Low-voltage areas as alternative targets for the ablation of unmappable atrial tachycardia in patients undergoing atrial fibrillation ablation
Masaharu Masuda1, Mitsutoshi Asai1, Osamu Iida1, Shin Okamoto1, Takayuki Ishihara1, Kiyonori Nanto1, Takashi Kanda1, Takuya Tsujimura1, Yasuhiro Matsuda1, Shota Okuno1, Toshiaki Mano1
1Kansai Rosai Hospital Cardiovascular Center, 3-1-69 Inabaso, Amagasaki, Hyogo 660-8511, Japan.
Unmappable regular atrial tachycarrhythmias (ATs) occasionally develop during atrial fibrillation (AF) ablation, and are difficult to treat by conventional ablation. Recently, low-voltage areas (LVAs) have been reported to represent AT substrate. The purpose of this study was to elucidate the efficacy of LVA ablation for unmappable AT.
This observational study included 32 consecutive patients who developed unmappable ATs during and after AF ablation. Unmappable AT was defined as AT lasting for >5 s, but that terminated or changed the activation sequence over too short a time to create a sufficient activation map. We used conventional ablation to target undetermined AT circuits estimated from activation timings of electrograms recorded on the placed electrode catheter, the response to entrainment mappings, and/or diastolic potentials during AT. Subsequently, in cases without successful elimination of unmappable ATs by conventional ablation, LVA (≤ 0.5 mV) ablation was performed at the discretion of the operators.
Conventional ablation failed to eliminate at least one unmappable AT in 29 patients. Among them, LVA ablation was performed in 16 patients. LVA ablation eliminated all the unmappable ATs in 8 of 16 patients. The LVA size did not differ between patients with and without the acute elimination of unmappable ATs (17±11 vs. 21±12 cm2, p = 0.39), and AT/AF recurrence rates were comparable between the two groups (38% vs. 63%, p = 0.62) during a mean follow-up period of 14±8 months.
LVA ablation was efficacious to some extent for the elimination of unmappable ATs refractory to conventional ablation.
Key Words : Low-voltage area, Unmappable atrial tachyarrhythmia, Atrial fibrillation.
Masaharu Masuda
Kansai Rosai Hospital Cardiovascular Center
3-1-69 Inabaso, Amagasaki-shi, Hyogo 660-8511, Japan
Catheter ablation has become an established therapy for atrial fibrillation (AF). However, many patients experience atrial tachyarrhythmias even after AF ablation, including not only recurrent AF but also regular atrial tachyarrhythmias (AT). As far as an AT is stable, the AT circuit is easily visualized using a 3-dimensional electroanatomical mapping system, and the ablation targeting the earliest activation site for centrifugal AT or the linear ablation interrupting the reentrant circuit for macro-reentrant AT are effective for AT elimination.1, 2 However, if an AT is too unstable to create an activation map and/or to allow performance of an entrainment study, the entire activation circuit cannot be entirely defined. In such a case, conventional ablation targeting an undetermined AT circuit can rarely eliminate all the unmappable ATs.
Recently, left atrial (LA) low-voltage areas (LVAs) have been reported to correlate well with recurrent atrial tachyarrhythmias after pulmonary vein isolation (PVI) in patients with AF.3-5 LVA ablation in addition to PVI has been shown to result in better procedural outcomes than PVI alone.3 We recently reported that stable macro-reentrant ATs induced after PVI depended on the distribution of LVAs, and that most slow-conduction isthmuses might be located within LVAs.6
We hypothesized that some parts of critical substrates of unmappable ATs, such as a slow-conduction isthmus, are located within LVAs, and that LVA ablation could eliminate unmappable ATs. The purpose of this study was to assess the efficacy of LVA ablation on unmappable ATs refractory to conventional ablation.
This observational study enrolled consecutive AF patients who developed unmappable ATs after AF ablation at Kansai Rosai Hospital from December 2014 to April 2017. Unmappable AT was defined as an AT that lasted for > 5 s, and terminated or changed the activation sequence over too short a time to allow creation of an activation map to identify the ablation target (Figure 1 and Figure 2). Patients in whom ablation targeting undetermined unmappable AT circuits (conventional ablation) failed to eliminate at least one unmappable AT were divided into two groups according to whether they had received LVA ablation. The discretion to perform LVA ablation was made by the attending operators considering the operation time, patient condition, and other clinical factors. A patient flow chart is shown in Figure 3.
