Clinical and Echocardiographic Predictors of Atrial Fibrillation after Coronary Artery Bypass Grafting
Al-Shimaa Mohamed Sabry1, Heba Abd El-Kader Mansour1, Tarek Helmy Abo El-Azm1, Mohamed El Sayed Akef2, Shimaa Ahmed Mostafa1
1Cardiology Department, Faculty of Medicine, Benha University, Egypt.2National Heart Institute, Egypt.
To detect the clinical and echocardiographic parameters that predict AF in coronary artery disease (CAD) patients after coronary artery bypass surgery (CABG).
One hundred CAD patients scheduled for CABG were included. Standard 2D, PW Doppler and 2D speckle tracking echocardiography were performed to assess left atrial (LA) and ventricular (LV) function and their role in predicting post-operative atrial fibrillation (POAF).
Twenty-two percent of patients developed POAF. POAF patients were significantly older (P= 0.001) with increased heart rate (P= 0.001). POAF patients had increased LA diameters and volumes (P < 0.001). Left ventricular ejection fraction (LVEF) was significantly lower in POAF patients (P < 0.004). POAF patients had significantly lower LA and LV global longitudinal strain (LVGLS) (p < 0.001). Clinical predictors of POAF were age and heart rate (P < 0.001). While, echocardiographic measures associated with POAF were LA and LV global longitudinal strain (P <0.001). LA longitudinal strain ≤ 23.1 (85% sensitivity and 66% specificity ) and LVGLS ≤ -14.4 (70% sensitivity and 85% specificity) predicted POAF.
Preoperative LA and LV global longitudinal strain predicts POAF in CABG patients. Echocardiographic deformation measures can enhance clinical profile to identify patients at high risk for POAF.
Key Words : Atrial fibrillation, Coronary artery bypass graft, LA longitudinal strain, LV global longitudinal strain.
Al-Shimaa Mohamed Sabry, Benha University, Faculty of Medicine, Cardiology Department, Benha, Egypt.
After cardiac surgery, postoperative atrial fibrillation (POAF) is the most common type of arrhythmia with an incidence ranging from 33% to 49% 1. Patients with POAF had higher morbidity and mortality post-cardiac surgery 2. Preventive measures may be possible if patients at high risk for POAF were identified early. Preoperative heart rate and rhythm control can be effective in preventing POAF 3. However, the use of prophylactic treatment does not outweigh the risk and thus, medical prophylaxis is not routinely used.
Unfortunately, clinical variables only are not sufficient to identify patients at risk of developing POAF. Therefore, it is still not possible to depend on clinical data only to guide POAF prophylaxis. Impaired left ventricular ejection fraction was associated with POAF 4. However, the role of subclinical LV mechanical dysfunction detected by 2D speckle tracking is less clear. Reduced LV global longitudinal strain, measured by speckle tracking echocardiography (STE), was associated with POAF in patients with aortic stenosis 5 and after mitral valve replacement 6.
Our study aimed at detecting the clinical and echocardiographic measures that can predict POAF in CAD patients undergoing coronary artery bypass graft (CABG).
It is a single center, prospective, observational study that included patients with CAD undergoing CABG at National Heart Institute, Egypt. Exclusion criteria were history of paroxysmal or permanent AF, reduced LV ejection fraction (LVEF < 40%), associated aortic or mitral valve disease requiring aortic or mitral valve replacement, co morbidities precluding cardiac surgery, congenital heart diseases, prior cardiac surgery, and patients refusal. The local ethics committee approved this study, and the patients provided an informed consent.
The primary study endpoint was occurrence of post-operative AF. It was diagnosed by the presence of irregular ventricular rhythm with absence of P wave lasting for at least 30 seconds. Continuous ECG monitoring was performed in the intensive care unit. Daily ECG was performed until discharge from the hospital, and then it was performed on regular weekly visits during the first post-operative 30 days. 12 lead ECG was performed immediately if there was a clinical suspicion of cardiac arrhythmia (palpitation, dyspnea, or chest pain). In patients with new onset post-operative AF, amiodarone was used to regain sinus rhythm. In patients with persistent AF and controlled heart rate, warfarin was started before discharge. Hemodynamically unstable patients or with failure of antiarrhythmic therapy to control heart rate underwent cardioversion.
Echocardiographic examination was performed using Philips iE33 xMatrix – DS Ultrasound Machine with a multi frequency transducer equipped with DTI software and conducted to a single-lead ECG. All measurements were done from the standard views, according to the guidelines of the American Society of Echocardiography and were digitally stored for offline analysis.
