High Brain Natriuretic Peptide Level Predicts The Prevalence Of Low-Voltage Areas And Poor Rhythm Outcome In Patients Undergoing Atrial Fibrillation Ablation
Yasuhiro Matsuda1, Masaharu Masuda*, Mitsutoshi Asai, Osamu Iida, Shin Okamoto, Takayuki Ishihara, Kiyonori Nanto, Takashi Kanda, Takuya Tsujimura, Shota Okuno, Yosuke Hata, Hiroyuki Uematsu, Toshiaki Mano
Kansai Rosai Hospital Cardiovascular Center, 3-1-69 Inabaso, Amagasaki, Hyogo 660-8511, Japan.
The prevalence of residual left atrial low-voltage areas (LVAs) is associated with atrial fibrillation (AF) recurrence after pulmonary vein isolation. Brain natriuretic peptide (BNP) may be increased in AF patients and may raise AF recurrence risk after catheter ablation. We investigated the association between BNP and the prevalence of LVAs.
One hundred and eighty three consecutive AF cases were retrospectively enrolled that underwent initial ablation for AF (persistent AF, 82 [45%] patients). Serum BNP was measured before ablation and the natural logarithm of BNP (log-BNP) was calculated. Low-voltage points were defined as sites with left atrial electrogram amplitude <0.5 mV. LVAs were defined as regions with ≥5% low-voltage points across the total surface area of the left atrium.
Of the 183 patients, 38 (21%) had LVAs. Patients with LVAs demonstrated higher log-BNP (4.8±0.9 vs. 3.9±1.2, P<0.001). The optimal cut-off value of log-BNP was 4.4, which was equivalent to 81 pg/mL of BNP. LVAs were more frequent in patients with higher log-BNP. In multivariate analysis, log-BNP >4.4 was an independent predictor of LVAs (odds ratio 2.7 [95% confidence interval 1.01–7.1], P=0.048). Freedom from AF recurrence was significantly lower in patients with than without high log-BNP (P=0.007).
BNP correlated with the prevalence of left atrial LVAs and AF recurrence in patients with AF undergoing catheter ablation.
Key Words : Atrial fibrillation, Catheter ablation, Brain natriuretic peptide, Substrate, Low-voltage areas.
Masaharu Masuda, Kansai Rosai Hospital Cardiovascular Center, 3-1-69 Inabaso, Amagasaki-shi, Hyogo, 660-8511, Japan
Catheter ablation is an established effective therapy for atrial fibrillation (AF). However, a number of patients require repeat ablation procedures due to recurrence of atrial tachyarrhythmias. Reduced amplitude on atrial endocardial electrograms correlates with atrial scarring as detected by delayed-enhancement magnetic resonance imaging.1 The prevalence of left atrial low-voltage areas (LVAs) is strongly associated with the recurrence of atrial tachyarrhythmias, and adding guided ablation of LVAs improves procedural outcomes compared to pulmonary vein isolation (PVI) alone.2-5
Brain natriuretic peptide (BNP) is released by the heart in response to myocardial tension and increased intravascular volume, and is a reported biochemical marker of high left ventricular end-diastolic pressure,6 reflective of left atrial pressure. Elevated left atrial pressure is associated with LVA prevalence.7-8 A preliminary study showed that BNP levels were increased in AF patients and was associated with greater risk of AF recurrence after catheter ablation.9 To our knowledge, however, the association between BNP and LVA prevalence has not been fully clarified.
The objective of this study was to investigate the association between BNP levels and the prevalence of LVAs.
From December 2014 to January 2016, we retrospectively enrolled 183 consecutive AF cases of initial ablation at our hospital. Serum BNP levels were measured one day before and 6 months after ablation. Patients who could not maintain sinus rhythm after electrical cardioversion followed by PVI were excluded. Other exclusion criteria were age <20 years, severe coronary artery disease requiring revascularization, left atrial thrombus, and prior catheter ablation of AF. Patients with decompensated heart failure, such as pulmonary edema, were also excluded. This study complied with the Declaration of Helsinki. Written informed consent for the ablation and use of data in this study was obtained from all patients, and the protocol was approved by our Institutional Review Board.