Figure 1. A representative case with complete voltage homogenization
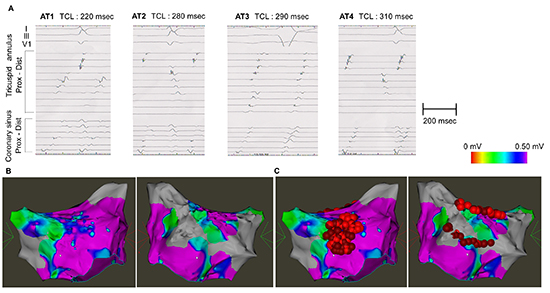
A case (#15 in Table 2) with 4 unmappable ATs after pulmonary vein isolation (A). LVAs were distributed in the septal and posterior regions (B). Conventional ablation failed to eliminate some unmappable ATs. LA LVA ablation achieved complete voltage homogenization (C). However, some unmappable ATs were still inducible even after the LVA ablation.
Exclusion criteria were age < 20 years, prior cardiac surgery, and prior LVA ablation. This study complied with the Declaration of Helsinki. Written informed consent for the ablation and participation in the study was obtained from all patients, and the protocol was approved by our Institutional Review Board.
Catheter ablation was performed by two experienced operators (MM and TK) with the patient under intravenous sedation with dexmedetomidine. A 6-Fr decapolar electrode was inserted into the coronary sinus while a second 6-Fr decapolar electrode was placed in the right atrium. Following a transseptal puncture at the fossa ovalis, two long sheaths (Agilis® and SL0®, St. Jude Medical, St. Paul MN, USA) were introduced into the left atrium. A 20-pole circular catheter was placed in a pulmonary vein via the SL0® sheath. Subsequently, the operators performed mapping and ablation guided by an electroanatomical mapping system (Carto3®; Biosense Webster, Diamond Bar CA, USA; or Rhythmia®, Boston Scientific, Marlborough [Cambridge] MA, USA).
In initial AF ablation, extensive encircling PVI was performed first. A dragging technique was employed to perform circumferential ablation around both ipsilateral pulmonary veins using an open-irrigated ablation catheter with a 3.5-mm tip (Thermocool SmartTouch® or Thermocool Celsius®, Biosense Webster) via the Agilis® or SL0® sheath (St. Jude Medical). Radiofrequency energy was applied for 30 s (15 s at the posterior LA wall near the esophagus) at each site using a maximum temperature of 42°C and maximum power of 35 W. The irrigation rate was 8 or 17 mL/min. Operators attempted to maintain an appropriate contact force between the catheter and endocardium of between 5 and 20 g, if contact force measurement was available. PVI was considered complete when both entrance and exit blocks were created. In patients undergoing a repeat ablation procedure, the conduction blocks of the previous PVI and other previous linear ablations were confirmed. If a block line was reconnected, additional point-by-point ablations were performed at the conduction gap sites. Non-pulmonary-vein AF triggers were attempted to be ablated guided by P-wave morphology and activation sequence of intracardiac electrogram recording.[7]
A voltage map using a 3.5-mm ablation catheter (Thermocool SmartTouch®, Biosense Webster), 20-pole circular catheter with 1mm-electrode, or 64-pole mini-basket catheter with 0.4-mm2 print electrode (Orion®, Boston Scientific) was created after PVI. Mapping was performed throughout the entire LA during sinus rhythm in principle; however, AT or AF rhythms were allowed when sinus rhythm could not be maintained. In addition, high-density mapping was performed at sites where LVAs had been detected to delineate the extent of each LVA. We confirmed adequate endocardial contact by stable electrograms, the distance to the geometric surface, and if available, contact force ≥ 5 g. The band pass filter was set at 30–500 Hz. Bipolar peak-to-peak voltage at each acquired point was measured. We defined LVAs as sites ≥ 5 cm2 demonstrating local bipolar voltage ≤ 0.50 mV.
Induction, mapping and ablation of ATs after the PVI
The induction of AT was performed with burst pacing from the electrodes placed in the right atrial (RA) appendage and from those in the LA appendage sequentially. Constant burst pacing was performed for 5 s at each cycle length starting with 300 ms and decrementing by 20 ms to 200 ms or the shortest cycle length that resulted in 1:1 atrial capture at an amplitude of 10 V and a pulse width of 1 ms. Above induction protocol was repeated again under isoproterenol infusion of 5µg/min.
