The overall response rate of Delphi first round was 100% (62 responding participants out of 62 total panelists) and that of second round was 100% (62 out of 62).
Of the total of 65 items, 37 reached a positive consensus (agreement), 14 reached a negative consensus (disagreement) and 14 did not reach a consensus. The group of experts therefore decided to undergo a second vote. In particular, the statements 7, 9, 10 (items 10.4 to 10.8) and 13 were revised. Among these, only point 7.2 reached a different consensus than the first vote. For narrative reasons the topics have been organized and discussed in 7 scenarios.
Scenario 1. DOACs versus VKAs (topics 1, 2 and 4)
Participants expressed agreement on the superiority of DOACs compared VKAs both in terms of efficacy (87%) and efficacy and safety (92%) ([Table 1], statements 1.1, 1.2). Clear disagreement on statement 1.3 (84%), showed that according to the experts’ opinion, effectiveness of DOACs does not compromise the safety ([Table 1], statement 1.3). The consensus on superiority in terms of safety alone was more articulated and less compact ([Table 1], statement 1.4), thus emphasizing the importance of the "net clinical benefit" while assessing impact of DOACs. On the other hand, consensus on the greater handling of the DOACs compared to the VKAs was almost unanimous (97%) ([Table 1], statement 1.5).
Table 1. Statement 1: DOACs are superior to VKAs
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 1.1 In terms of efficacy |
2 |
6 |
14 |
17 |
23 |
62 |
|
13% |
87% |
100% |
| 1.2 In terms of efficacy and safety |
1 |
4 |
6 |
14 |
37 |
62 |
|
8% |
92% |
100% |
| 1.3 In terms of efficacy but not safety |
26 |
26 |
5 |
3 |
2 |
62 |
|
84% |
16% |
100% |
| 1.4 In terms of safety but not efficacy |
17 |
15 |
9 |
17 |
4 |
62 |
|
52% |
48% |
100% |
| 1.5 In terms of handling |
1 |
1 |
3 |
10 |
47 |
62 |
|
3% |
97% |
100% |
Participants expressed maximum agreement to consider DOACs as the first choice compared to VKAs, not only in patients with high thromboembolic or hemorrhagic risks, but in all patients. This position is also in line with the latest European guidelines on AF [4] ([Table 2], item 2.1).
Table 2. Statement 2: DOACs are the first-choice option for treatment of NVAF
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 2.1 In all patients with no contraindications |
0 |
0 |
3 |
10 |
49 |
62 |
|
0% |
100% |
100% |
| 2.2 Only in patients with high hemorrhagic risk |
21 |
23 |
8 |
6 |
4 |
62 |
|
71% |
29% |
100% |
| 2.3 Only in patients with high thromboembolic risk |
23 |
25 |
5 |
6 |
3 |
62 |
|
77% |
23% |
100% |
| 2.4 Never |
53 |
9 |
0 |
0 |
0 |
62 |
|
100% |
0% |
100% |
Appropriateness of the switch from AVKs to DOACs obtained the maximum consensus in cases of failure to INR (International Normalized Ratio) control or in any case of practical difficulty in performing close sampling ([Table 3], items 4.1-4.2). In case of INR stability (i.e., adequate time in therapeutic range, TTR) there was no consensus to switch. As well as no consensus was reached on indiscriminate switch to DOACs for all patients treated with AVKs who have no contraindications to treatment with DOACs themselves ([table 4], items 4.3-4.4).
Table 3. Statement 4: The switch from VKAs to DOACs is appropriate
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 4.1 In not-controlled patients via AVKs |
0 |
0 |
0 |
8 |
54 |
62 |
|
0% |
100% |
100% |
| 4.2 In well controlled patients with difficulty in monitoring the INR and adhering to the therapy |
0 |
0 |
3 |
12 |
47 |
62 |
|
0% |
100% |
100% |
| 4.3 Never if patient is stable while on AVK therapy |
5 |
29 |
19 |
9 |
0 |
62 |
|
55% |
45% |
100% |
| 4.4 Always in the absence of contraindications |
5 |
22 |
13 |
9 |
13 |
62 |
|
44% |
56% |
100% |
A meta-analysis of the results of four pivotal trials for the use of DOACs in patients with NVAF was performed to evaluate ischemic and hemorrhagic stroke, systemic embolism, all-cause mortality, myocardial infarction and major bleeding events [5]-[8]. The results showed that DOACs significantly reduced systemic stroke/embolism events by 19% compared to warfarin (RRR 0.81, 95% CI 0.73-0.91; p <0.0001), markedly reduced the hemorrhagic stroke (RRR 0.49, 95% CI 0.8-0.64; p <0.0001) and significantly reduced all-cause mortality (RRR 0.90, 95% CI 0.85-0.95; p = 0.0003) [9].
Similar meta-analyses performed by Renda et al. [10],[11], evaluating the net clinical benefit by a cumulative examination of endpoints analysis, demonstrated the clear superiority of DOACs compared to warfarin in terms of the composite endpoint of disabling stroke and life-threatening bleeding. On the contrary, compared to warfarin, only dabigatran and apixaban showed a significant reduction in the disabling stroke and life-threatening bleeding composite endpoint. Moreover, only edoxaban (at both recommended doses) was superior to warfarin in the cumulative evaluation of ischemic/hemorrhagic stroke/acute myocardial infarction/systemic embolism and major bleeding [12].
Regarding the safety endpoint of DOACs compared to warfarin, in addition to the strong reduction in brain hemorrhage of 50% in all studies, the sub-analysis of the ENGAGE AF-TIMI 48 study demonstrated a significant reduction in fatal bleeding at both recommended doses of edoxaban, compared to warfarin [6].
In parallel, a meta-analysis of randomized clinical studies reported that DOACs significantly reduced major bleeding compared to warfarin, when the TTR was <66% (p <0.02), even if intestinal bleeding was slightly increased (RR 1.25, p = 0.04) [13].
