Complete AV Block Induced by Right Coronary Artery Spasm Following Radiofrequency Ablation for Atrial Fibrillation
Austin A. Howard1, Francia Rojas-Delgado2, Robert Schutt2, Jie Cheng1, Nilesh Mathuria1
1Texas Heart Institute..2Memorial Hermann Southwest Hospital, Houston, TX USA..
Coronary artery spasm during catheter ablation for arrhythmias is a rare but previously reported complication. Timing of presentation, manifestations of vasospasm, and purported mechanisms vary somewhat in the prior literature. We present a case of chest pain, inferior lead ST elevation, and complete AV block with angiographically confirmed right coronary artery (RCA) vasospasm that occurred immediately after catheter ablation for atrial fibrillation.
Key Words : Coronary Artery Spasm, AV Block, Atrial Fibrillation Ablation.
Correspondence to: Nilesh Mathuria MD
PO Box 20345
MC 2-225
Houston, TX 77225-0345
Catheter ablation for various arrhythmias may cause transient changes in autonomic tone. This may include acute changes in heart rate and/or blood pressure. We present a case of angiographically confirmed coronary vasospasm manifesting with inferior ST elevation, chest pain, and complete AV block developing immediately after radiofrequency (RF) ablation for atrial fibrillation. This phenomenon may represent a unique presentation of ablation related autonomic modulation.
A 56-year-old male with a history of symptomatic persistent atrial fibrillation (AF) and likely tachycardia-induced cardiomyopathy status post implantable cardioverter defibrillator (ICD) was admitted for AF ablation. The patient had documented left ventricular (LV) dysfunction since 2013 with initial left ventricular ejection fraction (LVEF) of 20-25%. Over time, with medical therapy the LVEF improved to 45-49% prior to ablation in 2018. Cardiac dimensions prior to ablation included LVEDD of 5.5 cm with volume of 137mL, LVESD 3.6 cm with volume of 74mL with LA volume index of 34mL/m2. The patient had no prior clinical history of Prinzmetal angina. The ablation strategy employed included pulmonary vein isolation with LA roof line with further posterior wall isolation. Radiofrequency ablation was performed with power ranging from 20-30W. There were no hemodynamic derangements as well as no periods of ablation related bradycardia during the procedure. Furthermore, no ablation was performed within the right atrium or SVC.
In the recovery unit, the patient complained of retrosternal chest pain that radiated to the jaw with associated hypotension. ECG demonstrated ST elevations in the inferior leads and third degree AV block with junctional escape rhythm [Figure 1]. Complete resolution of ECG abnormalities and normalization of vital signs was evident after atropine injection and after initiation of dopamine infusion [Figure 2]. Normal wall motion and preserved LV function without evidence of pericardial effusion was confirmed by echocardiogram.
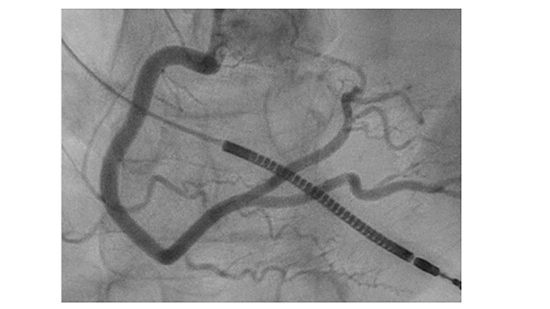
Urgent coronary angiography was performed which showed normal coronaries. There was no evidence of an acute obstructive lesion or thrombus. During the procedure, the patient once again developed chest pain and complete heart block with demonstration of severe vasospasm of the proximal RCA [Figure 3-Figure 4]. This resolved after multiple doses of intracoronary nitroglycerin and nicardipine. These findings were suggestive of vasospastic angina and patient was started on verapamil with no further episodes of heart block or ST changes. The patient has remained in sinus rhythm at 6 months post ablation without any clinical events related to coronary spasm.
Figure 1. ST segment elevation in inferior leads and complete heart block with junctional escape rhythm.