When a stable mappable AT was induced, an activation map using the electroanatomical mapping system was created to delineate the AT circuit. Entrainment studies were also performed for the macro-reentrant AT to confirm the reentrant circuit. An ablation targeting the earliest activation site for centrifugal AT or a linear ablation interrupting the reentrant circuit for macro-reentrant AT was performed.
If unmappable ATs were encountered, the operator initially tried to ablate the unmappable ATs based on the undetermined AT circuits estimated using conventional methods such as activation timings of placed catheter electrodes, the responses to entrainment pacing, and/or the distribution of diastolic potentials, defined as an fractionated signals covering the missing time zone of simple large signals recorded on other electrodes during AT. If an induced AT was successfully eliminated by conventional ablation, the induction protocol was repeated again until no atrial tachyarrhythmias other than AF was induced.
If the induction resulted in AF lasting for > 1 minute, electrical cardioversion was delivered to restore sinus rhythm and the next induction was delayed for a period of time greater than twice the duration of the last induced AF episode to ensure recovery of the AF-induced shortening of the myocardial refractory period to baseline values.8
LA LVA ablation was performed at the discretion of the attending operators based on the presence of an LVA, patient condition, time spent on the PVI and other ablations, and clinical course (symptoms, frequency) of the arrhythmias.
LA LVAs were regionally ablated with the power set at 30W, and the ablation catheter was moved point by point in a dragging fashion via a long sheath (Figure 1 and Figure 2). The endpoint at each ablation site was defined as an electrogram voltage reduction of > 50% during sinus rhythm.5 The LA posterior LVA was sometimes isolated by PVI, roof, and bottom lines. Both entrance and exit blocks between the posterior wall and other LA were confirmed.
Figure 2. A representative case with residual LVAs after LVA ablation.
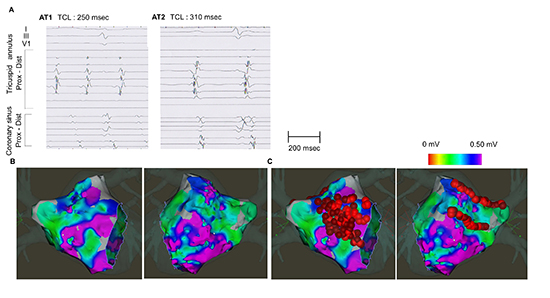
A case (#9 in Table 2) with 2 unmappable ATs after pulmonary vein isolation (A). LVAs were distributed in the septal, anterior, roof, and posterior regions (B). Conventional ablation failed to eliminate some unmappable ATs. LA LVA ablation failed to complete voltage homogenization (C). Ablation at anterior, septal, and inferior regions were aborted to avoid conduction delay at Bachman’s bundle, atrioventricular block, and esophageal injury. However, unmappable ATs were no longer inducible after the LVA ablation. AT, atrial tachycardia; LVA, low-voltage area; LA, left atrial
Patients were followed up every 4–8 weeks at the dedicated arrhythmia clinic of our institution for a minimum of 1 year. Routine ECGs were obtained at each outpatient visit, and 24-h ambulatory Holter monitoring was performed 6 and 12 months post-ablation. When patients experienced symptoms suggestive of an arrhythmia, a surface ECG, ambulatory ECG, and/or cardiac event recording were also obtained. Either of the following events after the initial 3 months from the ablation (blanking period) was considered to indicate atrial tachyarrhythmia (AF and regular atrial tachycardia) recurrence: (1) atrial tachyarrhythmia recorded on a routine or symptom-triggered ECG during an outpatient visit, or (2) atrial tachyarrhythmia of at least 30 s duration on ambulatory ECG monitoring. No antiarrhythmic drugs were prescribed after the ablation procedure unless recurrent atrial tachyarrhythmia was observed.
Continuous data are expressed as the mean ± standard deviation or median (interquartile range). Categorical data are presented as absolute values and percentages. Tests for significance were conducted using the unpaired t-test, or nonparametric test (Mann-Whiney U-test) for continuous variables, and the chi-squared test or Fisher’s exact test for categorical variables. All analyses were performed using commercial software (SPSS version 22.0®, SPSS, Inc., Chicago IL, USA).