Several real-world studies support the importance of examining the net clinical benefit in the elderly before establishing a therapy because the risk of thromboembolic and hemorrhagic events in patients with AF increases with age. In this regard, some researchers aimed at comparing DOACs with VKAs in terms of the 1-year clinical outcome in elderly (≥75 years) patients with AF enrolled in a prospective European Registry. The data obtained in 3,852 elderly patients were assembled by the PREFER in AF registry [14] and in AF-PROLONGATION (the data of this registry are still unpublished). The primary outcome was the incidence of the composite endpoint, including major hemorrhagic and ischemic events, during the treatment with DOACs (N = 1,556) compared to VKAs (N = 2,269). The percentage of the composite endpoint was 6.6%/year with DOACs versus 9.1%/year with VKAs (adjusted OR 0.64, 95% CI 0.48-0.86, p = 0.003). The treatment with a DOAC was associated with a lower bleeding rate compared to VKA treatment (adjusted OR 0.52, 95% CI 0.33-0.83, p = 0.006). Moreover, the number of ischemic events was lower (OR adjusted 0.71, 95% CI 0.50-0.99, p = 0.048). The difference in major bleeding associated with DOACs compared to patients treated with VKAs was even greater in elderly patients with low body mass index (BMI, adjusted OR 0.40), and in patients aged ≥85 (adjusted OR 0.33) [14].
Participants of this consensus expressed agreement on the superiority of DOACs compared VKAs both in terms of efficacy, safety and handling. Consequently, DOACs can be considered as first-choice option for thromboprophylaxis in patients with NVAF and no contraindications to them.
Scenario 2. DOACs use in patients undergoing ECV (topic 3)
The panel agreed in considering DOACs as first therapeutic choice also in the setting of patients undergoing ECV [Table 4], according to the results of recent trials and based on greater safety, manageability and quick action compared to VKAs [15]-[17].
Table 4. Statement 3 on the use of DOACs in patients undergoing ECV
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 3.1 DOACs are always the first-choice therapy |
1 |
5 |
8 |
16 |
32 |
62 |
|
10% |
90% |
100% |
| 3.1 DOACs are a valid alternative to VKAs |
3 |
2 |
14 |
19 |
24 |
62 |
|
8% |
92% |
100% |
| 3.3 VKAs are the first-choice therapy |
24 |
32 |
4 |
2 |
0 |
62 |
|
90% |
10% |
100% |
| 3.4 DOACs should not be used |
56 |
5 |
0 |
1 |
0 |
62 |
|
98% |
2% |
100% |
ECV is a valid alternative for restoring sinus rhythm in patients with AF [18]. The need for anticoagulation for the prevention of thrombotic events in patients with AF undergoing ECV is entirely empirical, even if it was further validated by studies using transesophageal echocardiography (TEE) in the 1990s [18].
The current mainstay is the use of a VKA for at least 3 weeks prior to ECV and for the following 4 weeks. Furthermore, the patient should have INR values in the range of 2.0- 3.0 in the 3 weeks before the procedure. The duration of anticoagulant therapy preceding ECV may be less than three weeks, if ECV is anticipated by a negative TEE. This approach results in thromboembolic rates lower than 1% within 30 days [19].
Since the marketing of DOACs, the scenario of the prevention of thromboembolism in the AF has changed. This certainly also extends to the subgroup of patients who are candidates for ECV [19]. During the pivotal studies, efficacy and safety were demonstrated for all DOACs, even in patients who underwent ECV during the anticoagulant treatment. Prospective studies focused on patients undergoing ECV have also validated the possibility of using the DOACs in this setting, both for the classic anticoagulation (late ECV) scheme for 3 weeks before and 4 weeks after ECV, and for early ECV (TEE-guided).
Subgroup analyses followed the publication of the results of the related main studies (RE-LY, ROCKET AF, ARISTOTLE and ENGAGE AF-TMI 48) [5]-[8]. The largest sub-analysis is that of the RE-LY study regarding 1,983 ECV in 1,270 patients (647, 672, and 664 patients respectively in each of the dabigatran 110 mg, dabigatran 150 mg, and warfarin arms) [20]. TEE was performed in about 25% of the dabigatran groups versus 13.3% in the warfarin group. No difference was observed for the incidence of spontaneous left atrial echo contrast or auricular thrombus (ranging from 1.1% with warfarin to 1.8% with dabigatran 110 mg). The main results of an intention-to-treat analysis showed a low rate of events (<1%) 30 days after ECV and no statistical difference was found among the three groups [20].
In a post-hoc analysis of the ARISTOTLE study on apixaban and ECV, 743 ECVs were performed in 540 patients [21], 265 ECVs in patients allocated to the apixaban arm, and 275 in patients assigned to warfarin. In the 30-day follow-up period no ischemic stroke or systemic embolism occurred in either groups. Major bleeding occurred in 1 patient (0.2%) treated with warfarin and in 1 patient treated with apixaban (0.3%). TEE was performed in 171 patients (203 ECVs): 86 patients (97 ECVs) assigned to the apixaban arm, and 85 patients (106 ECVs) assigned to the warfarin arm. In none of the patients a left atrial thrombus occurred, while 4 patients (1 for apixaban and 3 for warfarin) had evidence of spontaneous echo contrast. For apixaban, the EMANATE trial in 1,038 patients undergoing ECV and 300 spontaneous cardioversions showed that there were 0/753 vs. 6/747 strokes [relative risk (RR) 0; 95% confidence interval (95% CI) 0-0.64; nominal P = 0.015], no systemic embolism, and 2 vs. 1 deaths (RR 1.98; 95% CI 0.19-54.00; nominal P > 0.999). Moreover, there were 3/735 vs. 6/721 major (RR 0.49; 95% CI 0.10-2.07; nominal P = 0.338) and 11 vs. 13 clinically relevant non-major bleeding events (RR 0.83; 95% CI 0.34-1.89; nominal P = 0.685). In summary, rates of stroke, embolic events, deaths and bleedings were low for both apixaban and heparin/VKA in patients with AF undergoing cardioversion [17],[21].