LA dimensions were measured during end-ventricular systole. Antero-posterior diameter was measured in the parasternal long-axis view while, longitudinal and transverse diameters were measured in the apical 4-chamber view. Minimal LA volume (Vmin) was measured in end-diastole just before the mitral valve closure. Maximal LA volume (Vmax) was measured in end-systole just before the mitral valve opening. Atrial emptying fraction is the difference between maximum and minimum LA volume divided by the maximum LA volume 7.
LV volumes and ejection fraction were measured from the apical 2- & 4-chamber views, by modified Simpson’s method 8. Color Doppler jet area was used to assess the severity of MR: severe MR (jet area of > 8 cm²), moderate MR (4-8 cm²) and mild MR (< 4 cm²) 9. Tissue Doppler mitral annular velocities "systolic (S), early diastolic (E′), and late diastolic (A′)" were assessed in the apical views (apical four- and two-chamber views) 10.
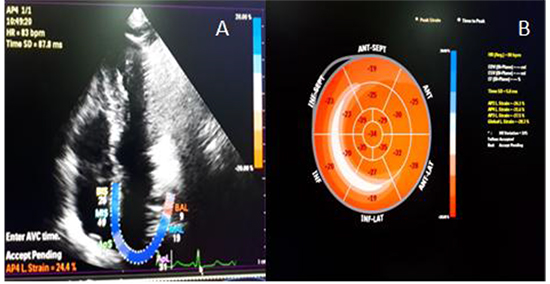
LV global longitudinal strain was measured by 2D speckle tracking echocardiography in the apical 4-, 2-chamber and long axis views with frame rates ranging from 50 to 90 frames/second. The endocardial border was manually traced and the region of interest was adjusted manually to track the entire myocardium. Each left ventricular image was divided into six segments for analysis of segmental strain; global peak systolic longitudinal strain is the average of peak systolic values of the eighteen segments from the three apical views 11. LA strain was also measured by 2D speckle tracking of the apical 4-chamber view. The ECG reference point was set at the onset of the QRS complex, and the region of interest was adjusted to the thickness of the LA wall 12 ([Figure 1] and [Figure 2]).
Figure 1. A 60 years old male developed AF 2 days postoperative. (A) LA strain = 13.7%, (B) LVGLS = -15.8%.
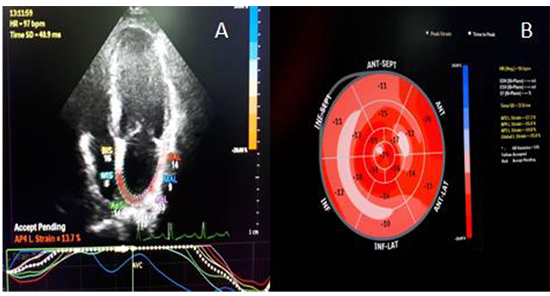
Figure 2. A 46 years old male remained in sinus rhythm. (A) LA strain = 24.4%, (B) LVGLS = -28.3%.
all patients had preoperative coronary angiography. Significant coronary artery stenosis was defined by decreased luminal diameter by by ≥ 50% for left main coronary artery and 70% for the left anterior descending, circumflex, and right coronary arteries. Multivessel coronary artery disease was considered if there is significant stenosis in ≥ 2 vessels 13.
The risk of mortality and morbidity were calculated pre-operatively using STS score for coronary artery bypass graft 14. Parameters for STS score included age, gender, body surface area, DM, HTN, smoking status, chronic lung disease, peripheral vascular disease, cerebrovascular disease, preoperative renal failure, preoperative creatinine level, CHF, prior revascularization procedure, MI timing (hours since MI), preoperative angina, LVEF, left main disease, urgency of operation (status), and preoperative use of an intraaortic balloon pump. The patients were limited to those without previous valve surgery, preoperative endocarditis, or a ventricular assist device.
Statistical analysis was performed using STATA/SE version 11.2 for Windows (STATA corporation, College Station, Texas). Numerical data were summarized in terms of mean± standard deviation (SD). Categorical data were summarized as numbers and percentages. Numerical data were compared using Student t-test (t), or Mann-Whitney test (z). Categorical data were compared using Chi-square test (χ2) and Fisher Exact test (FET) (as appropriate). Receiver operating characteristics (ROC) analysis was used to detect the diagnostic performance of LV and LA global longitudinal strain for POAF. The best cutoff value and its corresponding sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and area under the curve (AUC) were calculated. Stepwise logistic regression analysis was carried out to predict POAF and the results were presented as OR and 95% CI. Comparisons between the models based on the corresponding log likelihood (the smaller the better) and AUC (the greater the better). P-value <0.05 was considered significant, P value <0.001 was considered highly significant while a P value >0.05 was considered non-significant.