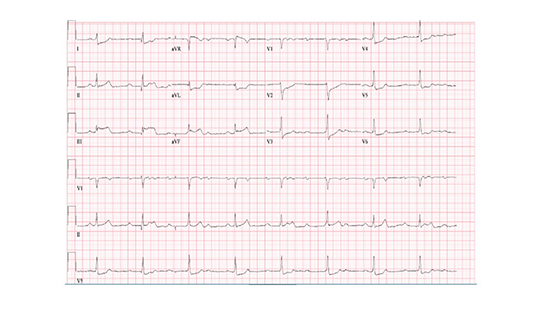
Figure 2. Resolution of ECG abnormalities after atropine injection and dopamine infusion.
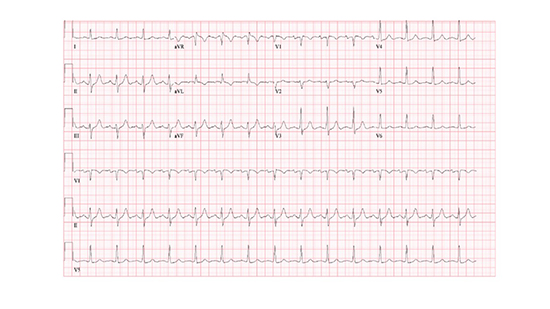
Figure 3. Severe spasm of proximal RCA.
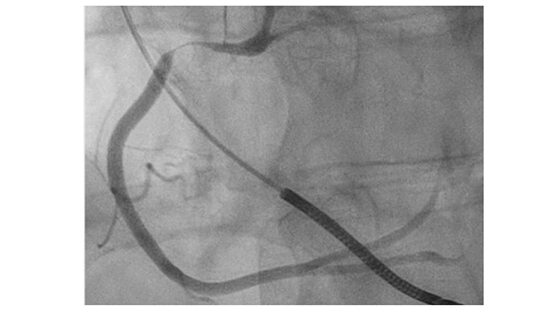
Figure 4. LAO image of proximal RCA after intracoronary nitroglycerin and nicardipine.
Apparent coronary ischemia during and following ablation has been attributed to several different mechanisms including air embolism [1], local catheter effects, and coronary vasospasm [2]. Coronary vasospasm has been noted both in those with traditional risk factors for vasospastic angina, i.e. tobacco use, in addition to those with no history of coronary vasospasm [3]. Given ablation and/or modification of left atrial ganglia during AF ablation, it has been proposed that a vagal mediated parasympathetic imbalance induced by ablation near ganglionated plexi surrounding the left atrium also may play a role in the vasospasm seen during ablation procedures [4], which may be exacerbated by anesthesia [5]. Aside from left atrial ablation lesions, prior reports describe similar responses (ST elevation, bradycardia, hypotension) during trans-septal puncture, possibly due to interatrial vagal network stimulation [6,7].
As to why this occurs, Kawakmi, et al. found that AF patients seem to have higher rates of drug provoked coronary spasm, implying baseline autonomic differences in AF patients. Spasm in our case was limited to the RCA, which has been suggested to be more susceptible to vagally mediated vasospasm than the left coronary system [8]. Signs and symptoms in prior reported cases have varied from transient with normal angiography [9] to cardiac arrest requiring cardiopulmonary resuscitation [10]. Complete heart block, as seen in our circumstances, has also been reported [5,6]. Additionally, the timing of onset appears to vary. Most cases in the literature have noted symptoms during the actual procedure, but symptoms in the post-operative period as in our case have been reported as well [9,11]. Most cases show good response with nitrates as was also seen in the presented case [12]. Of the cases evaluated in our literature search, no death or persistent morbidity were noted, although symptoms of frank syncope/aborted sudden death or new onset AV block may warrant evaluation for coronary spasm.
Aside from coronary spasm occurring after ablation at a distant site, multiple prior reports have described direct coronary spasm/injury from direct local catheter ablation. This includes RCA injury during cavotricuspid isthmus ablation for typical RA flutter and posterior descending artery injury during posteroseptal accessory pathway ablation and circumflex artery injury during LAA isolation. Given the sites of ablation and site of coronary spasm in the patient presented, a local ablation effect did not seem to apply.
Here, we present a case of inferior ST elevation and complete heart block presenting immediately following AF ablation due to right coronary artery spasm. This is a rare and potentially under-recognized complication of AF ablation and should be considered in patients post ablation with new onset AV block, ST elevation ECG pattern and/or unexplained syncope.






