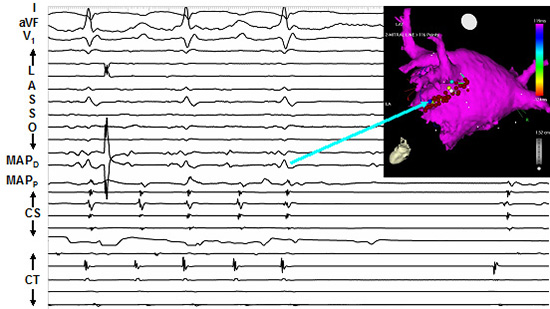
Figure 6.
These are usually localized to the septal aspect of right sided veins or the anterior aspect of the left sided veins where there is segmental PV reconnection. Focal tachycardias display a centrifugal
activation pattern (Figure 6). At these locations it is not uncommon to identify a very early and often fractionated signal which can encompass ~70% of the tachycardia CL.7,18 Care has to be taken to differentiate the true sites of tachycardia origin from areas of markedly delayed conduction around the previously ablated veins that can spuriously appear to be early. Entrainment mapping can be very helpful in making this distinction with the latter locations demonstrating PPI ≥30-40 msec. Once correctly localized, ablation at the appropriate site usually terminates the tachycardia. Even when the tachycardia appears to emanate from within PV, the best strategy is to target the PVLA junction and the recommended end-point is re-isolating (entry / exit block) the culprit vein.16,18
Macroreentrant Flutter Circuits
As discussed above, MA flutter is the most
common type of macroreentrant circuit encountered in patients post AF ablation. Entrainment mapping demonstrating multiple locations around the MA with PPI ≤20 msec is proof of macroreentry and the usual ablation strategy involves delivering lesions across the narrowest part of this circuit, i.e., from the MA to the left inferior PV (Figure 5D and Figure 5E).2,3 Sometimes lesions may need to be delivered within the CS in order to achieve block although this may not always be necessary to terminate the flutter.7,18,19 Lesions extending from septal MA to the right inferior PV may also achieve flutter termination but these are more difficult to deliver both on account of difficulty in catheter deployment in this area and the
relatively longer extent as compared with the isthmus between the MA and LIPV.7,18,19 For macroreentrant circuits involving the roof and / or the posterior wall, lesions connecting the right and left sided PVs are effective and ideally block across these linear lesions should be the end point.2,3,19 In rare instances involving reentry around the veins, following PV isolation additional lesions extending from right PVs to the fossa or left PVs to the appendage and / or the MA may be required to terminate the arrhythmia.7,18 In instances where one or more of the above macroreentrant circuit is suspected but not confirmed (changing tachycardias, disorganization to AF or organization to sinus rhythm during entrainment), a combination of the above lesion sets can be empirically deployed. However, such a strategy results in extensive LA ablation which can potentially be pro-arrhythmic in the long run.
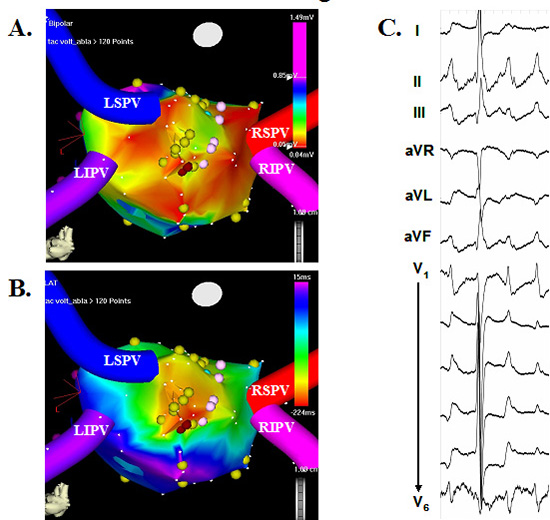
Figure 5D. Represents the same patient as in Figure 5B with identical arrangement of recordings. Following termination of pacing drive from the distal bipoles of the mapping catheter (MAPD) which located at 12 0’clock on the mitral annulus, the post-pacing interval is identical to tachycardia cycle length (225ms) which proves this part of the MA is in the circuit and proves that this is macroreentry.
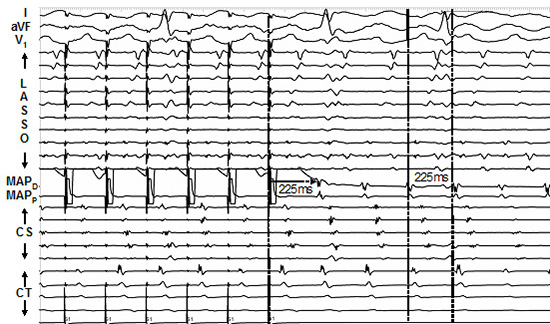
Figure 5E. Represents the same patient as in Figure 5B with identical arrangement of recordings. Lesions were delivered extending from the inferolateral aspect of mitral anulus to the left inferior pulmonary veins (see inset) with additional lesions required within the coronary sinus that resulted in termination of the flutter (see arrow)
Organized atrial tachyarrhythmias are not uncommonly encountered after AF ablation. Depending on the ablation strategy utilized, these can either be focal or macroreentrant. These arrhythmias are associated with well defined P or flutter waves that manifest unique morphologies which can help in
correctly identifying them. This information is very useful in developing a strategy for mapping and successfully ablating them.