Radiofrequency catheter ablation procedure
Electrophysiological studies and catheter ablation were performed under local anesthesia and intravenous sedation with dexmedetomidine and thiamylal sodium, with the latter performed by two experienced operators. A 6-Fr decapolar electrode was inserted into the coronary sinus, while another 6-Fr decapolar electrode was placed in the right atrium. Following a transseptal puncture at the fossa ovalis, we introduced two or three long sheaths into the left atrium using a single transseptal puncture technique under intracardiac echocardiographic guidance. A 20-pole circular catheter was placed at the pulmonary veins via long sheaths. Electrical cardioversion was performed in cases with persistent AF. Ablation and mapping were then performed under guidance from an electroanatomical mapping system (Carto3; Biosense Webster, Diamond Bar, CA, USA). Circumferential ablation around both ipsilateral pulmonary veins was performed using a dragging technique.
An open-irrigated ablation catheter with a 3.5-mm tip (Thermocool SmartTouch™ catheter; Biosense Webster) was used via an Agilis™ or Swartz™ Braided SL0™ Transseptal Guiding Introducer Sheath (St. Jude Medical, Minnetonka, MN, USA). Radiofrequency energy was applied for 30 s at each site using a maximum temperature of 42°C, maximum power of 35 W, and flow rate of 17 mL/min. At the posterior wall near the esophagus, the duration of the radiofrequency energy delivery was limited to 15 s. Operators attempted to maintain contact force values between 10 and 30 g to ensure an appropriate degree of contact between the catheter and myocardium. PVI was considered complete when the 20-pole circular catheter ceased recording pulmonary vein potentials. If atrial flutter was induced by atrial burst stimuli or occurred spontaneously, additional ablation was performed. AF triggers originating from non-pulmonary-vein foci induced by isoproterenol infusion were also ablated.
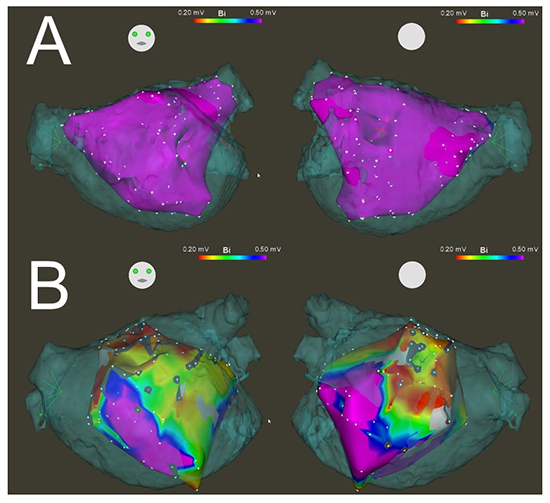
Following PVI, detailed voltage mapping using a bipolar 3.5-mm tip catheter was performed during sinus rhythm using methods we described previously.3 Mapping points were acquired to fill all color gaps on the voltage map using the electroanatomical mapping system with an interpolation threshold of 15 mm for the fill threshold and 23 mm for the color threshold. High-density mapping was additionally added at sites of recorded LVAs to exactly delineate their extent. Adequate endocardial contact was confirmed by increased contact force values of ≥5 g, the distance to the geometry surface, and stable electrograms. The band pass filter was set at 30–500 Hz and each acquired point was classified according to the peak-to-peak electrogram as follows: >0.5 mV, healthy; 0.2–0.5 mV, diseased; and <0.2 mV, scarred. Low-voltage points were defined as sites with ≥3 adjacent points of <0.5 mV as per our previous study.3 LVAs were defined as regions with ≥5% low-voltage points across the total surface area of the left atrium. The target number of mapping points was >100 points throughout the left atrium. Similar to our previous study, the left atrium was divided into six segments: antero-septal, posterior, roof, inferior, and posterolateral.3 Representative cases are shown in [Figure 1].
Figure 1. Representative electroanatomical maps from patients with or without LVAs. (A) A patient without LVAs with low log-BNP (1.4, equivalent to 4 pg/mL of BNP). (B) A patient with LVAs in the antero-septal, posterior, roof, inferior, and posterolateral regions of the left atrium with high log-BNP (5.2, equivalent to 186 pg/mL of BNP). Anterior-posterior view (left), posterior-anterior view (right). LVAs: low-voltage areas, log-BNP: natural logarithm of brain natriuretic peptide, BNP: brain natriuretic peptide.