Among 911 AF ablation procedures during the study period, unmappable ATs developed in 32 cases. Patient characteristics are shown in [Table 1]. Of 17 (53%) patients undergoing repeat ablation, the ablation of lesions in addition to PVI created at the previous ablation included 4 LA roof lines, 3 LA bottom lines, 2 mitral isthmus lines, and 7 cavo-tricuspid isthmus lines for induced macro-reentrant ATs, and 1 isolation of superior vena cava (SVC) and 1 focal ablation at the anterior LA for a non-PV AF trigger.
Table 1. Patient characteristics
| Age, years |
72 ± 8 |
| Female, n (%) |
17 (53) |
| Body mass index, kg/m2 |
23.1 ± 3.7 |
| AF type, n (%) |
|
| Paroxysmal |
14 (44) |
| Persistent (< 1 year) |
17 (53) |
| Long-standing persistent |
1 (3) |
| AF duration, months |
14 (5, 22) |
| Hypertension, n (%) |
13 (41) |
| Diabetes mellitus, n (%) |
6 (19) |
| Heart failure, n (%) |
9 (28) |
| CHA2DS2-VASc score |
3.0 ± 1.5 |
| LA diameter, mm |
44 ± 8 |
| Use of Rhythmia®, n (%) |
4 (12) |
| Repeated ablation, n (%) |
17 (53) |
| 2nd session |
14 (44) |
| > 2 sessions |
3 (9) |
In the ablation procedure, de novo PVI or repeat PVI were performed in all patients. After the completion of PVI, a voltage map was created during sinus rhythm in 26 patients, and during atrial tachyarrhythmias in 6 patients. The number of mapping points were 133 (106, 170) using the Carto3® with the ablation catheter (n = 19), 1028 (872, 1129) with the circulation catheter (n = 9), and 7588 (6718, 9220) using the Rhythmia® with the mini-basket catheter (n = 4). LVAs existed in 31 (97%) patients with an area of 19 ± 12 cm2, occupying 16% ± 12% of the LA surface area.
Ablation for mappable ATs
Twenty-eight mappable ATs developed in 21 patients spontaneously and/or by pacing induction before and during the LVA ablation procedure, except for those developing after LVA ablation. Identified mappable AT circuits consisted of 15 macro-reentrant type (6 peri-mitral, 3 LA roof dependent, 1 RA lateral wall, 5 peri-tricuspid ATs), and 13 focal type (1 LA anterior, 4 LA septal, 1 LA posterior wall, 3 LA appendage, 1 RA appendage, 1 SVC, 1 coronary sinus ostium, and 1 lateral tricuspid annulus). Catheter ablation successfully eliminated all the mappable ATs.
Conventional ablation of unmappable ATs
During the ablation procedure, 117 unmappable ATs developed spontaneously and/or by pacing induction. Unmappable ATs were sustained for 58 (19, 161) s with a cycle length of 270 (230, 320) ms. Conventional ablation targeting the estimated AT circuits resulted in the complete elimination of ummappable ATs in 3 (9%) cases Figure 3. Detailed ablation sites were: LA roof line in 4 patients, LA bottom line in 3, septal mitral line in 1, posterior mitral line in 1, cavo-tricuspid isthmus line in 4, isolation of SVC in 1, and diastolic potential during AT in 2.
Figure 3. Patient flow chart
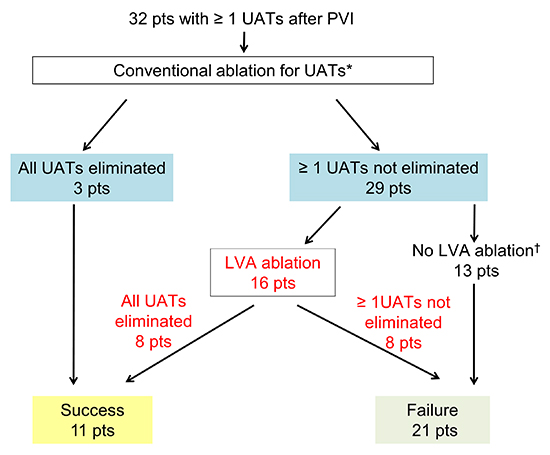
Conventional ablation targeting the undetermined AT circuits estimated from activation timings of electrograms recorded on the placed electrode catheter, the response to entrainment mappings, and/or diastolic potentials during AT, was performed. After that, LVA ablation was performed at the discretion of the operators. *Conventional ablation included LA roof line in 4 patients, LA bottom line in 3, septal mitral line in 1, posterior mitral line in 1, cavo-tricuspid isthmus line in 4, isolation of SVC in 1, and diastolic potential during AT in 2. †The reasons for not performing LVA ablation were as follows: LVA was not observed in 1 patient and 12 patients were too exhausted to endure an additional LVA ablation after the time-consuming conventional ablation procedure.