Two studies examined rivaroxaban in this context. In the post-hoc analysis of the ROCKET AF study [22] in 14,264 patients only 143 patients underwent 181 electrical ECVs. This number was small because, according to the protocol, the patients for whom an ECV was planned, were excluded from the trial. Because of this small number, the patients undergoing ECV, pharmacological cardioversion, and transcatheter ablation were analyzed together. There were 2 thromboembolic events in the rivaroxaban group (1.64%) and 3 in the warfarin group (2.48%).
Rivaroxaban was compared to warfarin in the prospective randomized X-VeRT study specifically focused on ECV [15], where 1,504 patients with hemodynamically stable NVAF were randomized in a 2:1 ratio to receive rivaroxaban once daily (20 mg/day, or 15 mg/day in patients with creatinine clearance [CrCl] 30-49 ml/min), or VKAs. Patients were also randomized to either early strategy or delayed strategy for ECV. For early ECV, rivaroxaban or VKA were administered for a period of 1-5 days prior to ECV, and for 6 weeks after the procedure. For late ECV, patients received rivaroxaban or a VKA for 3-8 weeks before ECV and for further 6 weeks. Interestingly, among patients assigned to late ECV, 77% of the rivaroxaban group and only 36.3% of the VKA group underwent ECV within the expected period (p <0.001). The main reason for postponing the procedure in the patients treated with VKAs was the failure to achieve adequate anticoagulation with weekly INRs within the range 2.0-3.0. The primary efficacy outcome was the composite of stroke, transient ischaemic attack, peripheral embolism, myocardial infarction, and cardiovascular death. The primary efficacy outcome occurred in 5 (two strokes) of 978 patients (0.51%) in the rivaroxaban group and in 5 (two strokes) of 492 patients (1.02%) in the VKA group [risk ratio 0.50; 95% confidence interval (CI) 0.15-1.73]. The primary safety outcome was major bleeding. Major bleeding occurred in 6 patients (0.6%) in the rivaroxaban group and 4 patients (0.8%) in the VKA group (risk ratio 0.76; 95% CI 0.21-2.67) [15]. Consequently, rivaroxaban can be considered an effective and safe alternative to VKAs.
The post-hoc analysis of the ENGAGE AF-TIMI 48 trial regarded a total of 632 ECV attempts performed while on study drug in 365 patients [23]. In the 30 days after ECV, stroke or systemic embolism occurred in 2 patients on the lower-dose edoxaban regimen; none occurred with warfarin or higher-dose edoxaban. There were no major bleeding events and 1 death (higher-dose edoxaban) in the same timespan. Consequently, thromboembolic and major bleeding events post ECV were infrequent and similar with edoxaban and warfarin in the ENGAGE AF-TIMI 48 trial [23]. The ENSURE-AF study is the largest randomized clinical trial comparing a DOAC agent and VKAs in patients with NVAF undergoing ECV [16]. The study enrolled 2,199 patients and compared in a 1:1 fashion edoxaban mono-therapy daily with the enoxaparin/warfarin treatment with a mean TTR (INR 2.0-3.0) of 70.8%. The primary efficacy endpoint was a composite of stroke, systemic embolic event, myocardial infarction, and cardiovascular mortality, analysed by intention to treat. It occurred in 5 (<1%) patients in the edoxaban group versus 11 (1%) in the enoxaparin-warfarin group (odds ratio [OR] 0.46, 95% CI 0.12-1.43). The primary safety endpoint was major and clinically relevant non-major bleeding. It occurred in 16 (1%) of patients given edoxaban versus 11 (1%) of patients given enoxaparin-warfarin (OR 1.48, 95% CI 0.64-3.55). The results were independent of the TEE-guided strategy and anticoagulation status. Edoxaban was shown as a valid alternative to warfarin in subjects undergoing both TEE-guided ECV or late ECV [16].
The results of this consensus were totally convergent in deeming the treatment with DOACs as first choice compared to VKAs also in patients who undergo ECV.
Role of GPs and TAO centers (topics 5, 6 and 7)
According to the expert panel, GPs should manage the follow-up and the intermediate controls, monitoring renal function and blood count. Moreover, GPs could indicate temporary suspension of anticoagulation therapy prior to invasive diagnostics and interventions, as well in case of minor bleeding ([Table 5], items 5.1-5.2). This scenario is also suggested by the European Heart Rhythm Association (EHRA) Practical Guide for the use of anticoagulants in patients with AF [24]. There was no consensus on the exclusive role of GPs in control and management of any adverse events, which should - at least in selected cases - be prerogative of the specialist (namely, Centro Prescrittore in Italy) ([Table 5], item 5.3). The consensus was broad on the involvement of GPs in the management of patients treated with DOACs ([Table 5], item 5.4). However, the panel highlighted operative issues as the number of therapeutic plans with DOACs is constantly increasing (e.g., in Lazio Region, about 3,000 new therapeutic plans/month are recorded). In this setting, service providing for the subsequent year is overflowing. A further problem raised by the panel is related to patients who do not have the clinical documentation suitable for follow-up visits (echocardiogram and updated biochemical tests).
Table 5. Statements 5 on GPs role in the management of patients treated with DOACs
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 5.1 Manage follow-up and intermediate controls |
2 |
3 |
20 |
18 |
19 |
62 |
|
8% |
92% |
100% |
| 5.2 Manage temporary suspension of anticoagulation therapy prior to invasive diagnostics and interventions, as well as in case of minor bleeding |
6 |
10 |
18 |
17 |
11 |
62 |
|
26% |
74% |
100% |
| 5.3 Manage potential adverse events |
7 |
17 |
15 |
14 |
9 |
62 |
|
39% |
61% |
100% |
| 5.4 Not to be involved in the management of patients treated with DOACs |
36 |
18 |
5 |
2 |
1 |
62 |
|
87% |
13% |
100% |
Consensus was reached on the control and management of adverse events, as well as renewal of therapeutic plan and start of therapy with DOACs, performed by TAO centers ([Table 6], items 6.1-6.5).
