Left Atrial Appendage Morphology as a Determinant for Stroke Risk Assessment in Atrial Fibrillation Patients: Systematic Review and Meta-Analysis
Abu Rmilah Anan1, Jumah Fareed 2, Jaber Suhaib 3, Roubi Rafat 4, Daana Murad 4, Bsisu Isam5, Muamar Tariq 6, Erwin Patricia 1, Egbe Alexander 1, Vaibha Vaidya 1, Noseworthy Peter A 1, Deshmukh Abhishek1
1Department of Cardiovascular Diseases, Mayo Clinic, Rochester, MN, USA.2Rutgers-Robert Wood Johnson Universty Hospital, New Brunswick, NJ, USA.3Cairo University Hospital, Egypt.4Hadassah Medical Center, Jerusalem, Israel.5Jordan University Hospital, Amman, Jordan.6Zarqa New Hospital, Zarqa, Jordan.
Atrial fibrillation (AF) is a leading source of emboli that precipitate cerebrovascular accident (CVA) which is correlated with left atrial appendage (LAA) morphology. We aimed to elaborate the relationship between CVA and LAA morphology in AF patients.
Medline and EMBASE databases were thoroughly searched between 2010-2018 for studies that included atrial fibrillation patients and classified them into two groups based on CVA occurrence. Four different LAA morphologies (Chicken wing CW, Cauliflower, cactus and windsock) were determined in each group by 3D TEE, MDCT or CMRI. New Castle Ottawa Scale was used to appraise the quality of included studies. The risk of CVA before cardiac ablation and/or LAA intervention in CW patients was compared to each type of non-CW morphologies. The extracted data was statistically analyzed in the form of forest plot by measuring the risk ratio (RR) using REVMAN software. P value and I square were used to assess the heterogeneity between studies.
PRISMA diagram was illustrated showing 789 imported studies for screening. Three duplicates were removed, and the rest were arbitrated by 2 reviewers yielding 12 included studies with 3486 patients including 1551 with CW, 442 with cauliflower, 732 with cactus 765 with windsock. The risk of CVA in CW patients was reduced by 41% relative to non-CW patients (Total RR=0.59 (0.52-0.68)). Likewise, the risk of CVA in CW patients was less by 46%, 35% and 31% compared to cauliflower (Total RR =0.54(0.46-0.64)), cactus (Total RR =0.65(0.55-0.77)) and windsock (Total RR =0.69(0.58-0.83)) patients respectively. Low levels of heterogeneity were achieved in all comparisons (I square <35% and p value > 0.1).
Patients with non-CW morphologies (cauliflower, cactus and windsock) show a higher incidence of CVA than CW patients. For that reason, LAA appendage morphology could be useful for risk stratification of CVA in AF patients.
Key Words : Atrial fibrillation, Left atrial appendage, Stroke.
Correspondence to: Abu Rmilah, Anan MD
Division of cardiovascular disease
Mayo Clinic, 200 1st St SW, Rochester, MN 55905
Atrial fibrillation AF is the most common sustained arrhythmia with an estimated prevalence of 1-1.5% in the general population and up to 10% in the elderly.[1-3] AF has been associated with significant morbidity, mortality, and healthcare resource utilization and costs.[4][5]AF is associated with a five-fold increase in the risk of cardioembolic stroke,[5]and is implicated in approximately 25% of strokesin patients over 80 years of age.[5]
Stroke preventionis a top clinical priority and a focus of ongoing investigation.The left atrial appendage (LAA) has been implicated in more than 90% of cardioembolic strokes in AF.[6-8]The anatomic characteristics of the LAA could underlie some of this risk and could be particularly important in identifying patients with lowerCHA2DS2-VASc score that would benefit from thromboprophylaxis.[6-8]One of these features is the LAA morphology or shape. Four different types of LAA morphology: 1) chicken wing 2) wind sock 3) cauliflower and 4) cactus. These morphologies can be defined by echocardiography, cardiac computed tomography (CT) or cardiac magnetic resonance imaging (CMRI).[9]
For that purpose, we aimed to perform a systematic review/meta-analysis study to summarize and statistically analyze the prevalence of stroke/TIA associated with each type of LAA morphology. We aimed to determine whether there is an association between the risk of TE and the shape of LAA in patients with AF,especially those with low CHA2DS2-VASc score.
