Left Septal Fascicular Block Following Alcohol Septal Ablation for Hypertrophic Obstructive Cardiomyopathy
Enes Elvin Gul1, Andrés Ricardo Pérez-Riera2, Sohaib Haseeb3, Reda Abuelatta4, Adrian Baranchuk3
1Division of Cardiac Electrophysiology, Madinah Cardiac Centre, Madinah, Saudi Arabia.2Design of Studies and Scientific Writing Laboratory, ABC School of Medicine, Santo André,São Paulo, Brazil.3Division of Cardiology, Kingston Health Sciences Centre, Queen's University, Kingston, Ontario, Canada.4Department of Cardiology, Madinah Cardiac Centre, Madinah, Saudi Arabia.
Left septal fascicular block, or blockage of the middle fibers of the left bundle branch, is known to be suggestive of a critical proximal obstruction of the left anterior descending coronary artery before its first septal perforator branch. We describe the case of a 68-year-old male who exhibited this transient intraventricular dromotropic disturbance following alcohol septal ablation for hypertrophic obstructive cardiomyopathy.
Key Words : alcohol septal ablation, hypertrophic cardiomyopathy, left septal fascicular block.
Correspondence to: Enes Elvin Gul, MD
Consultant Cardiac Electrophysiologist
Division of Cardiac Electrophysiology
Madinah Cardiac Centre
Madinah, Saudi Arabia
Percutaneous alcohol septal ablation (ASA) has emerged as an alternative treatment to surgical myectomy for the reduction of left ventricular outflow tract (LVOT) gradient in hypertrophic obstructive cardiomyopathy (HOCM) [1].Several studies have reported high functional and hemodynamic success of ASA in symptomatic patients with HOCM [2-4]. Acute electro cardiographic changes seen in previous studies after ASA are right bundle branch block, ST-segment deviation, and Q wave formation[5,6]. We present a case of left septal fascicular block (LSFB) which appeared secondary to ASA for HOCM.
A 68-year-old male with previously known HOCM was admitted for ASA. At admission, the patient’s heart rate was 70 bpm and blood pressure was 106/68 mm Hg; there were no detectable murmurs or other cardiac signs. His laboratory test results were with in normal limits. Transthoracic echocardiography showed a preserved left ventricular (LV) systolic function (LVEF 50%) and severe concentric LV hypertrophy with LVOT obstruction. There was severe systolic anterior motion of the mitral valve and a peak pressure gradient across the LVOT of 120 mmHgat rest. There were no significant valvular abnormalities noted. A 12-lead electro cardiogram (ECG) obtained prior to the procedure showed sinus rhythm with left atrial enlargement, LV hypertrophy with a strain pattern, and a QRS duration of 85 ms [Figure 1]. The patient underwent a successful AS aprocedure and echocardiographic measurement demonstrated a significantly reduced peak LVOT gradient of 30 mmHg. An ECG obtained immediately after the procedure showed sinus rhythm with right bundle branch block (RBBB), left axis deviation, and prominent anterior QRS forces in the right precordial leads V1-V2 [Figure 2] and [Figure 3]. One day following the procedure, the patient’s clinical condition deteriorated and he was subsequently admitted to the coronary care unit (CCU). An ECG showed Mobitz type Iatrioventricular block with left posterior fascicular block and right axis deviation [Figure 4]. Echocardiography showed a slightly impaired LV systolicfunction (LVEF 40%) with no changes in the peak LVOT gradient (30 mm Hg). While in the CCU, the patient developed complete heart block. He was scheduled for atemporary pacemaker insertion but his clinical condition further deteriorated and he expired due to cardiogenic and septic shocks, in spite of efforts at resuscitation.
Figure 1. ECG obtained before the procedure.