Among the 29 (91%) cases with residual unmappable ATs following conventional ablation, 16 underwent LVA ablation. LVA ablation was not performed in the remaining 13 patients for the following reasons: LVA was not observed in the LA in 1 patient, and the operator assessed that the patient could not endure the additional LVA ablation due to the exhaustion from the time consuming procedures before LVA ablation (12 patients). Among the patients with residual unmappable ATs following a conventional ablation, the number of unmappable ATs were comparable between the patients with and without an LVA ablation (3.3 ± 2.4 vs. 4.0 ± 2.2, p = 0.38).
Electrophysiological details of each patient undergoing LVA ablation are shown in Table 2. LVA was observed at the anterior and/or septal regions in most patients, followed by roof and posterior regions with an area of 19 ± 11 cm2 occupying 15% ± 11% of the LA surface area.
Table 2. Substrate and atrial tachyarrhythmias in each patient with LVA ablation
| No |
Before LVA ablation |
After LVA ablation |
|
Already-ablated lesions |
LVA |
UAT |
Residual LVA |
|
LA |
RA |
Region |
Area, cm2 |
No |
|
CLs*, ms |
Region |
Area,cm |
| 1 |
Rf, Btm, |
CTI |
Post |
11 |
10 |
|
170-380 |
- |
- |
| 2 |
Spt, Rf |
- |
Spt |
10 |
1 |
|
220-220 |
- |
- |
| 3 |
Spt |
Spt |
Spt, Ant |
25 |
2 |
|
230-230 |
- |
- |
| 4 |
Lat |
CSo, TA, SVC |
Spt |
13 |
3 |
|
220-270 |
- |
- |
| 5 |
Rf, Btm |
- |
Spt, Ant |
10 |
5 |
|
210-380 |
- |
- |
| 6 |
App |
- |
Ant |
6 |
2 |
|
300-320 |
- |
- |
| 7 |
- |
CTI |
Ant, Rf |
7 |
6 |
|
250-320 |
- |
- |
| 8 |
Spt, Rf, App |
- |
Spt, Ant, Lat |
13 |
1 |
|
230-230 |
Spt, Ant |
5 |
| 9 |
Ant |
- |
Spt, Ant, Rf, Post, Inf |
32 |
2 |
|
250-310 |
Spt, Ant, Inf |
9 |
| 10 |
Spt |
- |
Spt, Ant, Inf |
33 |
2 |
|
270-280 |
- |
- |
| 11 |
- |
- |
Spt, Ant, Rf |
5 |
1 |
|
220-220 |
- |
- |
| 12 |
Ant |
- |
Spt, Ant, Rf, Inf |
30 |
2 |
|
330-360 |
Ant, Rf, |
16 |
| 13 |
- |
CTI, SVC, App |
Spt, Ant, Post |
24 |
5 |
|
230-340 |
- |
- |
| 14 |
Rf, Btm |
- |
Spt, Ant, Rf, Lat |
35 |
2 |
|
310-750 |
Spt, Ant |
12 |
| 15 |
- |
CTI |
Spt, Post |
15 |
4 |
|
220-310 |
- |
- |
| 16 |
Spt, Ant, App |
- |
Spt, Ant, Post, Rf |
36 |
4 |
|
270-390 |
- |
- |
*Minimum - maximum cycle lengths are shown. †The mappable AT had a bi-atrial reentrant circuit and was successfully eliminated by focal ablation at the RA-LA connection. LVA indicates low-voltage area; No, number; UAT, unmappable atrial tachycardia; LA, left atrium; RA, right atrium; CLs, cycle lengths; Rf, roof; Btm, bottom; Spt, septal; Lat, lateral; App, appendage; Ant, anterior; CTI, cavo-tricuspid isthmus; CSo, coronary sinus ostium; TA, tricuspid annulus, SVC; superior vena cava; Post, posterior; Inf, inferior; AF, atrial fibrillation; MAT, mappable AT.