Ovid MEDLINE database from 1946 to November 29, 2018 and Embase database from 1988 to November 29, 2018 were searched by a professional librarian (PE) for all articles that addressed LAA morphology in patients with AF and were published between January 2010 and November 2018. The following keywords were used to perform the literature search: (atrial fibrillation OR AF) AND (left atrial appendage OR LAA OR left atrial appendage morphology OR left atrial appendage anatomy, OR left atrial appendage geometry OR left atrial appendage shape, OR left atrial appendage hemodynamic) AND (stroke, transient ischemic attack, cardioembolic event, thromboembolism, or cerebrovascular attack) AND (cardiac magnetic resonance imaging OR 3D transesophageal echocardiography OR multi gated cardiac computed tomography). Furthermore, we reviewed references listedin bibliographies of two comprehensive review articles to ensure that all relevant studies were included in our search.[10,11]
Study design and Selection criteria
We performed a systematic review/meta-analysis in accordance with PRISMA guidelines. A PRISMA-style flow diagram was prepared to clarify the total number of references retrieved by search and how many articles were excluded during the screening process and the final number of included studies utilized for data extraction.
All the references were imported to Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia)and then underwent an accurate screening process by two independent reviewers (AA and JF) based on title and abstract followed by full text review to determine the final included studies for data extraction. Any discrepancies were resolved by discussing with a third independent reviewer (DA).
All included studies met the following criteria: 1) included patients with AF in whom multi-gated cardiac CT, CMRI or (3D TEE) were carried out before a cardiac ablation, 2) LAA morphology characteristics were obtained, 3) all patients were classified according to the shape of LAA, and 4) the rate of cardioembolic stroke/TIA was documented in each LAA appendage shape.
Studies thatwerepublished before January 2010, not published in English, limted to imaging results after cardiac ablation, basic science/animal studies, review articles, case reports, pediatric studies, included pregnant patients, commentaries, editorials, conference papers or posters were excluded from our review.
Three independent authors (AA, JF, and JS) participated in data extraction using standardized protocol and reporting forms. Any discordanceswere resolved by consensus with the fourth reviewer (DA).Demographics (sample size, age, gender and smoking status), clinical characteristics (hypertension, diabetes mellitus, hyperlipidemia, CHA2DS2 or CHA2DS2-VASc score), employed imaging modality (multi gated cardiac CT, CMRI or (3D TEE)), type of LAA shape (chicken wing (CW), non-chicken wing which includes cactus, cauliflower and windsock) and number of strokes in each shape were extracted.
Newcastle-Ottawa quality assessment scale (NOS)[12] was utilized to appraise the quality of all included studies. The checklist form for cohort studies of NOS was considered for our assessment. It consists of three categories: Selection which contains four subcategories (representativeness of the exposed cohort, selection of the non-exposed cohort, ascertainment of exposure and demonstration that outcome of interest was not present at start of study), comparability (are cohort groups compared to study controls) and outcome which comprises of three subcategories (assessment of outcome, was follow-up long enough for outcomes to occur?, adequacy of follow-up of cohorts). Studies werethen classified into one of three categories: a) goodquality 6-7 points b) fair quality 3-5 points and c)poor quality 0-2 points.
Continuous variables were expressed as means and standard deviations (SD), whereas dichotomous and categorical variables were presented as number of cases (n) and percentages (%).Review Manager (RevMan 5.3;Copenhagen, Denmark)[13]was employed to execute the statistical meta-analysis in the form of forest plots. In our analysis, data were analyzed using Cochran-Mantel-Haenszel Estimate for a Risk Ratio(RR) in the fixed-effects model.[14], A confidence interval of 95 % (95% CI)was selected for the effect size. Heterogeneity was assessed by Chi-square, and I2 tests, and publication bias was determined using funnel plots. Homogeneity was indicated when p-value > 0.1 and I square <50% [15] and absence of publication bias was defined when all studies (dots) exist within the funnel in a symmetrical manner.
We prepared four forest plots to evaluate the risk of stroke/TIA between chicken wing and non-chicken groups and chicken wing versuseach of the subtypes of non-chicken wing morphology.