Long-term rhythm outcomes were followed for 24 months in 181 patients. Two patients were lost to followup. Followup of the patients was performed as routine visits, usually every 3 months in the first year and every 6 months thereafter. Patients who could not visit our hospital were contacted by a physician and asked about their symptoms. A twelve-lead electrocardiogram was performed at each routine consultation and Holter electrocardiography was performed 6 months after the procedure. AF recurrence was defined as atrial tachyarrhythmias lasting >30 s ≥90 d after the procedure.
Continuous data are expressed as the mean ± standard deviation. Categorical data are presented as absolute values and percentages. Tests for significance were conducted using the unpaired t-test, paired t-test or Mann-Whitney test for continuous variables and the chi-squared test for categorical variables. The natural logarithm of BNP (log-BNP) was calculated to follow a normal distribution. Pearson's correlation analysis was performed to analyze the correlation between area on the left atrial surface and BNP or total area with low-voltage. We also performed receiver operating characteristic curve (ROC) analysis between log-BNP and the prevalence of LVAs. Kaplan-Meier analysis and the log-rank test were performed to investigate the association between recurrence of atrial tachyarrhythmia and the prevalence of LVAs. Univariate and multivariate logistic regression analyses were used to determine the clinical factors associated with the prevalence of LVAs. Variables with a P value ≤ 0.05 in the univariate models were included in the multivariate analysis. All analyses were performed using commercial software (SPSS, SPSS, Inc., Chicago IL, USA).
Patient characteristics are shown in [Table 1]. Of the 183 patients in this study, 23 (13%) had a past history of heart failure: 19 (10%) patients had heart failure with a preserved ejection fraction (left ventricular ejection fraction ≥50%) and 4 (2%) had heart failure with a reduced ejection fraction (left ventricular ejection fraction <50%). The presumed causes of heart failure were tachycardia-induced cardiomyopathy (11 patients), ischemic cardiomyopathy (3 patients), dilated cardiomyopathy (2 patients), hypertrophic cardiomyopathy (2 patients), valvular heart disease (2 patients), and other (3 patients).
Table 1. Characteristics of patients with and without high BNPa
| Variable |
All (n = 183) |
Log-BNP |
P value |
|
|
> 4.4b(n = 84) |
≤ 4.4b (n = 99) |
|
| Age, years |
67±9 |
69±8 |
65±10 |
< 0.001 |
| Female, n (%) |
49 (27) |
24 (29) |
25 (25) |
0.61 |
| Body mass index, kg/m2 |
24±3.8 |
23±3.6 |
24±3.9 |
0.10 |
| CHA2DS2-VASc score |
2.3±1.4 |
2.6±1.4 |
2.1±1.5 |
0.02 |
| Persistent AFc, n (%) |
82 (45) |
56 (67) |
26 (26) |
< 0.001 |
| Congestive heart failure, n (%) |
23 (13) |
15 (18) |
8 (8) |
0.047 |
| Hypertension, n (%) |
110 (61) |
49 (58) |
61 (62) |
0.65 |
| Diabetes mellitus, n (%) |
27 (15) |
15 (18) |
12 (12) |
0.28 |
| Brain natriuretic peptide, pg/mL |
73 (27-152) |
159 (109-227) |
30 (17-51) |
< 0.001 |
| Log-brain natriuretic peptide |
4.1±1.2 |
5.1±0.5 |
3.2±0.8 |
< 0.001 |
| eGFRd, mL/min/1.73m2 |
81±24 |
68±15 |
58±14 |
< 0.001 |
| Left ventricular diastolic diameter, mm |
47±5 |
47±6 |
47±5 |
0.50 |
| Left ventricular ejection fraction, % |
64±9 |
63±10 |
65±7 |
0.07 |
| Left ventricular mass index, g/m2 |
97±88 |
92±25 |
101±117 |
0.54 |
| Left atrial diameter, mm |
39±7 |
41±7 |
37±7 |
< 0.001 |
| Mitral regurgitation ≥ mild, n (%) |
52 (28) |
34 (41) |
18 (18) |
0.001 |
a BNP = brain natriuretic peptide. b This log-BNP level is equivalent to 81 pg/mL of BNP. cAF = atrial fibrillation. d eGFR = estimated glomerular filtration rate. Values indicate mean ± standard deviation or median (1st quartile-3rd quartile).