LVA ablation was performed with a mean radiofrequency application time of 9.6 (4.6, 19.6) min. Voltage homogenization in all LVAs was achieved in 12 (75%) patients. In the remaining 4 patients, ablation at anterior, septal, roof, and/or inferior regions were performed to an extent not causing conduction delay at Bachman’s bundle, atrioventricular block, or esophageal injury.
AT/AF inducibility after LVA ablation
Atrial burst pacing after LVA ablation induced unmappable ATs in 8 (50%) patients [Table 2]. The distribution of the patients undergoing repeat ablation procedures (63% vs. 50%, p = 1.0) and those with a paroxysmal type of AF (63% vs. 50%, p = 1.0) did not differ between the patients with and without AT/AF inducibility after the LVA ablation. Comparisons of electrophysiological characteristics between patients with and without AT/AF inducibility after LVA ablation are shown in Table 3. The LVA size and the ratio of complete voltage homogenization did not differ between patients with and without successful elimination of unmappable ATs. A stable and mappable AT was induced after LVA ablation in one patient (Table 2, case No. 14). The AT had a bi-atrial reentrant circuit and was successfully eliminated by focal ablation at the RA-LA connection.
Table 3. Comparisons of electrophysiological and anatomical properties between patients with and without successful elimination of unmappable AT(s) by LVA ablation
|
Elimination of unmappable ATs by LVA ablation |
|
|
Successful |
failed |
|
|
n = 8 |
n = 8 |
P |
| Number of unmappable ATs |
2.9 ± 2.9 |
3.6 ± 1.8 |
0.55 |
| LA diameter, mm |
44 ± 8 |
46 ± 10 |
0.87 |
| Estimated AT origin |
|
|
|
| Left atrium only |
8 (100) |
6 (75) |
0.32 |
| Both left and right atria |
|
1 (13) |
|
| Unknown |
|
1 (13) |
|
| Shortest cycle length, ms |
244 ± 50 |
248 ± 34 |
0.80 |
| Longest cycle length, ms |
290 ± 62 |
374 ± 161 |
0.24 |
| LA area, cm2 |
141 ± 21 |
141 ± 14 |
0.98 |
| LVA, cm2 |
17 ± 11 |
21 ± 12 |
0.59 |
| Proportion of LVA in relation to LA surface, (%) |
13 ± 8 |
18 ± 13 |
0.29 |
| Complete voltage homogenization |
7 (88) |
4 (50) |
0.08 |
| AF inducibility after LVA ablation |
0 (0) |
3 (38) |
0.62 |
| Recurrence during follow-up period |
|
|
|
| AT |
1 (13) |
4 (50) |
0.28 |
| AT and/or AF |
3 (38) |
5 (63) |
0.62 |
During a mean follow-up period of 14 ± 8 months, AT/AF recurrence was observed in 20 patients (63%). There was no difference in recurrence rates between patients with and without residual unmappable ATs after the conventional ablation (62% vs. 67%, p = 1.00). The numbers of induced unmappable ATs were comparable between the patients with and without an AT/AF recurrence (3.6 ± 2.0 vs. 3.9 vs. 2.6, p = 0.66). Further, among 29 patients with residual unmappable ATs after conventional ablation, the recurrence rates were 50% and 75% in patients with and without additional LVA ablation, respectively. (p = 0.25). In addition, among 16 patients with LVA ablation, no statistical difference in AT/AF recurrence rates was observed between patients with and without successful elimination of unmappable AT Table 3.
This observational study included 32 consecutive patients who underwent AF ablation and developed unmappable ATs. Of 29 patients in whom conventional ablation failed to eliminate at least one unmappable ATs, 16 patients underwent LVA ablation. LVA ablation successfully eliminated the inducibility of unmappable ATs in 8 of 16 patients. However, the small sample size inhibited investigation of the influence of LVA ablation on long-term outcomes. To our knowledge, this is the first clinical study describing the efficacy of LVA ablation on the elimination of unmappable ATs refractory to conventional ablation.
LVA as an arrhythmogenic substrate for AT
.