Our literature search yielded 789 references which were imported to Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). Three duplicates were removed, and 786 articles entered the title and abstract screening process. Subsequently, 714 articles were irrelevant, and 72 studies were assessed for final eligibility by reviewing thefull-text version. As a result, twelve studies fulfilled the inclusion criteria and were included in data extraction and meta-analysis, whereas 50 studies were excluded due to the following reasons: wrong outcomes in 42 studies, wrong patient population in 2 studies, wrong study design in one study, two non-English articles, three conference papers.
Demographics and clinical characteristics
We analyzed3,486 patients whom their data were included and analyzed in our meta-analysis. [Table 1] shows the demographics and characteristics of all included patients. Male gender wasnoted in 72.3% of the final sample. The mean age was 60.6 years old. About 49.5 % (in eleven studies only) and 15 % (in nine studies) were having hypertension and diabetes mellitus respectively. LAA morphology was determined by multi gated cardiac CT in eleven studies, CMRI in one study and (3D TEE) in three studies. The overall prevalence of cardioembolic stroke in the studied population was 20 (n = 696). [Table 2] describes thedemographics and general characteristics of all included patients.
Table 1. Demographics and general characteristics of all included patients.
| Author/year |
Type of study |
Sample Size |
Male |
Age |
DM |
HTN |
Hyperlipidemia |
Patients with CHADS2 ≥2 |
Patients with CHA2DS2-VASc≥2 |
Stroke/TIA |
Imaging |
| Di Biase 2012(25) |
Prospective |
932 |
734
(78.8%)
|
59 ±10 |
40(4.3%) |
450 (48.3%) |
218 (23.4%) |
127 (13.6%) |
N/A |
78 (8.4%) |
MDCT (433) or MRI (499) |
| Khurram 2013(20) |
Retrospective |
678 |
507 (74.8%) |
59±9.7 |
44 (6.5%) |
327 (48.4%) |
N/A |
113 (16.6%) |
274 (40.4 %) |
65 (9.6%) |
MDCT |
| Kimura 2013(26) |
Retrospective |
80 |
66 (82.5%) |
58.6 ± 6 |
N/A |
N/A |
N/A |
11 (13.8 %) |
N/A |
30 (37.5%) |
MDCT |
| Kong 2014(27) |
Retrospective |
219 |
143 (65.3%) |
59
±7.5
|
19 (8.7%) |
80 (36.5%) |
N/A |
15 (7%) |
77 (35.2%) |
26 (11.9%) |
MDCT |
| Kosiuk 2014(28) |
Retrospective |
85 |
50 (58.8%) |
64 ±11 |
19 (22%) |
63 (74.1%) |
N/A |
N/A |
Median: 3 (2-4) |
23 (27.05%) |
MDCT |
| Lee 2014(29) |
Retrospective |
218 |
166 (76.4%) |
61±9.5 |
33 (15%) |
113 (51.8%) |
49 (22.5%) |
N/A |
Mean: 1.5 +/-1.2 |
67 (30.7%) |
MDCT |
| Fukushima 2015(24) |
Retrospective |
96 |
72 (75 %) |
59 ±10.2 |
12 (13%) |
46 (47.9%) |
34 (35.4%) |
19 (19.8%) |
19 (19.8%) |
10 (10.4%) |
3D-TTE MDCT |
| Kelly 2017(30) |
Retrospective |
332 |
278 (83.7%) |
55 ±13 |
48 (15%) |
200 (60.2%) |
N/A |
N/A |
162 (48.8%) |
16 (4.8%) |
MDCT |
| Nedios2015(31) |
Retrospective |
100 |
88 (88%) |
55 ±9 |
N/A |
46 (46%) |
23 (23%) |
0 (0%) |
0 (0%) |
25 (25%) |
MDCT |
| Petersen 2015 (32) |
Retrospective |
131 |
86 (65.6%) |
68±11.6 |
23 (18%) |
62 (47.3%) |
N/A |
N/A |
82 (62.7%) |
16 (12.2%) |
3D-TEE |
| LEE 2015(23) |
Retrospective |
360 |
302 (63.7%) |
64 ± 7 |
77 |
224 62.2% |
75 (20.8%) |
N/A |
Mean: 1.75 +/-1.15 |
160 (44.44%) |
3D-TEE
MDCT
|
| Lee 2017(33) |
Retrospective |
255 |
150 (58.8%) |
65 ±7 |
33 (13%) |
55 (21.6%) |
N/A |
95 (37.25%) |
95 (37.25%) |
170 (66.7%) |
MDCT |
Table 2. The distribution of different LAA shape with number and percentage of stoke events in each shape.
