Evidence-Based Case Report: The Use of D-Dimer Assay to Exclude Left Atrial Thrombus in Patient with Atrial Fibrillation >48 Hours
Raymond Pranata1, Emir Yonas2, Veresa Chintya 3, Alexander Edo Tondas 4, Sunu Budhi Raharjo5
1Faculty of Medicine, Universitas Pelita Harapan, Tangerang, Indonesia.2Faculty of Medicine, Universitas YARSI, Jakarta, Indonesia.3Faculty of Medicine, Universitas Kristen Krida Wacana, Jakarta, Indonesia.4Department of Cardiology and Vascular Medicine, Faculty of Medicine Universitas Sriwijaya, Dr. Mohammad Husein General Hospital, Palembang, Indonesia.5Department of Cardiology and Vascular Medicine, Faculty of Medicine Universitas Indonesia, National Cardiovascular Center Harapan Kita, Jakarta, Indonesia .
Patients with atrial fibrillation (AF) for >48 hours who are a candidate for cardioversion should have transesophageal echocardiography (TEE) performed to exclude left atrial thrombus (LAT) that may cause systemic thromboembolism upon conversion to sinus rhythm. However, TEE facilities were limited, especially in developing countries.
A 50 years-old man presented with exertional dyspnea and palpitation for 72 hours prior to admission. Electrocardiography showed AF with a ventricular rate of 140x/minute. Cardioversion was decided to be the best approach. This patient has an AF >48 hours of onset, hence, LAT should be excluded by the use of TEE. Unfortunately, there was no TEE facility nearby.
Upon comprehensive search on the use of D-Dimer assay to exclude the LAT in AF patients, we found seven studies showed increased D-dimer level in those with left atrial thrombus. In 4 studies, AUC was > 0.70, sensitivity and specificity varied from 75.9% to 89% and 73.1% to 95% respectively. However, there is no single cut-off point, due to the heterogeneity of cut-off points.
D-dimer assay combined with other variables of atrial thrombus exclusion score is valuable in excluding LAT. Previously, weeks of anticoagulation is more advisable before attempting cardioversion in the absence of nearby TEE facilities. With current evidence, a low D-dimer and ATE score of 0 is safe for cardioversion.
Key Words : Atrial Fibrillation, D-dimer assay, Left atrial thrombus, Cardioversion, Thromboembolism.
Correspondence to: Raymond Pranata
Faculty of Medicine, Universitas Pelita Harapan, Tangerang, Banten, Indonesia
Patients with atrial fibrillation (AF) for >48 hours who are a candidate for cardioversion should have transesophageal echocardiography (TEE) performed to exclude left atrial thrombus (LAT) that may cause systemic thromboembolism upon conversion to sinus rhythm. However, TEE facilities were limited mainly in developing countries and left atrial appendage may be a challenge to visualize by transthoracic echocardiography. In this article, we would like to discuss a patient that presented with AF >48 hours and is a candidate for cardioversion, however, there is no TEE at the facility. We performed a comprehensive search on whether d-dimer assay can be used to exclude LAT in this patient in order to perform safe cardioversion.
A 50 years-old man presented with exertional dyspnea and palpitation for 72 hours prior to admission. There was no chest pain, episode of syncope, or edema. The patient was limited by symptoms but hemodynamically stable. Electrocardiography showed AF with a ventricular rate of 140x/minute. The patient has a history of hypertension on treatment with captopril. There was no history of stroke and heart failure. There was no apparent reversible cause of AF based on a panel of laboratory examinations (Including a D-Dimer <250 ng/ml DDU). Based on CHADVASC scoring, this patient has a score of 1, a 0 Wells DVT score for thromboembolic probability, and a HAS-BLED Score of 1 for bleeding probability while on anticoagulants. After considerations, it was decided that cardioversion into sinus rhythm would be the best approach in this patient. This patient has an AF >48 hours of onset, hence, LAT should be excluded by the use of TEE. Unfortunately, there was no TEE facility nearby. The patient was anticoagulated for weeks, cardioversion was performed, and AF was converted into sinus rhythm. On 6 months’ follow-up, the patient remained in sinus rhythm.