Several histological and clinical studies support the hypothesis that LVAs may act as arrhythmogenic substrates of AT. LVAs on the atrial voltage map have been reported to correlate with regions of scarring detected by delayed enhancement on magnetic resonance imaging.9, 10 Fibrotic scar tissue and surrounding diseased myocardium might form an arrhythmogenic substrate by predisposing to reentry, which plays an important role in the maintenance of atrial tachyarrhythmias.11, 12 A prior clinical study demonstrated slow conduction of propagation wave fronts at LVAs.13 We recently reported that macro-reentrant ATs following PVI were likely to have LVAs on their reentrant circuits.6 More directly, a detailed analysis of scar-related AT using an ultra-high-resolution mapping system revealed that the slow-conduction isthmus of macro-reentrant AT had a much lower voltage than the surrounding area.14 It has also been reported that that the connection between fibroblasts and myocytes shortens the action potential duration, possibly resulting in the development of triggered activity at the LVA.15
Substrate ablation targeting LVA for unmappable ATs
The present study showed that LVA ablation successfully eliminated unmappable ATs in half of patients. The underlying concept of the substrate-based approach targeting LVAs is to ablate the critical slow-conduction channels and some foci of ectopic activity, which might contribute to the development and maintenance of unmappable ATs. Although the conventional ablation strategy identifying the AT circuit using a 3-dimensional electroanatomical mapping system in conjunction with electrophysiological maneuvers, including an entrainment study, is the optimal approach to the ablation of an AT, it works as far as the AT is stable enough to draw a map and/or perform entrainment pacing. LVA ablation is a substrate ablation strategy that may enable operators to ablate some unmappable ATs refractory to conventional ablation.
A substantial proportion of unmappable ATs were not eliminated by LVA ablation. There are probably several reasons. Macro-reentrant ATs propagating around large anatomical obstacles like the tricuspid or mitral annuli can occur without any obvious slow-conduction area on the circuit. ATs with abnormal automaticity and triggered activity would not necessarily depend on the existence of significant amounts of fibrotic tissue. Voltage mapping and ablation were performed only in the left atrium, which might have missed arrhythmogenic substrates in the RA, coronary sinus, and other epicardial structures. The radiofrequency application at LVAs was continued until a significant reduction of voltage on an ablation catheter was observed. However, this endpoint may allow some residual viable myocardium to act as an arrhythmogenic substrate, because tiny signals would be obscured using the large electrodes of ablation catheters.16
LVA ablation in addition to PVI has been reported to be effective to improve the rhythm outcomes in AF patients.3 In addition, successful elimination of AT that develops during AF ablation procedures could be associated with a reduced long-term AT/AF recurrence rate. However, in the present study, the long-term AT/AF recurrence rates did not differ between the patients with and without an LVA ablation for unmappable ATs, nor between those with and without a successful elimination of unmappable ATs after the LVA ablation. The sample size was too small to appropriately explore the long-term rhythm outcomes that would be influenced not only by the ablation procedures, but also by the baseline characteristics, post ablation patient management, and recurrent-AT/AF monitoring methods during the follow-up period. DECAAF II, an ongoing randomized controlled trial will clarify the long-term effect of the ablation targeting fibrotic tissue.
Several limitations of this study warrant mention. First, the heterogeneous patient background made the implication of the study results difficult. Second, as we conducted voltage mapping after creating PVI and some other ablation lesions, LVAs near pre-ablation lesions could not be determined precisely. Third, the voltage map was created using more than one kind of catheter, different mapping systems, and under both sinus rhythm and AT, such that a single criterion for LVAs may not always identify arrhythmogenic substrate consistently. Especially, it was reported that LVA measurement is broader when using ablation catheter than multielectrode catheter.17 Fourth, the impact of conventional ablation before LVA ablation is operator-dependent, and this would influence the efficacy of LVA ablation. Fifth, AF recurrences after discharge were identified on the basis of the patients’ symptoms, giving rise to the possibility that asymptomatic episodes of AF might have been missed. Finally, the small sample size limits the statistical accuracy, especially analyses of long-term outcomes.
LVA ablation was efficacious to some extent for the acute elimination of unmappable ATs developing in patients undergoing AF ablation, and could be an alternative to the conventional approach identifying each AT circuit. Larger studies are warranted.