Table 6. Statements 6 on the role of TAO centers
TAO centers should continue managing patients for whom AVKs is the only therapeutic option. Namely: carriers of mechanical valve prostheses, patients with moderate-severe rheumatic mitral stenosis, patients with diseases affecting the factors of coagulation (e.g., anti-phospholipid antibodies) and patients with stable INR not switched to treatment with DOACs.
The panel evaluated the possibility of converting TAO centers into DOAC centers, for i) better management of the switch from AVKs to DOACs, ii) therapy with DOACs in naïve patients, iii) managing follow-up visits and renewals of therapeutic plans and iv) the management of side effects. However, this scenario would perpetrate some territorial disparities due to lack of equality of the distribution of TAO centers in the Country and within Regions.
Clinicians (such as cardiologists, internists, neurologists) could manage prescription of DOACs in naïve patients and switch from treatment with AVKs to DOACs in patients with low TTR.
No consensus was reached on the hypothesis that the GPs can replace TAO/DOAC centers neither in prescription and management of DOAC-based therapy nor in the renewal of the therapeutic plan ([Table 7], statements 7.1 and 7.2). Although GPs should not prescribe DOACs in naïve patients ([Table 7], statement 7.4), they should be involved in the monitoring of patients treated with DOACs ([Table 7], statement 7.5), being in charge of the management of DOACs minor side effects ([Figure 7], statement 7.3).
Table 7. Statements 7 on GPs role in the management of therapy with DOACs
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 7.1 GPs can replace TAO centres and/or specialists in prescribing therapy and managing follow-up visits for patients treated with DOAs |
11 |
17 |
15 |
9 |
10 |
62 |
|
45% |
55% |
100% |
| 7.2 GPs can replace TAO centres and/or specialists in renewing therapeutic plans with DOACs |
18 |
16 |
7 |
10 |
11 |
62 |
|
55% |
45% |
100% |
| 7.3 GPs can manage minor side effects of therapy with DOACs |
1 |
5 |
19 |
28 |
9 |
62 |
|
10% |
90% |
100% |
| 7.4 GPs can prescribe DOACs in native patients |
27 |
23 |
8 |
3 |
1 |
62 |
|
81% |
19% |
100% |
| 7.5 GPs should not be involved in the monitoring of patients treated with DOACs |
38 |
14 |
7 |
1 |
2 |
62 |
|
84% |
16% |
100% |
Regarding the involvement of the GPs, the panel expressed a negative consensus on the possibility that the GPs will carry out the first prescription of a DOAC or renew the treatment plan when expired. It was agreed instead that the GPs shall manage the follow-up and the intermediate controls in patients treated with DOACs. This position is also suggested by a European consensus document [24].
Nevertheless, according to the expert panel, the TAO centers will continue managing patients who have unique indications to VKAs, such as patients with mechanical prostheses, rheumatic mitral stenosis, single coagulation factor disorders (e.g., anti-phospholipid antibodies), and with stable INR.
Converting TAO centers into DOAC centers may be envisioned, with the specific aim of optimizing the management of VKA to DOAC transition, the referral of naïve patient to DOAC therapy, the intermediate controls, and the restorations of therapeutic plans, as well as the management of adverse events. However, this transformation in principle may introduce the risk of regional disparities. The prescription of DOACs in naïve patients and the transition from VKAs to DOACs in patients with low TTR, should be managed by the specialist (cardiologist, internist, neurologist) who can follow the patient directly. There was no consensus in the panel on the control and management of the possible adverse events by the GP.
The panel debated the operational weaknesses related to the TAO to DOAC centers, as the number of DOAC therapeutic plans is constantly increasing (e.g., according to data provided by the Lazio region, around 3,000/month new DOAC therapy are currently established), leading to saturation of the planning of health services in the following year [25].
A further issue discussed by the panel is the lack of clinical documentation (echocardiogram or updated biochemical tests) suitable for the follow-up visits of the patient at the referral center, as suggested by guidelines and consensus papers [4],[24],[26].
In August 2018, a consensus document from SIMG-FCSA (Società Italiana di Medicina Generale e delle cure primarie – Federazione Centri per la diagnosi e la Sorveglianza delle terapie Antitrombotiche) was issued on the correct anticoagulation procedures, gathering the opinions of different experts on the theme of clinical/organizational course for an integrated management of DOAC [27]. This document highlights that DOACs represent therapeutic agents of great social impact (improving the quality of life of patients), and underscores that their use must be managed appropriately and dutifully, by exploiting the collaboration among all the health figures involved, to improve drug effectiveness and safety. Therefore, it is proposed a model of shared and integrated management also for DOACs, which includes a close, collaborative, and interactive action among GPs, thrombosis centers, and specialists, with the aim of improving the quality of life of patients, and ensuring prescription appropriateness and a level of assistance of high quality with regard to efficacy and safety [27].
The health management of patients treated with DOACs (at first visit and at follow-up) is currently performed by the TAO center, or by the specialist who takes care of the patient, ensuring the required appropriateness and the consequent safety and efficacy of the treatment. Given the strategic role of the GPs in the follow-up of patients treated with DOACs, for ensuring prescription appropriateness, it is proposed to involve GPs in the implementation of an integrated management project, similar to that existing for the management of VKAs.