One hundred ten CAD patients scheduled for CABG were assessed. Four patients with aortic valve disease requiring aortic valve replacement and six patients with mitral valve disease requiring mitral valve replacement were excluded. Finally, 100 patients were included. Baseline clinical data are summarized in [Table 1].
Table 1. Baseline demographic & clinical data of the studied groups
| Variable |
Overall patients |
POAF (n=22) |
No POAF (n=78) |
P value |
| Age (Mean ± SD) |
56.9 ±7.8 |
65.3 ±5.3 |
54.5 ±6.7 |
<0.001 |
| Gender: |
| Male |
68 (68%) |
16 (72.72%) |
52 (66.66%) |
0.59 |
| Female |
32 (32%) |
6 (27.27%) |
26 (33.33%) |
|
| Cardiac risk factors: |
| Diabetes mellitus |
56 (56%) |
12 (54.54%) |
44 (56.41%) |
0.876 |
| Hypertension |
69 (69%) |
17 (77.27%) |
52 (66.66%) |
0.342 |
| Dyslipidemia |
80 (80%) |
17 (77.27%) |
63 (80.76%) |
0.717 |
| Smoking |
66 (66%) |
11 (50%) |
55 (70.51%) |
0.613 |
| Family history of CAD |
23 (23%) |
6 (27.27%) |
17 (21.79%) |
0.59 |
| Patients' clinical data: |
| Heart rate (bpm) |
81.8 ±11.7 |
90.1 ±7.5 |
79.4 ±11.7 |
<0.001 |
| Systolic blood pressure(mmHg) |
115.4±14.4 |
115.7 ±13.7 |
115.3 ±14.7 |
0.895 |
| Diastolic blood pressure(mmHg) |
70.8 ±9.8 |
72.7 ±9.5 |
70.3 ±9.9 |
0.232 |
| BMI (kg/m2) |
28.8 ±0.93 |
28.8 ±0.83 |
28.8 ±0.97 |
0.92 |
| Patients’ presentation: |
| STEMI |
23 (23%) |
6 (27.27%) |
17 (21.79) |
0.925 |
| NSTEMI |
28 (28%) |
7 (31.81%) |
21 (26.92%) |
0.452 |
| Unstable angina |
27 (27%) |
3 (13.63%) |
24 (30.76%) |
0.11 |
| Stable angina |
22 (22%) |
6 (27.27%) |
16 (20.51%) |
0.499 |
| Medications: |
| Beta-blockers |
53 (53%) |
9 (40.90%) |
44 (56.41%) |
0.198 |
| ACE inhibitors |
66 (66%) |
14 (63.63%) |
52 (66.66%) |
0.791 |
| Angiotensin receptor blockers |
10 (10%) |
4 (18.18%) |
6 (7.69%) |
0.148 |
| Statins |
100 (100%) |
22 (100%) |
78 (100%) |
NA |
| Aspirin |
100 (100%) |
22 (100%) |
78 (100%) |
NA |
| Clopidogrel |
100 (100%) |
22 (100%) |
78 (100%) |
NA |
CAD: coronary artery disease; BMI: body mass index; STEMI: ST elevation myocardial infarction; NSTEMI: non ST elevation myocardial infarction; ACE: angiotensin converting enzyme.
During the follow up period (1 month after surgery), 22 patients (22%) had new onset AF (group I) who were compared with the remaining 78 patients (78%) with sinus rhythm (group II). Group I had 8 patients (36.36%) with paroxysmal AF, 6 patients (27.27%) with persistent AF who regained sinus rhythm on pharmacological cardioversion (amiodaron infusion) and 8 patients (36.36%) required DC shock to regain sinus rhythm.
Patients of group I were significantly older (65.3 ± 5.3 vs. 54.5 ± 6.7, p =0.001) with significantly greater heart rate (90.1±7.5 vs. 79.4±11.7, P <0.001).