| Author/year |
Sample Size |
Chicken Wing |
|
Cauliflower |
|
Cactus |
|
Windsock |
|
|
|
Total number |
Stroke patients |
Total number |
Stroke patients |
Total number |
Stroke patients |
Total number |
Stroke patients |
| Di Biase 2012 (25) |
932 |
451 |
20 (4.4%) |
24 |
4 (16.7%) |
278 |
35 (12.6%) |
179 |
19 (10.6%) |
| Khurram 2013 (20) |
678 |
306 |
24 (7.8%) |
68 |
11 (16.17%) |
125 |
15 (12%) |
179 |
15 (8.38%) |
| Kimura 2013 (26) |
80 |
14 |
3 (21.4%) |
32 |
18 (56.3%) |
4 |
2 (50%) |
30 |
7 (23.3%) |
| Kong 2014 (27) |
219 |
114 |
6 (5.26%) |
29 |
7 (24.13%) |
24 |
3 (12.5%) |
52 |
10(19.2%) |
| Kosiuk 2014 (28) |
85 |
25 |
5(20%) |
30 |
13 (43.3%) |
19 |
4 (21.05%) |
11 |
1 (7.7%) |
| Lee 2014 (29) |
218 |
110 |
33 (30%) |
22 |
7 (31.8%) |
24 |
7 (29.2%) |
62 |
20 (32.3%) |
| Fukushima 2015 (24) |
96 |
12 |
1 (8.3) |
16 |
3 (18.8) |
37 |
4 (10.8) |
31 |
2 (6.5%) |
| Kelly 2017 (30) |
332 |
190 |
9 (4.7%) |
44 |
4 (9%) |
15 |
0 |
83 |
3 (3.6%) |
| Nedios 2015 (31) |
100 |
32 |
6 (19) |
40 |
11 (28) |
18 |
5 (28) |
10 |
3 (30%) |
| Petersen 2015 (32) |
131 |
56 |
6 (10.7%) |
11 |
0 |
20 |
4 (20%) |
44 |
16 (13.6%) |
| LEE 2015 (23) |
360 |
155 |
55 (35.4%) |
50 |
29 (58%) |
108 |
52 (49.48 %) |
47 |
24 (51.06%) |
| Lee 2017 (33) |
255 |
86 |
41 (47.6%) |
72 |
66 (91.67%) |
60 |
41 (68.33%) |
37 |
22 (59.4%) |
| Total |
3486 |
1551 |
209 (13.5%) |
438 |
173 (39.4%) |
732 |
172 (23.5%) |
765 |
142 (18.6%) |
LAA morphology and cardioembolic stroke/TIA rate
All patients were classified into four groups based on the shape of the LAA. Chicken wing (CW), cauliflower, cactus and windsock morphologies were indentified in 1551, 442, 732, and 765 patients respectively.
In terms of the distribution of cardioembolic stroke/TIA events among different groups, 209 of 1,551 CW patients (13.5%) developed stroke whereas 487 of 1,935non-CW patients (25.2%) developed stroke events. Among non-CW patients, stroke events were reported in 173 of 438 cauliflower patients (39.4%), 172 of 732 cactus patients (23.5%) and 142 of 765 windsock patients (18.6%). Table 3 demonstrates the distribution of different LAA shapes with number and percentage of stoke events in each shape
As shownin [Figure 2] the risk of cardioembolic stroke/TIA in CW patients was associated with 41% fewer events relative to non-CW patients (Total RR=0.59; 95% CI [0.52-0.68]).On comparison with each type of non-CW shape, we found that the risk of cardioembolic stroke/TIA in CW patients was less by 46%, 35%, 31% compared to cauliflower ([Figure 3]; total RR =0.54; 95% CI [0.46-0.64]), cactus ([Figure 4]; total RR =0.65; 95% CI [0.55-0.77]), and windsock ([Figure 5]; total RR =0.69; 95% CI [0.58-0.83]) respectively.