Oncological patients with NVAF or VTE (topics 8 and 9)
Participants agreed on the use of therapy with DOACs in oncological patients with NVAF. However, the importance of a careful evaluation of possible interactions with drugs administered in these patients for cancer therapy was underlined ([Table 8], statement 8.1, 8.2). This consensus derives from the results of subgroup analyses of patients with cancer enrolled in clinical trials on DOACs therapy in AF, as reported in the results of a sub-analysis on oncological patients cancer in the ENGAGE AF-TIMI 48 study [28], and from the Hokusai VTE Cancer trial, which evaluated safety and efficacy of edoxaban in oncological patients with VTE [29]. Although these data were about patients treated for a different indication (VTE instead of AF), they added important information on safety of edoxaban in cancer patients, given the large number of antineoplastic and chemotherapeutic agents used in the study [29],[30].
Table 8. Statements 8 on DOACs use in oncological patients with NVAF
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 8.1 DOACs can be administered as in any other patients |
3 |
16 |
13 |
19 |
11 |
62 |
|
31% |
69% |
100% |
| 8.2 DOACs can only be administered if they do not interact with anti-cancer treatments |
1 |
1 |
20 |
22 |
18 |
62 |
|
3% |
97% |
100% |
| 8.3 DOACs should never be administered |
29 |
30 |
3 |
0 |
0 |
62 |
|
95% |
5% |
100% |
Based on the recent results of the prospective trial Hokusai VTE Cancer [29], a general consensus was reached on the use of DOACs in the setting of patients with VTE and cancer ([Table 9], statement 9.1-9.3.).
Table 9. Statements 9 on the use of DOACs in oncological patients with VTE
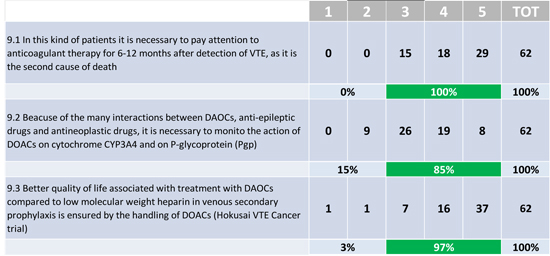
Regarding the neoplastic patient, the panel expressed a general consensus on the use of DOACs, following recent studies that demonstrated efficacy, safety, and compatibility with antineoplastic and chemotherapeutic agents [29],[30]. However, a drug warning is maintained in the subgroup of patients with gastric and intestinal neoplasms, where a higher degree of bleeding was observed, compared to low molecular weight heparin administered by subcutaneous injection [29]. Until 2017 the guidelines indicated low-molecular weight heparins as the sole treatment available for the secondary prophylaxis of venous thrombosis and pulmonary embolism in cancer patients [31]. At the end of 2017, the Hokusai VTE Cancer study compared edoxaban and dalteparin in the secondary prophylaxis of VTE in cancer patients. In the prospective, multicentric study with a PROBE design, edoxaban was shown to be not inferior to dalteparin in the composite endpoint of VTE recurrence and major bleeding [29]. Recurrent VTE was reduced by edoxaban: 7.9% versus 11.3% of the dalteparin group. There was an increase in major bleedings (although not fatal or life-threatening) with the DOAC, with 6.9% versus 4% of the dalteparin group. However, this increase is likely restricted to patients presenting with a randomized gastrointestinal neoplasia. The site affected by the increase in bleeding was that of the upper gastrointestinal tract. A greater proportion of gastric malignancies allocated to the edoxaban arm may have influenced the outcome [29].
Administration route, adherence to therapy and drug interactions (topics 10 and 11)
The panel expressed broad consensus that mono-administration of DOACs could end-up in greater adherence and better quality of life of patients who are often poly-treated because of co-morbidities ([Table 10], statement 10.1, 10.2). However, consensus was not reached on a real impact of the different route of administration of DOACs on adherence in clinical practice.
Table 10. Statements 10 on the route of administration and therapy adherence
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 10.1 Single aaadministartion can advantageous because it promotes adherence to therapy |
0 |
6 |
20 |
18 |
18 |
62 |
|
10% |
90% |
100% |
| 10.2 Single administration is preferable because it improves the quality of life of patients |
1 |
9 |
23 |
14 |
15 |
62 |
|
16% |
84% |
100% |
| 10.3 There are no differences in terms of adherence to therapy considering the route of administration |
9 |
31 |
15 |
6 |
1 |
62 |
|
65% |
35% |
100% |
| 10.4 In clinical practice patients prefer single administration regimen |
0 |
10 |
31 |
15 |
6 |
62 |
|
16% |
84% |
100% |
| 10.5 In clinical practice patients prefer double administration regimen |
9 |
43 |
7 |
1 |
2 |
62 |
|
84% |
16% |
100% |
| 10.6 If properly treated, patients maintain the reccomended treatment regimen for a long time |
3 |
0 |
13 |
30 |
16 |
62 |
|
5% |
95% |
100% |
| 10.7 Serioussness of AF or VTE disease and the possible treatment with anti-coagulants (in particular with DAOCs) should be clearly explained to patients |
0 |
0 |
8 |
19 |
35 |
62 |
|
0% |
100% |
100% |
| 10.8 Specific attention should be paid to the undesiderable effects reported by patients |
2 |
0 |
13 |
25 |
22 |
62 |
|
3% |
97% |
100% |
DOACs interact with commonly used drugs such as antibiotics, antifungals or antiarrhythmics [24]. The panel did not agree on the need for further discussion of the drug interactions of the DOACs, as no consolidated data are available on this point ([Table 11], statement 11.1). However, the interactions profile is standard of choice for the use of a specific DOAC. Participants state that further investigation and deeper knowledge on the interactions of each single DOAC could ensure a better safety for patients ([Table 11], statements 11.2, 11.3).