The clinical question is whether d-dimer assay can be used to exclude the diagnosis of LAT in patients presenting with AF >48 hours without the use of TEE or should patients be anticoagulated for weeks before attempting cardioversion. To answer this question, two independent authors (E.Y and V.C) performed a comprehensive and systematic search on studies on the use of D-Dimer assay to exclude the left atrial thrombus in patients with atrial fibrillation presenting >48 hours with keywords [“d-dimer”, “left atrial thrombus” and “atrial fibrillation”] and its synonym from inception up until June 2019 through PubMed, EBSCOhost, Cochrane CENTRAL, Proquest, EuropePMC, and hand-sampling from article references, discrepancies were resolved by discussion. Data extraction and quality assessment using appraisal tools from the Center of Evidence-Based Medicine, the University of Oxford was done by two independent authors (R.P and V.C). We included original articles and systematic reviews. We found a total of 182 unique results, 9 were relevant through screening of titles/abstract and the full-texts were assessed for eligibility [Figure 1] After excluding duplicate, applying inclusion criteria and performing critical appraisal using Oxford CEBM tools, we included seven studies [Table 1] and [Table 2] . All seven studies founded that D-dimer level significantly elevated in a group with LAT. Five were cross-sectional studies; one was a cohort and a systematic review. [Table 3]
Figure 1. Flow Chart of Search Strategy
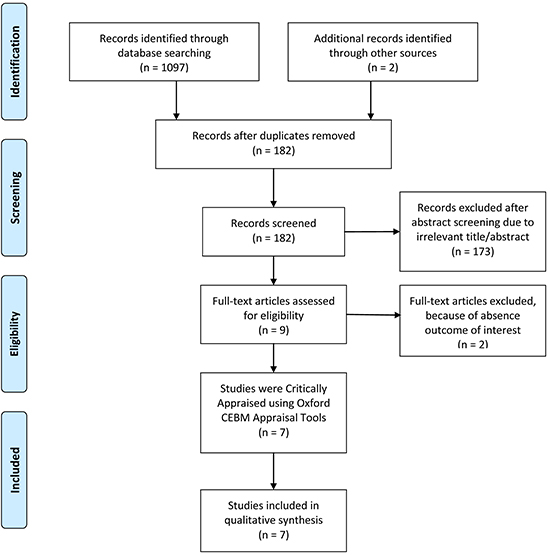
Table 1. Critical appraisal of four studies based on criteria by centre of evidence medicine University of Oxford
|
|
|
|
Validity |
|
Applicability |
|
| Articles |
Year |
Study Design |
Representative Spectrum |
Reference Standard Applied |
Independent, blind Comparison |
Applicability |
Level of Evidence |
| Milhem et al |
2019 |
Cross-Section |
+ |
+ |
+ |
+ |
1 |
| Du et al |
2019 |
Cross-Section |
+ |
+ |
+ |
+ |
2 |
| Tarnowski et al |
2018 |
Cross-Section |
? |
+ |
? |
+ |
2 |
| Bejinariu et al |
2016 |
Cross-Section |
+ |
+ |
+ |
+ |
2 |
| Habara et al |
2007 |
Cross-Section |
+ |
+ |
+ |
+ |
2 |
| Somloi et al |
2003 |
Prospective Observational Cohort |
+ |
+ |
+ |
+ |
2 |
Table 2. Critical appraisal of a systematic review based on criteria by centre of evidence medicine University of Oxford
| Article(s) |
Year |
PICO |
Appropriate Searching |
Relevant Study Included |
Quality assessment of Trial |
Heterogeneity |
Level of Evidence |
| Wan, et al |
2017 |
+ |
+ |
+ |
+ |
+ |
1 |
+ = Positive, - = negative, ? = Unclear. VIA was assessed using Oxford CEBM Appraisal Tools.
Table 3. Summary of studies included
| Author |
Year |
Study Type |
Sample (n) |
Outcome of Interest |
Results |
Summary |
| Milhem et al |
2019 |
Cross-section |
2494 |
Plasma D-dimer levels and clinical data, to rule out a diagnosis of atrial thrombus before catheter ablation of AF. |
D-dimer > 270 ng/mL was associated with adjusted OR of 2.29 (1.25–4.16) p=0.0070
The authors also proposed a score consisting of history of stroke, congestive heart failure, high plasma D-dimer level, and hypertension called atrial thrombus exclusion (ATE) score
|
D-dimers > 270 ng/mL combined with history of stroke, congestive heart failure, and hypertension is predictive of LAT |
| Du et al |
2019 |
Cross-section |
113 |
Plasma D-dimer levels and cardiac computed tomography angiography, to detect LAT |
Age-adjusted D-dimer has sensitivity= 100.0%, specificity= 86.7%, PPV= 51.7%, NPV= 100.0%
Combined with cardiac computed tomography angiography; sensitivity= 100.0%, specificity= 97.9%, PPV= 88.2%, and NPV= 100.0%
|
Age-adjusted D-dimer is reliable in predicting LAT especially when combined with cardiac computed tomography angiography |
| Tarnowski et al |
2018 |
Cross-section |
108 |
D-dimer level in patients with and without LAT in AF patients prior to electrical cardioversion or PVI |
D-dimer (0.13 ± 0.02 vs.0.69 ± 0.21, p=0.015) were significantly elevated in patients with AF and detected LAT. In regard to the ROC, D-dimer showed an AUC of 0.77. However, D-dimer levels above the conventional cut-off of 5 mg/L (500 ng/mL) indicated LAT with a sensitivity of only 35% and a corresponding specificity of 95% (OR 4.41, 95% CI. 0.6–31.1, p = 0.14). |
D-Dimer were elevated in presence of LAT but lost their quality as independent predictor using conventional cut-off value |
| Bejinariu et al |
2016 |
Cross-section |
372 |
D-dimer level in patients with and without LAA Thrombus in AF patients prior to cardioversion |
1. multivariate logistic regression analysis predicting likelihood of thrombus formation in LAA For D-Dimer (OR 1.055, 95% CI 0.783–1.420, p = 0.725)