PVI was successfully completed in all cases. We performed the following additional ablations: cavo-tricuspid isthmus linear ablation in 24 patients, left atrial linear ablation in 7 patients, superior vena cava isolation in 5 patients, premature atrial contraction or focal atrial tachycardia ablation originating from lesions other than the pulmonary vein or superior vena cava in 4 patients, and ablation of other lesions in 6 patients. Complications such as cardiac tamponade, stroke, bradycardia requiring permanent pacemaker implantation, and atrio-esophageal fistula were not observed.
Left atrial voltage mapping was completed in all cases, with a mean number of acquired mapping points of 104 ± 23 per case. LVAs were identified in 38 (21%) cases. Of these, the total area with low-voltage was 11.5 (8.5–20.3) cm2, the total area on the left atrial surface was 91.3 (78.0–107.0) cm2, and the proportion of areas with low-voltage on the left atrial surface was 11.6% (8.3–18.9%). There was significant correlation between the area on the left atrial surface and total area with low-voltage (r = 0.25, p < 0.001). LVAs were present in the antero-septum, posterior, roof, inferior, and posterolateral segments in 57 (31%), 16 (15%), 19 (16%), 8 (6%), and 7 (4%) patients, respectively.
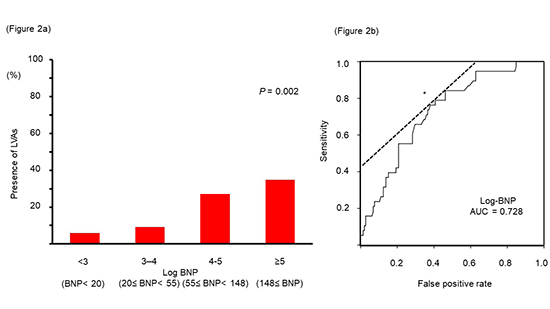
Patients with LVAs demonstrated higher BNP levels (138 (82-213) vs. 55 (23-119) pg/mL, P < 0.001) and log-BNP values (4.8 ± 0.9 vs. 3.9 ± 1.2, P < 0.001) than those without LVAs [Table 2]. There was significant correlation between area on the left atrial surface and BNP levels (BNP, r = 0.28, p < 0.001; log-BNP, r = 0.35, p < 0.001). ROC curve analysis revealed that log-BNP was a good predictor of the prevalence of LVAs (area under the curve, 0.728) [Figure 2]. The optimal cut-off value of log-BNP was 4.4, which was equivalent to 81 pg/mL of BNP, corresponding to 76.3% sensitivity, 62.1% specificity, and 65.0% predictive accuracy.
Table 2. Predictors of LVAsa
| Variable |
All (n =183) |
LVAs |
Univariate analysis |
|
|
With(n = 38) |
Without(n =145) |
ORe [95% CIf] |
P value |
| Age, per 10-year increment |
6.7±0.9 |
7.1±0.7 |
6.6±1.0 |
2.2 [1.3, 3.7] |
0.002 |
| Female, n (%) |
49 (27) |
18 (47) |
31 (21) |
3.3 [1.6, 7.0] |
0.002 |
| Body mass index, kg/m2 |
24±3.8 |
23±3.6 |
24±3.8 |
0.9 [0.8, 1.04] |
0.19 |
| CHA2DS2-VASc score |
2.3±1.4 |
3.0±1.6 |
2.1±1.4 |
1.5 [1.2, 2.0] |
0.002 |
| Persistent AFb, n (%) |
82 (45) |
25 (66) |
57 (39) |
3.0 [1.4, 6.3] |
0.004 |
| Congestive heart failure, n (%) |
23 (13) |
9 (24) |
14 (10) |
2.9 [1.1, 7.4] |
0.03 |
| Hypertension, n (%) |
110 (61) |
23 (61) |
87 (60) |
1.02 [0.5, 2.1] |
0.95 |
| Diabetes mellitus, n (%) |
27 (15) |
5 (13) |
22 (15) |
0.8 [0.3, 2.4] |
0.76 |
| Log-brain natriuretic peptide |
4.1±1.2 |
4.8±0.9 |
3.9±1.2 |
2.4 [1.6, 3.6] |
< 0.001 |
| Log-brain natriuretic peptide>4.4c, n (%) |
84 (46) |
29 (76) |
55 (38) |
5.3 [2.3, 12] |
< 0.001 |
| eGFRd, per 10mL/min/1.73m2 increment |
8.1±2.4 |
5.9±1.2 |
6.5±1.6 |
0.8 [0.8, 0.9] |
< 0.001 |
| Left ventricular diastolic diameter, mm |
47±5 |
46±6 |
47±5 |
0.96 [0.9, 1.03] |
0.27 |
| Left ventricular ejection fraction, % |
64±9 |
63±10 |
65±8 |
0.98 [0.9, 1.02] |
0.22 |
| Left ventricular mass index, g/m2 |
97±88 |
88±26 |
99±97 |
0.997 [0.99, 1.01] |
0.55 |
| Left atrial diameter, mm |
39±7 |
41±7 |
39±7 |
1.04 [0.99, 1.1] |
0.11 |
| Mitral regurgitation ≥ mild, n (%) |
52 (28) |
19 (50) |
33 (23) |
3.4 [1.6, 7.1] |
0.001 |
aLVAs = low-voltage areas, bAF = atrial fibrillation, c This level of log-BNP is equivalent to 81 pg/mL of BNP. deGFR = estimated glomerular filtration rate, eOR = odds ratio, fCI = confidence interval. All values indicate mean±standard deviation unless otherwise indicated.