Table 11. Statements 11 on drug interactions
| 11.1 Currently, drug interactions with DOACs are poorly known and further information is needed |
1 |
21 |
16 |
16 |
8 |
62 |
|
35% |
65% |
100% |
| 11.2 The profile of drug interactions of individual DOACs is a criterion of choice for drugs of this class |
0 |
1 |
23 |
26 |
12 |
62 |
|
2% |
98% |
100% |
| 11.3 A better understanding of drug interactions of DOACs would ensure greater safety for patients |
0 |
0 |
16 |
20 |
26 |
62 |
|
0% |
100% |
100% |
Mono-therapy is certainly recognized as favoring adherence and quality of life, although this is not the main element ensuring consistency of the intake of the anticoagulant. A correct education and motivation by the prescriber of DOAC drugs should promote the patient’s awareness of the importance of daily intake of anticoagulant therapy. Adherence to treatment is usually assessed by the percentage of days in the period in which the patient has taken the therapy. An adherence of at least 80% is considered suitable, while lower percentages indicate inadequate adherence. Inconsistent adherence to VKAs were depending on the modalities of monitoring and on health systems, which are often inadequate. It can be expected that the constant dose, the easy intake mode, the modality, and the unneeded periodic controls may ensure a greater adherence to the new DOACs. Some studies on adherence with DOACs or VKAs are already available, while others are ongoing [32],[33]. Very interesting results were shown by a recent retrospective study analyzing not only the adherence to both old and new anticoagulants, but also the clinical effect of the insufficient adherence. The study was based on insurance databases that examined 64,661 patients with AF (mean age 73 years, males 56.2%), who initiated the therapy with VKAs (warfarin, 59.1%), or DOACs (dabigatran, 15,8%, rivaroxaban, 19.1%, or apixaban, 6.0%), between 2010 and 2014 [25]. During the median 1.1-year follow-up only 47.5% of patients treated with a DOAC showed adequate adherence (>80% of days with appropriate drug usage), however this fraction was significantly greater than the one of patients treated with warfarin (40.2%, p <0.001). Similarly, data of 7,265 patients from primary care practices across Germany suggest that rivaroxaban and dabigatran have a better persistence than VKA at Day 360 and that rivaroxaban was associated with better persistence and adherence than dabigatran [34],[35]. On the contrary, a population-based study in Ontario (n=125,195) recently provided data about warfarin treatment in patients aged more than 65 years: 31.8% discontinued therapy within 1 year, 43.2% discontinued therapy within 2 years, and 61.3% discontinued therapy within 5 years [36]. In conclusion, adherence to anticoagulation was generally modest in the clinical practice, but it was significantly improved by the use of DOACs. The clinical importance of good adherence to anticoagulant therapy in patients with AF was likely greater in patients at increased risk of complications (CHA2DS2-VASc ≥ 2) [37]. The work of Castellucci et al. was aimed at evaluating patient self-reported adherence to anticoagulant treatment at a third-level hemostasis and thrombosis center [38]. This is a cross-sectional observational study in patients receiving oral anticoagulation agents, both VKAs and DOACs (rivaroxaban, dabigatran and apixaban). Adherence to treatment was assessed using the Morisky scale - a questionnaire based on 4 simple questions - and the basic characteristics of the patients were assessed in association with adhesion. Among the 500 patients who completed the questionnaire, 74% were in treatment with VKAs and 26% with DOACs (79% rivaroxaban, 19% dabigatran and 2% apixaban). The 72% of patients were treated for VTE and 18% for AF. Self-reported adherence according to the Morisky scale was 56.2% in patients treated with VKAs and 57.1% in patients treated with DOACs [38]. Age, female gender, and oral intake of other drugs were predictive factors of good adherence to treatment, even after multivariate analysis. The study found that adherence to the oral anticoagulant treatment was similar in patients treated both with VKAs and DOACs. Furthermore, there were no differences in between mono-therapy and dual-therapy. The authors conclude that, as long as adherence laboratory tests to evaluate adherence to treatment with DOACs will not be generally available, the physicians must emphasize with the patient the importance of adherence at each visit. Moreover, the Morisky scale, albeit providing a simple system to evaluate the adherence to anticoagulant treatment, has not yet been validated for this purpose [38].
A retrospective cohort study in patients of the Veterans Affairs (VA) Healthcare System who started pharmacotherapy with dabigatran, rivaroxaban, or apixaban between November 2010 and January 2015 for NVAF with a CHA2DS2-VASc score ≥2, showed that adherence, determined using the prescription data and estimated by calculating the proportion of days covered (PDC) during the first year of therapy, was relatively low [39]. Clinical results, including all-cause mortality and stroke, were measured at 6 months from the initiation of therapy and were used to evaluate adherence for each DOAC. A total of 2,882 patients were included. Most were prescribed dabigatran (72.7%), then rivaroxaban (19.8%), or apixaban (7.5%). The mean PDC was 0.84 ± 0.20 for dabigatran, 0.86 ± 0.18 for rivaroxaban, and 0.89 ± 0.14 for apixaban (p <0.01). The percentage of non-adherent patients (PDC <0.80) was 27.6% in general and was variable according to the DOAC administered. Low adherence to dabigatran was associated with a higher risk of mortality and stroke (HR 1.07; 95% CI 1.03-1.12 for a decrease of 0.10 PDC). The study concluded that in a real-life population of patients whom an anticoagulant was prescribed for AF, more than a quarter of patients showed non-optimal adherence [39]. Low adherence was associated with a higher risk of mortality and stroke. Efforts to identify non-adherent patients and adherence interventions are needed to improve outcomes. It should however be emphasized that the impact of mono- or dual-therapy of the DOAC on adherence remains under discussion yet. In a review of 76 studies, compliance with single-dose administration and twice-daily dosing was 79 ± 14% and 69 ± 15%, respectively. Therefore, in absolute terms single-dose administration was more favorable, even if the difference did not reach statistical significance [40]. In addition, data from a national Canadian survey suggest that patients prescribed and taking once daily medications (rivaroxaban or warfarin) show better compliance: approximately 30% of twice daily medications being taken once daily, with significantly more missed doses compared with once daily medications [41]. On the other hand, the EHRA Practical Guidelines clearly state that daily single-dose administration leads to greater adherence compared to twice-daily dosing in patients with cardiovascular disease [24]. When prescribing therapy with DOACs, in order to implement adherence to therapy it is essential: i) to emphasize the value of the dosage regimen in daily mono- or double-fixed-dose, and the importance of adherence to therapy; ii) to underscore that poor adherence is the main cause of ineffective drug therapy, providing simple and clear instructions; iii) to listen to the patient, his needs and hesitations aiming at personalizing the dosage regimen based on the patient's characteristics and wishes.