2. Ordinal logistic regression For D-dimer (OR 1.027, 95% CI 0.833–1.266, p = 0.806)
|
Biomarkers (Including D-dimer) failed to predict the outcome |
| Habara et al |
2007 |
Cross-section |
925 |
D-dimer level in patients with and without LAT in non valvular AF patients |
1. D-dimer levels (OR 97.6, 95% CI 17.3–595.8, P,0.0001).
LAA thrombi were detected in 21.8% of patients with higher D-dimer values, whereas it was detected in
only 3.1% of patients with lower D-dimer values.
2. D-dimer > 1.15 µg/ml (1150 ng/ml); AUC: 0.80, 95% CI 0.75–0.85
At a cutoff level of 1.15 µg/mL, the sensitivity was 75.9% (95% CI 65–85), specificity 73.1% (95% CI 70–76%), PPV 21.7% (95% CI 17–27%), and NPV 97.0% (95% CI 95–98) for identifying thrombi in LAA.
|
D-dimer cutoff level of 1150 ng/mL had a negative predictive value of 97% for identifying LAA thrombi. |
| Somloi et al |
2003 |
Prospective Cohort |
75 |
D-dimer measured before TEE in 75 consecutive patients referred for TEE before cardioversion for AF or flutter >48 hours |
ROC Curve, AUC 0.78 (95% CI: 0.63-0.93, p=0.007). Cut-off value of 0.6 µg/mL (600 ng/mL) yields a sensitivity 89% and specificity 75%. PPV 33% and NPV 98%. |
D-dimer cut off value is 0.6 ug/mL |
| Wan et al |
|
Systematic Review and Meta-analysis |
|
D-dimer and presence of LAT or Spontaneous Echo Contrast |
1. Pooled standardized mean difference (SMD) of D-dimer between patients with and without left atrial SEC and/or LAT was 1.29 (95% CI: 0.51, 2.08), with SMDs of 0.42 (95% CI: 0.08, 0.77) and 2.34 (95% CI: 1.01, 3.68) in SEC/LAT and LAT subgroups, respectively.
2. The combined RR of the presence of LAT among individuals between the top of the distribution of d-dimer levels and that in the bottom third was 3.84 (95% CI: 2.35, 6.28), associating with a mean difference of 0.78 ug/ml (1.10 vs 0.32 µg/ml).
3. D-Dimer for LAT Sensitivity 0.75 (95% CI: 0.65, 0.83), specificity 0.81 (95% CI: 0.59, 0.93) and positive likelihood ratio 4.0 (95% CI: 1.7, 9.9]
Range cut off 125 ng/ml – 4000 ng/ml
|
High plasma fibrin DD was associated with left atrial SEC/LAT, particularly among patients with LAT. DD levels have moderate sensitivity and specificity for diagnosing LAT |
Description: AUC=Area Under Curve, LA=Left Atrium, LAA=Left Atrial Appendage, LAT=Left Atrial Thrombus, NPV=Negative Predictive Value, PPV=Positive Predictive Value, ROC=Receiver Operating Characteristic, SEC=Spontaneous Echo Contrast.
Direct current cardioversion into sinus rhythm on patients with AF >48 hours may cause systemic thromboembolism due to the presence of LAT.[1] Thrombus formation leads to increased d-dimer products which means that D-dimer assay can possibly be used to exclude LAT in AF patients. Five included studies showed that d-dimer assay was elevated in those with LAT.
For D-dimer to have clinical implication, it is important to have a cut-off point that has satisfying diagnostic performance. Habara et al. showed that d-dimer assay at 1150 ng/mL had a negative predictive value (NPV) of 97% for LAT.[2] Somloi et al. found 600 ng/mL has a sensitivity: 89% and specificity: 75%, positive predictive value (PPV): 33% and NPV: 98%.[3] Tarnowski et al. found that d-dimer were significantly elevated in patients with AF and detected LA thrombus (0.13 ± 0.02 vs.0.69 ± 0.21, p=0.015); however, it is not significant at 500 ng/mL, which is the conventional cut-off value.[4] In contrast, Bejinariu et al. revealed that d-dimer assay failed to predict the LAT.[5] Wan et al. showed that elevated D-dimer was associated with left atrial spontaneous echo contrast/ LAT with moderate sensitivity and specificity. In 4 out of 5 studies, AUC was > 0.70, sensitivity and specificity varied from 75.9% to 89% and 73.1% to 95% respectively.[6] However, there is no single cut-off point, due to the heterogeneity of cut-off points.