Conventional Echocardiographic parameters
Group I had significantly increased LA diameters (antero-posterior, transverse and longitudinal) (4.9±0.3 vs. 4.43±0.2 cm, 4.6±0.2 vs. 4.4±0.2 cm and 6.3±0.4 vs. 5.6±0.4 cm, respectively; p <0.001) and LA volumes (maximal and minimal) (102±5 vs. 96±7 ml and 63 ±7 vs. 58±9 ml, respectively; p <0.001).
LVEF was significantly lower in group I (56±7 vs. 60±6%; p = 0.004). Data were comparable as regard LV end-systolic volume (38.57±14.11 vs. 28.4±1.12 ml; p =0.063), LV end diastolic volume (75±20 vs. 72±13ml; p =0.563) and the severity of mitral regurgitation [Table 2]. E /E` ratio was significantly higher in group I (9.84 ± 2.15 vs. 7.4±2.3; p <0.001). Data were comparable as regard S, E`, and A`.
Table 2. Echocardiographic and angiographic parameters of the studied groups
| Variable |
Group I (n=22) |
Group II (n=78) |
P value |
| Echocardiography: |
| LA antero-posterior diameter |
4.9±0.3cm |
4.43±0.2cm |
< 0.001 |
| LA longitudinal diameter |
6.3±0.4cm |
5.6±0.4cm |
< 0.001 |
| LA transverse diameter |
4.6±0.2cm |
4.4±0.2cm |
< 0.001 |
| LA maximal volume |
102±5ml |
96±7ml |
< 0.001 |
| LA minimal volume |
63±7ml |
58±9ml |
< 0.001 |
| LA emptying fraction |
40±10% |
43±11% |
0.143 |
| LVESV |
38.57±14.11ml |
28.4±1.12ml |
0.063 |
| LVEDV |
75±20ml |
72±13ml |
0.563 |
| LV EF |
56±7% |
60±6% |
0.004 |
| MR severity: |
| No |
10 (45.45%) |
42 (53.84) |
0.437 |
| Mild |
6 (27.27%) |
33 (42.3%) |
|
| Moderate |
2 (9.09%) |
6 (8.97%) |
|
| TDI: |
| S |
0.07±0.08 m/s |
0.08±0.02 m/s |
0.609 |
| E' |
0.12±0.05m/s |
0.12±0.03m/s |
0.22 |
| A' |
0.7±0.2m/s |
0.8±0.2 |
0.274 |
| E/E' ratio |
9.84±2.15 |
7.4±2.3 |
<0.001 |
| LA strain |
20.4±1.7% |
22.1±1.9% |
<0.001 |
| LV GLS |
-14±2.2 % |
-18±3.2% |
<0.001 |
| Number of diseased vessels: |
| Single |
1 (4.54%) |
12 (15.38%) |
0.072 |
| 2 vessel |
12 (54.54%) |
40 (51.28%) |
0.071 |
| Multi-vessel |
9 (40.9%) |
26 (33.33%) |
0.09 |
| Affected vessel: |
| Left main |
11 (50%) |
18 (23.07%) |
0.014 |
| LAD |
22 (100%) |
78 (100%) |
NA |
| LCX |
15 (68.18%) |
53 (67.94%) |
0.983 |
| RCA |
15 (68.18%) |
39 (50%) |
0.131 |
LVESV: left ventricular end systolic volume; LVEDV: left ventricular end diastolic volume; LV GLS: left ventricular global longitudinal strain; LAD: left anterior descending; LCX: left circumflex; RCA: right coronary artery.
Speckle tracking echocardiography
LA and LV global longitudinal strain (LVGLS %) were lower in group I (20.4 ± 1.7 vs. 22.1 ± 1.9 % and -14± 2.2 vs. -18 ± 3.2 %; p < 0.001).
Left main coronary artery involvement was more prevalent in patients of group I (11 patients “50%” vs.18 patients “23.07%”, p =0.014). The data regarding the number of diseased vessels did not differ [Table 2]. The risk of mortality and morbidity, cardio-pulmonary bypass time, cross clamping time, ventilator time, ICU time, inotropic support (dopamine and adrenaline), type of cardioplegia (cold or warm), and post-operative complications were similar in both groups [Table 3].