Low doses of DOACs, frail patients and chronic kidney disease (topics 12, 13, 14 and 15)
Participants agreed on the need to pay close attention to the use of the appropriate dosage of DOACs. In particular, the use of so-called low doses outside the pre-specified indications for each individual DOAC is strongly discouraged ([Table 12], statements 12.1, 12.2). Furthermore, the panel expresses a unanimous consensus against the use off-label of low-dose with the aim of reducing bleeding rates. The available data, in fact, do not support, but rather strongly contrast this attitude ([Table 12], statement 12.3).
Table 12. Statements 12 on safety on the use of DOACs at low doses
| 12.1 The off-label use of low doses may increase the risk of ischemic stroke |
0 |
3 |
13 |
20 |
26 |
62 |
|
5% |
95% |
100% |
| 12.2 Proper use of low doses does not result in a reduction in efficacy and safety |
2 |
8 |
21 |
20 |
11 |
62 |
|
16% |
84% |
100% |
| 12.3 The use of low doses even if off-label may increase safety by reducing the risk of bleeding |
16 |
30 |
7 |
8 |
1 |
62 |
|
74% |
26% |
100% |
Participants express preference of the use of DOACs over VKAs in frail patients needing triple therapy for coronary artery disease (CAD) and AF ([Table 13], statements 13.1, 13.2).
Table 13. Statements 13 on the use of DOACs in frail patients
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 13.1 The use of VKAs is preferable in frail patients with NVAF and CAD needing triple therapy |
20 |
35 |
7 |
0 |
0 |
62 |
|
89% |
11% |
100% |
| 13.2 The use of DOACs is preferable in frail patients with NVAF and CAD needing triple therapy |
0 |
1 |
10 |
29 |
22 |
62 |
|
2% |
98% |
100% |
In patients with GFR <30 ml/min, therapy with VKAs should be used. DOACs may be used only in the presence of specific supporting data in this patient setting ([Table 14], statements 14.1 and 14.3).
Table 14. Statements 14: on the use of DOACs in patients with NVAF and GFR <30 ml/min
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 14.1 VKAs might be used |
3 |
12 |
20 |
14 |
13 |
62 |
|
24% |
76% |
100% |
| 14.2 DOACs might be used with closer follow-up visits |
10 |
18 |
21 |
29 |
4 |
82 |
|
34% |
66% |
100% |
| 14.3 Only DOACs with available data on low-doses might be used |
9 |
4 |
24 |
16 |
9 |
62 |
|
21% |
79% |
100% |
| 14.4 DOACs should be used based on clinical experience and individual patient characteristics |
13 |
15 |
15 |
12 |
7 |
62 |
|
45% |
55% |
100% |
The population of frail patients is a broad category well represented in clinical trials and real-world evidence. Therefore, convincing data are available on the use of DOACs in these patients. Wide consensus was expressed on the use of DOACs as an advantage for frail patients also in terms of safety ([Table 15], statement 15.1), even in the presence of renal disease. Most of all, when DOACs have been specially tested in these settings ([Table 15], statements 15.3 and 15.4).
Table 15. Statements 15: The use of DOACs is particularly beneficial in frail patients
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 15.1 Yes, because of higher safety |
0 |
2 |
15 |
14 |
31 |
62 |
|
3% |
97% |
100% |
| 15.2 No, treatment with VKAs is preferable particularly in frail patients with moderate to severe renal disease |
10 |
37 |
10 |
5 |
0 |
62 |
|
76% |
24% |
100% |
| 15.3 Only together with closer follow-up visits |
1 |
14 |
24 |
19 |
4 |
62 |
|
24% |
76% |
100% |
| 15.4 Only if DOACs may be used at low doses according to product data sheet |
2 |
18 |
29 |
9 |
4 |
62 |
|
32% |
68% |
100% |
The defensive medicine has probably exceeded in using low dosages beyond the actual indications of the technical data sheets. An improper use of low doses is possibly the consequence of the attempt to further improve the safety of anticoagulant therapy in subgroups of patients who are considered frail. However, the inappropriate use of low dosages can lead to severe consequences on drug efficacy. All DOACs currently on the market have two doses that are indicated for the prevention of ischemic stroke and systemic embolism in patients with NVAF [42]. Although these dosages are generally defined as full dosages and reduced dosages, they exhibit significant differences indeed, both from a pharmacological and clinical point of view. These differences derive mainly from the diverse design of the pivotal studies of the four DOACs.