Figure 2. Association between brain natriuretic peptide and the prevalence of LVAs (a) LVAs are more frequently observed in patients with higher brain natriuretic peptide levels. (b) Receiver operating characteristic curve analysis reveals that brain natriuretic peptide is a good predictor of the prevalence of LVAs. The tangent (dotted line) to the curve intersects at a point corresponding to the cut-off value (asterisk). log-BNP: natural logarithm of brain natriuretic peptide, BNP: brain natriuretic peptide, LVAs: low-voltage areas, AUC: area under the curve.
Log-BNP was consistently higher in patients with LVAs than in those without LVAs, irrespective of the absence or presence of a history of heart failure (with heart failure, 5.3 ± 0.8 vs. 4.4 ± 1.0, P = 0.03; without heart failure, 4.7 ± 0.8 vs. 3.9 ± 1.2, P < 0.001).
Impact of ablation on BNP
Overall, log-BNP decreased after ablation (baseline, 4.2 ± 1.1; 6 months after ablation, 3.6 ± 1.0, P < 0.001). Moreover, log-BNP was reduced irrespective of AF recurrence and the prevalence of LVAs, except for patients without LVAs with AF recurrence [Figure 3].
Figure 3. Change in log-BNP before and 6 months after AF ablation (A) Among patients without AF recurrence at 6 months, log-BNP is significantly decreased in patients with and without LVAs. (B) Among patients with AF recurrence, log-BNP is significantly decreased in patients with LVAs. log-BNP: natural logarithm of brain natriuretic peptide, AF: atrial fibrillation, LVAs: low-voltage areas
Predictors of the prevalence of LVAs
Patients with LVAs were significantly older, more frequently female, and had persistent AF, higher CHA2DS2-VASc scores, higher log-BNP, lower estimated glomerular filtration rate and more frequent mitral regurgitation than those without LVAs [Table 2].
In the multivariate analysis, log-BNP >4.4, persistent AF, females, and aging were predictors of the prevalence of LVAs.
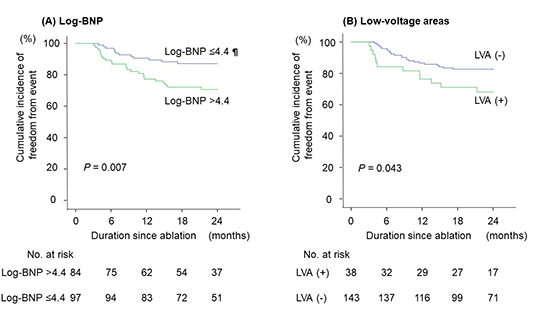
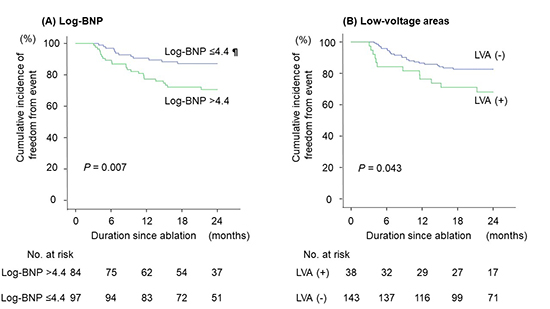
During the 24-month study period, 36 patients developed AF recurrence. Freedom from AF recurrence was significantly lower in patients with LVAs than in those without LVAs. Freedom from AF recurrence was also significantly lower in patients with log-BNP >4.4 than in those with log-BNP ≤4.4 [Figure 4].