Table 3. Operative data and postoperative complications of the studied groups
| Variable |
Group I (n=22) |
Group II (n=78) |
P value |
| STS score: |
| Risk of mortality |
1.1±0.5% |
1.5±0.14% |
0.82 |
| Risk of morbidity |
13.8±6.36 |
17.1±6.8% |
0.14 |
| Cardio-pulmonary bypass time |
127±14 min |
130±9 min |
0.054 |
| Cross-clamping time |
78±8 min |
78±5 min |
0.287 |
| Ventilator time |
8.3±2.1 hr |
10.6±5.9 hr |
0.079 |
| ICU duration |
36.95±15.07 hr |
28.1±1.9 hr |
0.518 |
| Dopamine use |
12 (54.54%) |
49 (62.82%) |
0.482 |
| Adrenaline use |
6 (27.27%) |
38 (48.71%) |
0.074 |
| Cold cardioplegia |
22 (100%) |
71 (91.02%) |
0.145 |
| Warm cardioplegia |
0 (0%) |
7 (8.97%) |
0.766 |
| Postoperative complications: |
| Graft failure |
0 (0%) |
2 (2.6%) |
NA |
| Pericardial effusion |
0 (0%) |
2 (2.6%) |
NA |
| Post-operative VT |
0 (0%) |
3 (3.84%) |
NA |
| Post-operative MI |
0 (0%) |
6 (7.69%) |
0.334 |
| Number of diseased vessels: |
| Single |
1 (4.54%) |
12 (15.38%) |
0.072 |
| 2 vessel |
12 (54.54%) |
40 (51.28%) |
0.071 |
| Multi-vessel |
9 (40.9%) |
26 (33.33%) |
0.09 |
| Affected vessel: |
| Left main |
11 (50%) |
18 (23.07%) |
0.014 |
| LAD |
22 (100%) |
78 (100%) |
NA |
| LCX |
15 (68.18%) |
53 (67.94%) |
0.983 |
| RCA |
15 (68.18%) |
39 (50%) |
0.131 |
VT: ventricular tachycardia; MI: myocardial infarction.
Multivariate logistic regression analysis revealed that age (OR 0.005, 95% CI 0- 0.22, p =0.001), heart rate (OR 1.43, 95% CI 1.09- 1.89, p =0.009), LA strain (OR 1.111, 95% CI 1.003- 1.23, p <0.001), and LVGLS (OR 0.643, 95% CI 0.488- 0.846, p <0.001) were significant predictors of POAF.
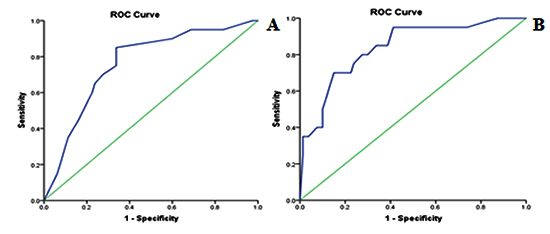
ROC analysis showed that LA strain cut-off value ≤ 23.1 predicted AF post CABG with a sensitivity of 85% and specificity of 66% (AUC 0.761; 95% CI 0.648 - 0.873; p < 0.001). LVGLS cut-off value ≤ -14.4 can predict AF post CABG with a sensitivity of 70% and specificity of 85% (AUC 0.84; 95% CI 0.742 - 0.935; p < 0.001) [Figure 3].
Figure 3. Roc curve of LA systolic strain (A) and LV global longitudinal strain (B)
Our study aimed at determining the clinical and echocardiographic predictors of POAF in patients with CAD and scheduled for CABG as early detection and management of this group of patients may improve their outcome.
We found that 22% of patients developed AF. Folla et al., 15 also, reported a 19% prevalence of AF post CABG. POAF patients were older in age, which is consistent with Perrier et al., 16. We did not find any significant statistical difference between the 2 groups regarding coronary risk factors and preoperative medications, a finding consistent with Parsaee et al., 17.
Left atrial size is a parameter that reflects structural changes in LA. However, LAVI is more accurate for assessment of LA size. LAVI is a predictor of AF in the general population and post cardiac surgery 18.
Table 4. Logistic regression analysis including pre-operative clinical and echocardiographic data
| Variable |
OR |
95% CI |
P |
| Age |
0.005 |
0.00 - 0.22 |
0.001 |
| Heart rate |
1.43 |
1.09 - 1.89 |
0.009 |
| LVGLS |
0.643 |
0.488 - 0.846 |
<0.001 |
| LA strain |
1.111 |
1.003 - 1.23 |
<0.001 |
LVGLS: left ventricular global longitudinal strain; LA: left atrial; CI: confidence interval; OR: odds ratio.
In the present study, POAF patients had increased LA diameters and volumes. Ozben et al., 19 reported that LAVI was an independent predictor of POAF and LAVI >36 ml/m² had 84.6% sensitivity and 68.6% specificity in predicting POAF.