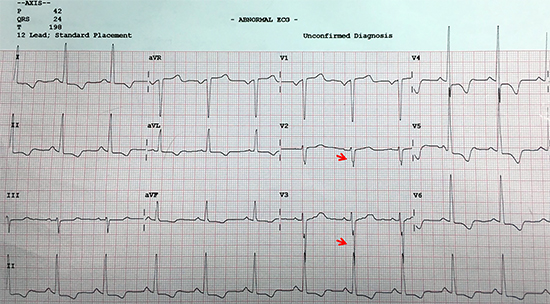
ECG diagnosis: P duration 120 ms, terminal mode negative of P in V1 > 40 ms, Morris index >0.04 mm/s, QRS axis +24°, QRS duration 85 ms, positive Sokolow-Lyon index >35 mm, strain pattern of repolarization, insinuation of fragmented QRS (red arrows). Conclusion: left atrial enlargement + left ventricular hypertrophy + fragmented QRS (fQRS on the surface ECG can be used as an indirect marker to predict the presence of fibrosis in HCM).
Figure 2. ECG obtained immediately after the procedure.
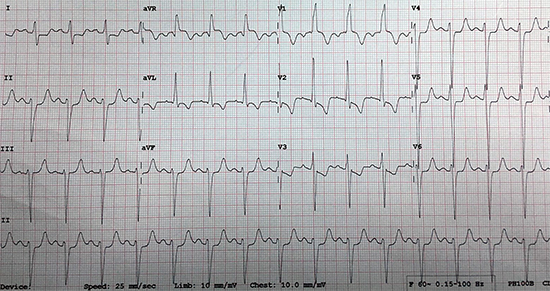
V1 LAE (Morris criteria + prolonged P duration = 120ms) + QRSd 120ms + ST-segment elevation followed by symmetric negative T-wave CRBBB + injury and ischemic. V2qRs pattern, prominent anterior QRS forces on right precordial leads V1-V2 “R-wave in crescendo” from V1 to V2 and decrescent from V2 to V6, prolonged R-wave peak time (> 40 ms) in V1-V2, R-wave voltage > 15mm and embryonic initial q wave in V1-V2 absence of q in I, V5-V6 consequence of absence of first septal vector. Conclusion: LAE + LVH + atypical LAFB + LSFB + RBBB (undescribed Trifascicular block: RBBB + left bifascicular block).
Figure 3. Typical ECG/VCG of LSFB in the frontal and horizontal plane.
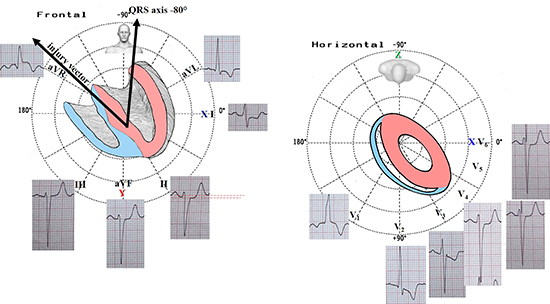
Note the ST-segment elevation in the unipolar lead aVR and concomitant ST-segment depression in lead II. The current injury vector pointing to lead aVR and consequently moves away from bipolar II, indicates proximal critical obstruction of the LAD before its first septal perforator branch or LMCA artery obstruction. This is compatible with the alcohol injection in this branch. Additionally, symmetric ischemic T waves are observed in II, III and aVF. Extreme left axis deviation -80°, SIII>SII atypical LAFB (why atypical? Because the absence of initial q wave in I. In the presence of typical LAFB, the 10-20 initial QRS forces are directed to +120°, originating initial r wave in III and concomitantly q wave in I.
Figure 4. ECG obtained one day after the procedure in the coronary care unit.