In the RE-LY study, patients were randomized in open into three homogeneous groups, dabigatran 150 mg bid, dabigatran 110 mg bid, and warfarin with adjusted doses, to maintain INR between 2.0 and 3.0 [5]. In ARISTOTLE, ENGAGE AF-TIMI 48, and ROCKET AF studies, the enrollment included two arms: 1) a warfarin arm with adjusted doses to maintain the INR between 2.0 and 3.0, and 2) an arm with apixaban 5 mg bid, edoxaban 60 mg/day (randomized to another arm receiving edoxaban 30 mg/day which did not reach the first outcome), and rivaroxaban 20 mg/day in the three studies respectively [6]-[8]. In the DOAC arms, the dose reduction was allowed (to 2.5 mg bid for apixaban, 30 mg/day for edoxaban (or 15 mg/day for the second arm not reaching the first outcome and so not on commerce), and 15 mg/day for rivaroxaban, respectively), based on characteristics differently pre-specified in the three studies (two or more characteristics among age ≥80 years, weight ≤60 kg, and serum creatinine ≥1.5 mg/dl for apixaban; one or more characteristics among creatinine clearance 30-50 ml/min, weight ≤60 kg, and concomitant use of P-glycoprotein inhibitors for edoxaban; creatinine clearance 30-49 ml/min for rivaroxaban). This dose reduction was based on the results of phase II studies on the plasma concentrations of these drugs [43],[44]. In practical terms, these results prompt to issue a strong recommendation for the clinician to carefully follow the dose reduction criteria for each factor Xa inhibitor, to ensure the most effective and safe dosage to each patient [24]. To date, the prescriptions for the DOAC category in Italy has exceeded VKAs (corresponding to a market share of 54% versus 46%, according to the IMS Health data of December 2017), in a market steered essentially by drivers on safety, as demonstrated also in the survey produced by ARCA Biopharma [45]. Currently, about 40% of the patients are administered the reduced dosage of factor Xa inhibitors and 60% of patients in treatment with dabigatran take the 110 mg bid dose. The fractions of patients treated with low doses strongly differ from those of the pivotal studies (5% for apixaban 2.5 bid, 25% for edoxaban 30 mg/day and 20% for rivaroxaban 15 mg/day) [6]-[8]. The overprescribing of low doses for factor Xa inhibitors may be a sign of frequent underdosing of the DOACs, resulting in the exposure of a proportion of patients to a greater risk of brain and systemic embolism. This hypothesis is supported by observational data obtained in the real-world setting that show that the use of reduced doses beyond the pre-specified conditions, may not provide adequate protection against cardioembolic events [37],[46].
Statement 14 analyzes the possibility of administering DOACs in patients with NVAF and GFR below 30 ml/min. The expert panel recommend reducing the time interval between renal function controls (although a consensus has not been reached on this point), and reiterates that DOACs can be used in these patients only in the presence of supporting evidence. Chronic kidney disease is common in patients with AF. A European register reported a prevalence of mild and moderate-severe renal failure in 47% and 18% of patients with AF, respectively [47]. Chronic renal failure is also associated with the increased risk of both thrombotic and hemorrhagic events, compared to patients with AF and normal renal function. Since all DOACs are, at least partially, eliminated by the renal route, the prescription of these drugs requires an assessment of renal function before initiating the therapy and regularly during treatment. In this regard, a recent study has shown that, similar to what has already been reported for patients treated with warfarin or aspirin, renal failure increases the risk of bleeding also in patients treated with DOACs [48]. Therefore, it is important to monitor renal function regularly in patients with AF who have been prescribed a DOAC, and to try identifying the patients who may experience worsening of renal function over time (e.g., patients with already reduced renal function, advanced age, heart failure, or contraindicated therapies). In the DOAC pivotal studies, renal function was evaluated using the Cockcroft-Gault equation, which provides an estimate of GFR (eGFR), taking into account the patient's age, sex, weight, and creatinine levels. A recent study by Becattini et al. evaluated 449 patients with NVAF (mean age 79 years) who were followed prospectively from the first prescription of a DOAC [49]. In this study the renal function was evaluated at regular intervals (every 3-6 months or when required by clinical reasons) using the Cockcroft-Gault equation, and was classified into 5 stages: 1.) conserved renal function (eGFR ≥90 ml/min); 2.) slight reduction in renal function (eGFR 60-89 ml/min); 3.) moderate reduction of renal function (eGFR 30-59 ml/min); 4.) severe reduction of renal function (eGFR 15-30 ml/min); 5.) pre-dialysis (eGFR <15 ml/min). The aim of this study was analyzing the frequency of changes in renal function in patients with AF and the consequence on the hemorrhagic risk during DOAC therapy. A deterioration in renal function causing staging changes occurred in 34% of patients. The advanced age and the presence of heart failure were independent factors associated with the worsening of renal function. During an average follow-up of 1.5 years, the incidence rate of major bleeding was 6.1% per patient/year and that of non-major, but clinically-relevant bleeding was 9.3% per patient/year. The eGFR was an independent risk factor for bleeding complications: each reduction of 1.0 ml/min of the eGFR was associated with a 2% increase in the risk of major bleeding. Furthermore, the change in staging of renal function was associated with an approximately 2-fold increase in the risk of major bleeding after age adjustment, diabetes and heart failure [49]. According to the opinion of the expert panel the advantage of DOACs compared to VKAs in the frail patient resides in the increased safety also in the subgroup with mild renal failure. The panel agrees on the need to increase the frequency of controls in frail patients [50],[51].
Limits to the use of DOACs (topic 16)
On the limits to the use of DOACs, participants did not reach any consensus ([Table 16], statements 16.1-16.4). The main limitation to the use of DOACs can no longer be charged to i) the higher cost in terms of single tablet compared to warfarin, ii) time spent to fill out the treatment plan, iii) the need for adequate information for GPs, and not even to iv) the issue of who and how patients treated with DOACs should be monitored in term of follow-up visits and adherence to therapy.
Table 16. Statements 16 on the main limit on DOACs use
|
1 |
2 |
3 |
4 |
5 |
TOT |
| 16.1 Costs |
12 |
18 |
11 |
10 |
11 |
62 |
|
48% |
52% |
100% |
| 16.2 Need for therapeutic plan |
9 |
14 |
16 |
11 |
12 |
62 |
|
37% |
63% |
100% |
| 16.3 Insufficient knowledge of the drug by GPs |
5 |
17 |
20 |
12 |
8 |
62 |
|
35% |
65% |
100% |
| 16.4 Management of follow-up visits and adherence uncertainty |
12 |
26 |
14 |
8 |
2 |
62 |
|
61% |
39% |
100% |
Regarding the statement 16 there is no consensus that the cost of the DOACs represents a limit for their use. There is consensus instead that the time required to complete the treatment plans and the insufficient information of the GPs are barriers to the use of the DOACs. On the contrary, the panel has reached no consensus on the fact that the uncertainty about who oversees the follow-up and adherence controls is a limiting factor to the use of DOACs.






