Selective Activation Re-Mapping Reveals the Mechanism in Apparently Unstable Atrial Tachycardias.
Ioannidis P1, Zografos T2, Vassilopoulos C1, Christoforatou E1, Dadous G3, Skeberis V4, Sakadamis G3, Kanonidis I3
1
Heart Rhythm Center, Athens Bioclinic, Athens, Greece
.2
Third Department of Cardiology, Hygeia Hospital, Athens, Greece
.3
Second Department of Cardiology, Aristotle University of Thessaloniki, Thessaloniki, Greece
.4
Third Department of Cardiology, Aristotle University of Thessaloniki, Thessaloniki, Greece
.
Following atrial fibrillation (AF) ablation procedures, patients may present with atrial tachycardias (ATs) that show remarkable stability for short periods of time but degenerate in unstable forms right afterwards. In order to map these types of ATs, we applied the sequential mapping capabilities only for time segments where ATs exhibited constant cycle length (CL) and activation sequence, excluding the segments with unstable recordings.
We herein describe two cases of ATs after AF ablation which were mapped with this technique that allowed for the successful identification and subsequent ablation of the tachycardia circuit.
Key Words : Atrial fibrillation, Atrial Tachycardias, Pulmonary Vein Isolation.
Correspondence to: Panagiotis Ioannidis,
15 M. Geroulanou Str, 11524, Athens, Greece
The evaluation of impulse propagation mapping during atrial fibrillation (AF) or unstable atrial tachycardias (ATs) requires simultaneous mapping, which is a subject of research and current clinical applications. Sequential mapping can only be used in stable ATs in order to disclose their mechanism. Advanced 3D mapping systems have the ability to perform reliable activation maps in a very short period of time in stable ATs. After AF ablation procedures, it is not unusual to be confronted with ATs that show remarkable stability for short periods of time, but degenerate in unstable forms right afterwards. In an attempt to map these types of ATs, we applied the sequential mapping capabilities only for time segments where ATs exhibited constant cycle length (CL) and activation sequence, excluding the segments with unstable recordings.
We describe two cases of ATs after AF ablation that were mapped using the EnSite Precision™ Cardiac Mapping System (Abbott Laboratories, Chicago, IL, USA) via the AutoMap module.
A 69-year-old woman with paroxysmal AF and pulmonary vein isolation (PVI) plus cavotricuspid isthmus (CTI) ablation procedure 13 months ago, presented with symptomatic persistent AT and underwent electrophysiological study and ablation. In the EP Lab the patient was in AT and all the pulmonary veins remained isolated. The AT mapping procedure was performed with continuous movement of the circular catheter which was continuously collecting points. Unfortunately, the AT was not stable throughout this process. In the retrospective analysis, points obtained at time intervals where the tachycardia presented with unstable and complex sequence were discarded. Therefore, the propagation map was based only on points collected in stable AT intervals. A clockwise perimitral circuit was clearly discernible (Video 1). During mitral isthmus (MI) ablation the tachycardia terminated and the MI line block was proved in sinus rhythm [Figure 1]. The patient 14 months after the ablation was free from any atrial tachyarrhythmia off antiarrhythmic drugs.
Figure 1. The selective activation mapping in the 1st case. The AT has initially constant sequence switching to an unstable form and inversely (A). The collection of points during the movement of the catheters occurs only for the periods that the tachycardia was stable. In the retrospective analysis of the entire recording, the points obtained at time intervals where the tachycardia presented with unstable and complex sequence (interval within dotted lines) were discarded. The propagation map obtained from this process showed a clockwise perimitral circuit (B) (video 1). It is worth mentioning that the AT initially has a CL of 205 ms (C1). When this slightly decreased to 187ms, the AT becomes complex and non-susceptible to sequential mapping (C2). Furthermore, in the tracing C2 we observe that the sequence in the coronary sinus (CS) for several beats remains the same (distal to proximal). Probably, the faster AT rate leads some parts of the atrial myocardium to conduct in a fibrillatory manner (schematic drawings), with different conduction velocities providing finally a completely disorganized AT appearance.

A74-year-old woman 69 months after the initial AF ablation (PVI plus CTI ablation) was admitted for electrophysiological study due to persistent AT. In a similar manner to Case 1, after PVI confirmation, following sequential mapping of the tachycardia, we retrospectively rejected the segments where the tachycardia became unstable. We thus constructed a propagation map which clearly showed a counterclockwise circuit around the mitral annulus (Video 2). The patient received MI ablation and, notably, at the time of MI line completion, while the tachycardia remained unstable, eventually sinus rhythm was restored [Figure 2]. The patient had no arrhythmia recurrence after the procedure for 12 months off antiarrhythmic drugs.