The findings are congruent to Yasaka et al. study who evaluate the use of d-dimer to detect LAT in patients with mitral stenosis, they found that D-dimer at 300ng/mL has sensitivity= 61%, specificity= 93%, PPV= 79%, and NPV= 86%. In their study, 44 out of 63 subjects have AF. Several patients were found to have elevated d-dimer despite the absence of intra-atrial coagulation on echocardiography which may be explained by mobile thrombi undetected on TEE. This is a possible additional benefit of D-dimer assay.[7]
Currently, there is no recommendation on D-dimer use to exclude LAT; however, the NPV of D-dimer assay is comparable to TEE in excluding left atrial thrombi. D-dimer’s effectiveness was shown to fall short to that of TEE (NPV= 98.7%; Hwang et al.) in studies performed by Habara et al. (NPV= 97%), Somloi et al. (NPV=98%), and Yasaka et al. (NPV= 86%). Thus D-dimer assay has the potential to be used to exclude LA thrombi[8]. Du et al. reported age-adjusted d-dimer assay has sensitivity= 100.0%, specificity= 86.7%, PPV= 51.7%, NPV= 100.0% for detection of LAT, the study included both valvular and non-valvular AF; an excellent diagnostic performance.[9] Du et al. study further combined cardiac computed tomography angiography to reach a sensitivity= 100.0%, specificity= 97.9%, PPV= 88.2%, and NPV= 100.0%. Hence, the combination may be valuable in the hospital without TEE but with cardiac computed tomography angiography.[9] The importance of d-dimer assay was further strengthened by a study by Milhem et al. whom suggested a d-dimer >270 ng/mL along with the history of stroke, heart failure, and hypertension formed a reliable atrial thrombus exclusion (ATE) score.[10] Milhem et al. demonstrated that an ATE score of 0 has a 0% atrial thrombus in 911 patients. While ATE score of 1 and 2 had 2.3% (out of 988 patients) and 2.9% (out of 481 patients) incidence of thrombus.[10] An ATE score of 3 and 4 had 9% (out of 111 patients) and 33.3% (out of 3 patients) incidence of atrial thrombus.[10] The ATE score is ideal in a rural hospital with limited facilities, needing only d-dimer assay and other variables that can be obtained by history taking and physical examination.
The patient in previous case illustration may benefit from cardioversion; however, those with AF >48 hours have a high risk for thromboembolism. The current recommendation is to rule out the LAT by the use of TEE. We conclude at that time (the year 2017) that there was not enough evidence to routinely recommend measurement of plasma D-dimer to rule-out LAT; hence, the safest option is to administer anticoagulation to patients for weeks before performing cardioversion in the absence of TEE facility nearby. However, with the advent of ATE score proposed by Milhem et al. in 2019; measurement of D-dimer assay in the evaluation of patient requiring exclusion of LAT is reasonable. This patient has an ATE score of 1 having a 2.3% risk of stroke, hence low but null risk of cardioversion. D-dimer assay (and ATE score) in addition to transthoracic echocardiography may be of use, especially in those with a risk score of 1 to 3, hence, we recommend further studies to evaluate this possibility.
Limitations in this study are selection bias in which only positive studies are published, hence, may lead to overestimation of diagnostic performance. These studies also have varying cut-off point, to have a clinical impact, there has to be a single cut-off point.
The authors declare no conflict of interest
Raymond Pranata conceived and designed the study and drafted the manuscript. Emir Yonas and Veresa Chintya acquired the data and drafted the manuscript. Raymond Pranata and Emir Yonas interpreted the data and performed critical appraisal. Alexander Edo Tondas and Sunu Budhi Raharjo performed extensive research and critically revised the manuscript. All authors contributed to the writing of the manuscript.
D-dimer assay is valuable in excluding LAT; especially combined other variables of ATE score. Previously, weeks of anticoagulation is more advisable before attempting cardioversion in the absence of nearby TEE facilities. With current evidence, a low D-dimer and ATE score of 0 is safe for cardioversion. Further investigations on diagnostic performance by the combined use of transthoracic echocardiography and ATE score further risk stratify those with a score of 1 to 3 may further delineate the risk of cardioversion in hospitals with limited facilities.