Homogeneity was achieved in all analyses (p value = 0.19 and I square = 26 % in [Figure 2], p value = 0.48 and I square = 0% in [Figure 3], p value = 0.57 and I square = 0% in [Figure 4] and p value = 0.14 and I square = 32% in [Figure 5]).
In accordance with the scoring system of NOS, all studies scored three stars on selection category, two stars on comparability and one star on the outcome. Thereby, all studies were regarded as good quality studies, and none of them were of fair or poor-quality.
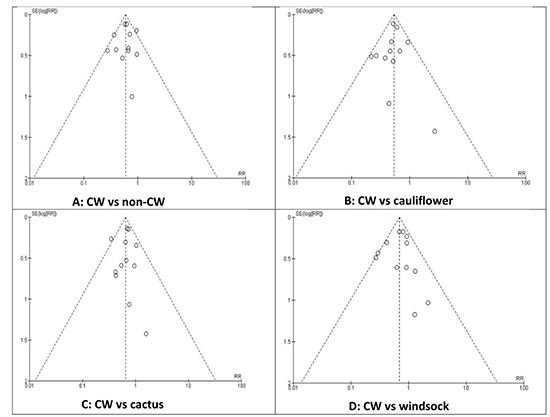
The meta-analysis of CW vs non-CW, CW vs cauliflower, CW vs cactus, and CW vs windsock demonstrated a symmetrical distribution of all included studies on either side of ther overall effect line (RR line) in funnel plots and therefore appear to reflect no significant publication bias in the study literature. [Figure 6] demonstrates the funnel plots for all comparisons.
Figure 1. The PRISMA flow diagram and summarizes the process search strategy.
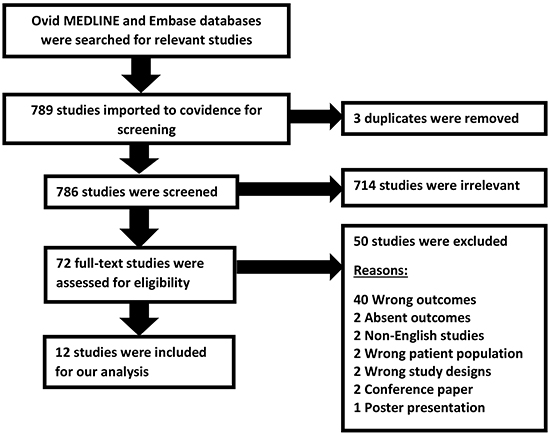
Figure 2. Forest plot compares the risk of cardioembolic events (stroke, TIA) between CW patients and non-CW patients.
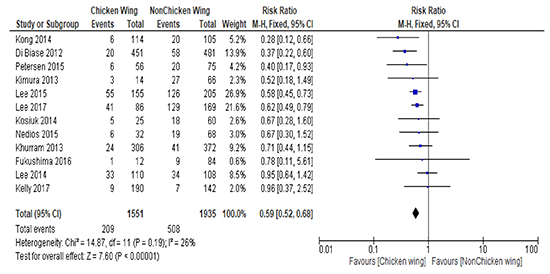
Figure 3. Forest plot compares the risk of cardioembolic events (stroke, TIA) between CW patients and cauliflower patients.
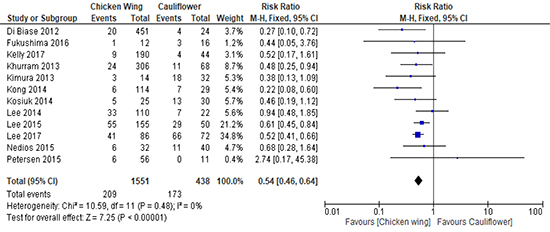
Figure 4. Forest plot compares the risk of cardioembolic events (stroke, TIA) between CW patients and cactus patients.

Figure 5. Forest plot compares the risk of cardioembolic events (stroke, TIA) between CW patients and windsockpatients.