Figure 4. Freedom from AF recurrence in patients with or without LVAs and high brain natriuretic peptide Freedom from AF recurrence is significantly lower in patients with high brain natriuretic peptide and those with LVAs than in patients without high brain natriuretic peptide and without LVAs, respectively. ¶ This level of log-BNP is equivalent to 81 pg/mL of BNP. log-BNP: natural logarithm of brain natriuretic peptide, AF: atrial fibrillation, LVAs: low-voltage areas
In this retrospective observational study, we analyzed 183 cases of AF ablation and investigated the association between the prevalence of LVAs and BNP level. The main findings were as follows: (1) LVAs were present in 21% of the total study population; (2) LVAs were more prevalent in patients with high BNP; and (3) freedom from AF recurrence was significantly lower in patients with log-BNP >4.4, which was equivalent to 81 pg/mL of BNP.
The association between high BNP levels and the prevalence of LVAs may be explained by the link between BNP and several factors that can cause atrial fibrosis and decrease endocardial voltage. First, increased left atrial wall stress caused by volume or pressure overload in the left ventricle and atrium can lead to left atrial fibrosis and BNP elevation.6 Second, neurohormonal abnormality is a well-recognized cause of myocardial fibrosis and has been shown to promote BNP secretion.10 Third, AF burden is associated with atrial fibrosis and BNP elevation,11-12 although the causal relationship between these factors has not been established. Finally, aging is also a factor associated with promoting myocardial fibrosis,13 and elderly people exhibit higher BNP levels than younger people.14
Change in BNP level before and after ablation
Log-BNP was significantly decreased in patients without AF recurrence for 6 months, irrespective of the presence or absence of LVAs. Even in patients with AF recurrence, log-BNP was reduced in patients with LVAs. However, patients without LVAs who experienced AF recurrence did not show a reduction in log-BNP.
A possible mechanism underlying the reduction in BNP levels after ablation may be that hemodynamics improves via the recovery of atrio-ventricular association and normal heart rate, and subsequent reduction in left ventricular filling pressure. Therefore, the degree of BNP decrease is expected to be maximal in patients with high baseline left ventricular filling pressure and no AF recurrence. This hypothesis would explain why no BNP decrease was observed in patients without LVAs who experienced AF recurrence but no increase in left atrial or left ventricular filling pressure.7-8
Patients with LVAs were significantly older, more frequently female, and more frequently had persistent AF, higher CHA2DS2-VASc scores, and more mitral regurgitation than those without LVAs, which is consistent with previous reports.15-17
Several factors, including AF duration and renal function, may have influenced LVAs.18 Even after adjusting for these factors, log-BNP was an independent predictor of the prevalence of LVAs. BNP might therefore compensate for other potential associated factors.
The prevalence of LVAs is associated with AF recurrence and the need for other forms of ablation in addition to PVI. A simple and non-invasive method for measuring BNP would enable the prediction of AF ablation outcomes, aid in determining the indication of catheter ablation and the need for additional ablations other than PVI.
Several limitations exist in this study. First, measurement of serum BNP levels performed before the procedure may be influenced by short-term hemodynamics, although we did exclude hemodynamically unstable patients such as those with decompensated heart failure. Second, as we conducted voltage mapping after completing PVI, the prevalence of LVAs might not have been precisely determined due to the presence of ablation lesions. Third, although contact force was used to confirm contact and we excluded low-voltage areas with < 5% across the total surface area of the left atrium, it could not be denied that LVAs by using ablation catheters were overestimated. Because ablation catheters produce larger LVAs measurements than multielectrode catheters.19 On the other hand, small LVAs might have been missed due to the limited resolution of voltage maps. Fourth, as this was a retrospective study, there were some differences in patient characteristics between the two groups, and mean left ventricular ejection fraction and left atrial diameter were normal. In addition, ablation strategy and patient followup methods were inconsistent among patients, and we performed only twelve-lead electrocardiogram and Holter electrocardiography to diagnose recurrence of AF. As a consequence, AF recurrence may have been biased and the results of this study should be carefully applied in clinical settings. Finally, statistical analyses were limited by the relatively small size of the study population.
Higher BNP levels were associated with the prevalence of left atrial LVAs and recurrence in AF patients undergoing catheter ablation.