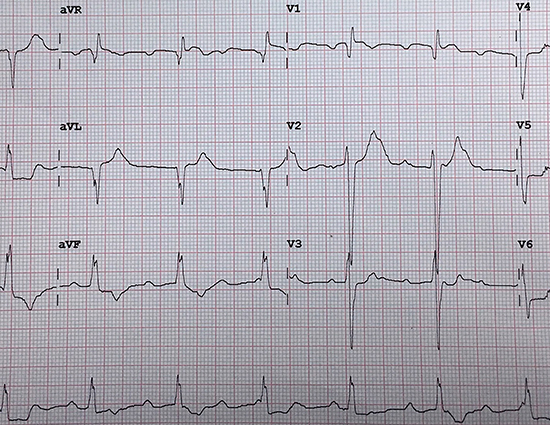
LAE+ LVH+ second-degree atrioventricular block Mobitz type I + left posterior fascicular block: QRS axis + 120°+ rS pattern in I + qR pattern in III and II, RIII>RII, prolonged R-wave peak time in aVF>45 ms; + localized septal infarction secondary to the procedure QR pattern in V1. PAFs disappear: transient LSFB.
We describe the case of a patient who developed transient LSFB following ASA for HOCM. Pérez Riera et al [7] previously analyzed the dromotropic disturbances (vector-electro cardiographic) and possible anatomic causes provoked by selective alcohol injection in the septal branch in 10 patients undergoing percutaneous treatment of HOCM. Prior to the procedure, 7 out of 10 patients had LV hypertrophy with a strain pattern, as reported in the present case.
The ECG criteria for LSFB have been previously defined [8-11].In the present case, all the criteria proposed in 2011 [8] were fulfilled [Table 1]. The presence of an intermittent pattern on ECG/VCG, as part of the requisites to recognize a new ECG dromotropic disturbance, is considered mandatory [12]. LSFB is one of the many causes that is responsible for the appearance of prominent anterior QRS forces in the horizontal plane (precordial leads). The transitory nature of the electro cardiographic findings, as seen in the present case, rules out the possibility of other causes for prominent anterior forces, such as normal variant, athlete’s heart,RBBB, obstructive and nonobstructive hypertrophic cardiomyopathy, erroneous placement of the precordial leads, vector cardiographic right ventricular hypertrophy, andothers as described else where [11].
The mechanism of LSFB following ASA can be explained with septal fibrosis following the alcohol injection. Septal fibrosis causes a predominance of RBBB, which differs from myectomy, that causes left bundle branch block [7]. In the present case, LSFB was accompanied with a typical left anterior fascicular block and complete RBBB with left axis deviation. However, the patient developed Mobitz type Iatrioventricular blockand the LSFB disappeared. We speculate that the transient appearance of LSFB with prominent anterior forces could be a sign of new onset acute coronary syndromeand should raise the suspicion of a critical obstruction of the left anterior descending (LAD) coronary artery before the first septal perforator branch [13], as a complication of ASA. However, this could not be diagnosed on time as the patient’s clinical condition dramatically deteriorated and the patient expired.
Table 1. Diagnostic criteria of left septal fascicular block.
| Criteria for LSFB |
Presence in the case |
| Presence of PAF of QRS |
Yes |
| Normal QRS duration or discrete increase when not associated with other blocks |
Yes |
| Unaltered frontal plane leads when isolated |
Yes |
| Prolonged R-wave peak time in V1 and V2 ≥ 40 ms |
Yes |
| R-wave voltage in V1 ≥ 5 mm |
Yes |
| R/S ratio in V1 and V2 > 2 |
Yes |
| S-wave depth in V2 < 5 mm |
Yes |
| Embryonic and/or transient q wave in V2 or V1 and V2 |
Yes |
| R-wave voltage in V2 ≥ 15 mm |
Yes |
| RS or Rs patterns in V2 and V3 with R-wave “in crescendo” from V1-V3 and decreasing from V5-V6 |
Yes |
| Absence of q wave in V5, V6 and lead I |
Yes |
We present a case of transient LSFB following ASA for HOCM. This clinical scenario should raise the suspicion of a critical proximal LAD occlusion before the first septal perforator branch. Physicians should be attentive to this pattern for the need of immediate coronary angiography.