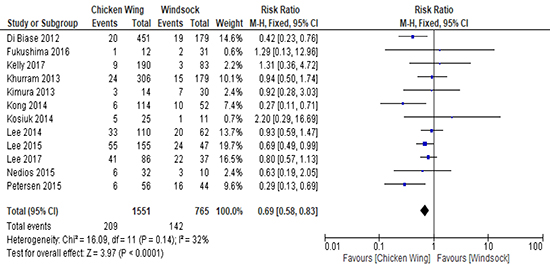
Figure 6. Funnels plots for detecting the publication bias for all comparisons.
The main goal of our study was to assess the risk of cardioembolic stroke in patients with AF based on different morphologies of the LAA. Theincluded studies enrolled a totalof 3,486 patients who underwent cardiac CT, MRI or TTE to evaluate the LAA characteristics prior to cardiac ablation and all studies reported rates of cardioembolic stroke/TIA according to LAA morphology. Our main findings suggesteda ‘chicken wing’ morphologywas associated withfewerthromboembolic events compared to the other morphologies. Among non-CW morphologies, the cauliflower shape poses the highest risk rate of thromboembolic events followed by cactus and windsock, in descending order.
It is well known that AF is a strong precipitating factor for the development of embolic stroke, and thus necessitating a thromboembolic prophylaxis. CHA2DS2-VASc scoring system has been widely employed as the most precise tool to stratify the risk of stroke in AF patients. CHA2DS2stands for (Congestive heart failure (1 point), Hypertension (1 point), Age ( > 65 = 1 point, > 75 = 2 points), Diabetes (1 point), previous Stroke/transient ischemic attack (2 points).[16] According to this score, all guidelines have advised against prophylactic anticoagulant for low risk patients who are defined as patients with score of 0 whereas thromboprophylaxis is recommended for high risk patients who achieved 2 points or more. Aside from that, there is still a sort of inconsistency between guidelines in deciding whether intermediate risk patients with score 1 need thromboprophylaxis or not. For those patients, oral anticoagulant is recommended according to the American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines 2014 [17] whereas female gender as the sole risk factor is the only exception based on the European Society of Cardiology Class IIaRecommendation 2016 [18]. Therefore, these conflicts foster the necessity for adding other factors that could help in the decision-making for thromboprophylaxis in intermediate-risk patients.
Anatomical, morphological and hemodynamic abnormalities in LAA occur in setting of AF. Increased stasis, endothelial dysfunction, and tissue injury due to comorbidities associated with AF as attributed by Virchow’s triad result in thrombus formation and subsequent stroke.
Based on the findings of our analysis, we strongly believe that different shapes of LAA are associated with different stroke risk rates in patients with AF. Non-CW shape, especially cauliflower is considered a risk factor for stroke development in those patients. Thereby, the addition of such a factor in stratifying the risk of stroke would be highly beneficial and facilitate the decision-making regarding thromboprophylaxisespecially in low CHA2DS2-VASc score.
On the other hand, several morphological and functional abnormalities including LAA orifice area, LAA depth, LAA volume and LAA flow velocity have been studied in several observational studies.[19-24] It has been shown that the increase in LAA orifice area, depth and volume and decrease in LAA velocity are strongly associated with increased stroke risk in AF.[19-24] These changes are attributable to blood pooling and stasis triggered by AF itself. Therefore, a systematic review and meta-analysis of all studies that address these parameters should be done in order to demonstrate the final association between these variables and the risk of embolic stroke and try to find a cut-off values that could help in assessing the risk of thromboembolism in AF patients. Importantly, CW morphology has been associated with a smaller LAA orifice area (p=0.013) and higher LAA emptying velocity (p<0.001) compared to non-CW shape [23]. These results further confirm the importance of non-CW shape as a predictor for the emergence of cardioembolic stroke in AF patients.
In summary, patients with non-CW morphologies (cauliflower, cactus and windsock) were associated witha higher incidence of embolic stroke/TIA than CW patients. LAA appendage morphology maybe useful inrisk stratification of thromboembolic events and decision-making regarding thromboprophylaxis in AF patients.
Patients with non-CW morphologies (cauliflower, cactus and windsock) show a higher incidence of CVA than CW patients. For that reason, LAA appendage morphology could be useful for risk stratification of CVA in AF patients.