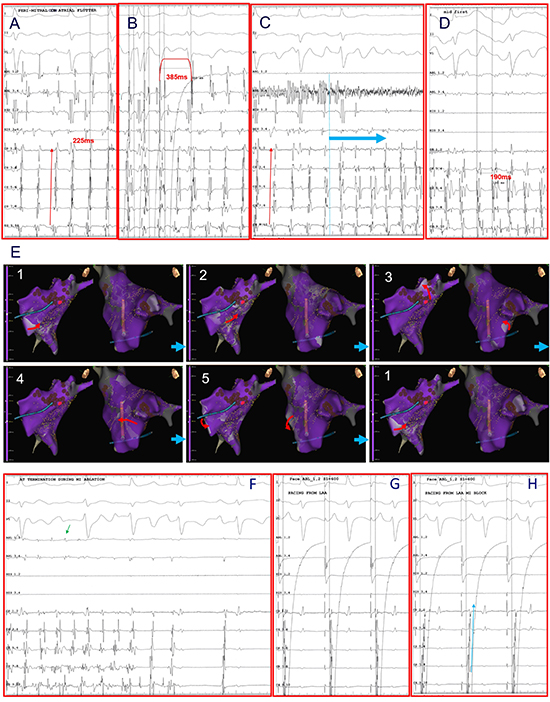
Figure 2. AT long after AF ablation in the 2nd patient, with CL of 225ms, and proximal to distal activation in CS (A). The tachycardia was mapped with rapid collection of points by moving the circular catheter to the LA. The entrainment mapping was negative from the CTI (B). The tachycardia after a few seconds lost its sequence stability (light blue arrow), with a small decrease in the CL at 190ms (C, D). In the retrospective analysis, the time segment where the tachycardia started to be unstable was rejected. Thus, the propagation map was based only at the points collected during the few seconds where the tachycardia showed CL and activation stability. The propagation map clearly showed a counterclockwise circuit around the mitral annulus (E, video 2). At the time of MI line completion, while the tachycardia remained unstable, eventually the sinus rhythm was restored (F). It is worth noting, that the tachycardia termination occurred in a non-fragmented atrial electrogram in MI (green arrow) (F). In sinus rhythm the MI line was completed with an apparent change in CS activation sequence during LAA pacing (G, H).
It is clear that in real time, an unstable AT could not be mapped with sequential mapping procedures due to disorganization and fibrillatory conduction. In this case, by failing to disclose the mechanism, we would probably be led to empirical complex fractionated atrial electrograms (CFAE) ablation. Probably, these areas represent decremental and fibrillatory conduction not critical for AF-AT maintenance, while the initial tachycardia continues [1]. The fact that in both cases the tachycardia terminated during MI completion probably supports the hypothesis that a macro-reentrant circuit is the main maintenance mechanism of these arrhythmias.
Therefore, if the areas of decremental and fibrillatory conduction do not represent critical areas in the maintenance of the arrhythmia, attempting to eradicate them, apart from not having a successful effect, would take time out of the procedure, depriving the possibility of intervening to the responsible mechanism. Indeed, if all the areas that show decremental conduction characteristics were gradually eliminated, an organized tachycardia could be emerged that would be susceptible to sequential mapping. This phenomenon is not uncommon in clinical practice since the abolition of CFAEs leads to organization of the arrhythmia in certain cases. On the other hand, the inability to ablate all responsible areas will not probably reach this result.
These findings may be indicative that some unstable ATs appearing as AF, can be produced from the existence of one or more tachycardia sources [2,3]. It would be ideal if the future pursuit, insofar as simultaneous mapping is not technically feasible or absolutely reliable, to have a fast sequential mapping. This can be achieved by using special multipolar catheters that are capable to obtain high density maps. At the same time, it is technically feasible to create softwares that will facilitate the focusing, by manual or automatic capabilities, on time periods where the tachycardia exhibits stability in terms of CL and activation sequence.
By describing the above cases we underline the possibility that, in selected cases, specific macro-reentrant circuits may drive the maintenance of unstable ATs or AF. However, we do not overlook the fact that some other drivers can also contribute to the maintenance of an unstable AT or AF. Nevertheless, it is likely that the ablation of an existing and hardly disclosable macro-reentrant circuit could prevent arrhythmia recurrence.
Video Links :
Link for Video 1
http://www.jafib.com/PMC/XML/Inprogress/2152/Multimedia_1.mp4
Link for Video 2
http://www.jafib.com/PMC/XML/Inprogress/2152/Multimedia_2.mp4