In the current study, POAF patients had reduced left ventricular ejection fraction (LVEF %). However, the data were comparable regarding both left ventricular end diastolic and end-systolic volumes. This was similar to Ismail et al., 20 who reported lower left ventricular ejection fraction in patients with POAF.
Impaired atrial systolic dysfunction is usually associated with increased atrial pressure. This may induce electrical remodeling with increased tendency of developing POAF. E/e′ is associated with LV filling pressures and increased E/e′ ratio is associated with new onset AF 21. In our study, POAF patients had significantly higher E/e′, a finding consistent with Ozben et al., 19.
In the present study, LA global longitudinal strain assessed by 2D STE was significantly reduced in patients with POAF. Similarly, a systematic review of 6 papers by Bigdelu et al., 22 considered strain and strain rate as an independent predictors of POAF after CABG. Global peak atrial longitudinal strain reflects passive stretching of LA during LV systole and is an accurate measurement of LA reservoir function 23.
In the present study, LV global longitudinal strain was significantly decreased in POAF patients (p <0.001). This was similar to Mansour et al., 6 who found that LV global longitudinal strain was significantly reduced in POAF patients after mitral valve replacement. While, This is in contrast to Başaran et al., 24 who reported that the left ventricular global longitudinal strain value was not different between the 2 groups (p >0.005). This could be related to the different group of patients they evaluated who had preserved LV function (the mean LVEF= 62.5%) with spared subenocardial fiber function.
In the present study, left main coronary artery involvement was higher in patients with POAF, but there was no statistical difference regarding the number of diseased vessels. Ismail et al., 20 found no statistical difference between both groups regarding neither diseased vessels nor the number of grafts performed.
There was no significant statistical difference between the 2 groups regarding the risk of mortality and morbidity, cardio-pulmonary bypass time, cross clamping time, ventilator time, ICU time, inotropic support (dopamine and adrenaline), type of cardioplegia (cold or warm) or the post-operative complications. This was similar to Perrier et al., 16 who found no difference between both groups regarding the EuroSCORE. While, Parsaee et al., 17 reported longer cardio-pulmonary bypass time, hospital and ICU stays in patients with POAF as they evaluated patients with impaired preoperative LV systolic function (the mean LVEF = 42.63 ± 9.7%), while in our study, patients had better LV systolic function (the mean LVEF = 52 ± 9%).
In the present study, multivariate logistic regression of the preoperative clinical and echocardiographic data revealed that age and heart rate significantly predicted POAF (P =0.001). While, the echocardiographic parameters were LA longitudinal strain (P <0.001) and LVGLS% (P =0.001). The area under the curve (AUC) was 0.761 and 0.84, respectively.
These results were consistent with Verdejo et al., 11 who reported that age (OR 1.09, 95% CI, 1.01–1.16) and LASs (OR1.63, 95% CI, 1.19–2.22) were both independent predictors of POAF, suggesting that atrial function assessed by echocardiographic deformation may enhance the clinical profile for identifying patients at high risk for developing POAF.
ROC curve identified that LA strain ≤ 23.1 has diagnostic accuracy of 76% in detection of AF post CABG (sensitivity = 85% and specificity = 66%) with an AUC of 0.761 (95%CI ''0.648 - 0.873 ''). LVGLS ≤ -14.4 has an accuracy of 84% in detection of AF post CABG (sensitivity = 70% and specificity =85%) with an AUC of 0.84 (95%CI ''0.742 - 0.935''). This is in agreement with Sabry et al., 6 who reported that LVGLS < -14.9 (sensitivity = 63.6%; specificity = 100.0%) and Tissue Doppler LA systolic strain < 23 (sensitivity = 90.91%; specificity = 93.33%) are the best cutoff for the prediction of POAF after mitral valve replacement.
Firstly, the relatively small size of the patient population and it was a single center study. Secondly, AF was considered only when objectively documented but could be transient, and all episodes may not be detected. Additionally, our observations are limited to the first month after CABG; we could not draw conclusions regarding long-term outcomes. In addition, we included only patients with LVEF > 40%.
POAF patients were older with greater heart rate. Multivariate regression analysis identified age, heart rate, lower LA, and LV global longitudinal strain as significant predictors of POAF. LA strain cut-off value of ≤ 23.1% and LVGLS ≤ -14.4 can predict new onset AF after CABG.






