Temporal Trend and Associated Risk Factors for New-Onset Atrial Fibrillation Following Cardiac Valve Surgery
Abhinav Sood, Andrew Toth, Mouin Abdallah, Marc Gillinov, Desai Milind, Klein Allan, Kanj Mohamed, David Majdalany
A.S.: Department of Cardiology, Mount Sinai Beth Israel, New York.
A.T.: Division of Quantitative Health Sciences, Lerner Research Institute, Cleveland Clinic, Cleveland.
A.G.: Division of Cardiothoracic surgery, Heart and Vascular Institute, Cleveland Clinic, Cleveland.
M.A., A.K., M.D., M.K., D.M.: Division of Cardiology, Heart and Vascular Institute, Cleveland Clinic, Cleveland.
Post cardiac surgery atrial fibrillation (POAF) is common, with adverse implications. However, relatively little is known regarding the time varying nature of risk factors associated with POAF. We describe variation in POAF along with its associated risk factors.
Medical records of adult patients undergoing cardiac valve surgery from 2003-13, without a history of pre-operative AF were analyzed retrospectively. POAF was adjudicated using inpatient and outpatient electrocardiograms (EKG). Risk of AF over time along with time-varying risk factors were estimated using multiphase non-linear logistic mixed effects model.
10,461 patients with 100,149 EKGs were analyzed [median follow-up 4 months (IQR 48 hours-2 years)]. AF prevalence changed with time since surgery and two distinct phases were identified. Prevalence peaked to 13% at 2 weeks (early phase) and 9% near 7 years post-operatively (late phase). Older age, greater severity of preoperative tricuspid valve (TV) regurgitation, mitral valve replacement and prior cardiac surgery were time-independent risk factors for POAF. TV repair was associated with a decreased risk of early phase POAF. Pre-operative blood urea nitrogen, peripheral vascular disease and hypertension were associated with a higher risk of late phase POAF.
POAF risk shows two distinct phases with an early peak and a late gradual rise, each associated with a different set of risk factors.
Key Words : Atrial fibrillation, Post-operative atrial fibrillation, Valvular heart surgery, Time varying risk.
Abhinav Sood
Mount Sinai Beth Israel
281 1st Avenue
New York, NY 10003
Atrial fibrillation (AF) is the commonest post-cardiac surgery arrhythmia with an estimated incidence between 30-50% and is associated with a significant increase in morbidity, mortality and healthcare costs[1]. Post-operative atrial fibrillation (POAF) following cardiac surgery is invariably noted within the first 5 days and commonest on the 2nd post-operative day[2]. Given the adverse impact of POAF, effective strategies for targeting POAF risk factors are expected to have momentous impact in decreasing post-operative morbidity and healthcare costs.
Risk of POAF is associated with risk factors related to surgery as well as conventional risk factors. Theoretically, these risk factors are expected to vary with time since surgery. For example, electrolyte abnormalities would be expected to have a pro-arrhythmogenic effect in the early post-operative stage, while incision related inflammation will tentatively have both short-term and long term (from scarring) implications. This is in contrast to conventional risk factors such as diabetes and hypertension, the effect of which is expected to be time-independent[3]. Characterization of this time-varying risk and identification of associated risk factors is integral to synthesizing effective programs for POAF monitoring, diagnosis and prevention.
Multiple studies have previously described POAF burden following cardiac surgery, but few have addressed its temporal pattern and the time-varying nature of risk factors influencing POAF[4]-[9]. The aim of this study is to describe the time-varying prevalence of POAF along with its associated time-varying and constant risk factors in patients undergoing cardiac valve surgery in a tertiary care hospital in the United States, without a previous history of atrial fibrillation.
This is a single-center, retrospective cohort study analyzing data of patients who underwent cardiac valve surgery at a tertiary-care center.
Patients older than 18 years undergoing cardiac valve surgery from 2003-2013, alone or in combination with coronary artery surgery were selected. Patients with a history of AF prior to surgery were excluded. Patients without at least one adjudicated pre-operative and post-operative electrocardiogram (ECG) were excluded. Patient consent for the surgical procedure was obtained prior to surgery. A waiver of informed consent for utilizing electronic medical records (EMR) was allowed by the institutional review board (IRB) since this was an observational study without any anticipated patient harm.
AF was defined utilizing AATS recommendations as its presence on an ECG lasting for greater than 30 seconds or for the duration of the reading, if less than 30 seconds[10]. History of AF was defined as either patient reported diagnosis of AF, documented history of AF in EMR or presence of a cardiologist adjudicated preoperative ECG with AF. POAF was described as the presence of a post-operative cardiologist adjudicated 12-lead ECG showing AF, either during an outpatient visit or inpatient hospitalization. Echocardiographic data was extracted from echocardiogram reports read by board qualified cardiologists.
Continuous data is described using means with standard deviations (SD) or medians with interquartile range (IQR). Categorical data is described using frequencies and percentages. Transformation of continuous variables was performed when necessary. 5-fold multiple imputation using Markov Chain Monte Carlo technique was employed to impute missing values (SAS PROC MI). In multivariate modeling, for each imputed complete dataset, their regression coefficients and variance-covariance matrices were estimated and final regression coefficient estimates, variance-covariance matrices and p-values were computed by combining estimates from the 5 models (SAS PROC MIANALYZE).
To assess the temporal trend of the prevalence of POAF (repeated binary measurements), post-operative ECG data was analyzed longitudinally for changes in prevalence of AF over time. A multiphase non-linear logistic mixed-effects model was used to resolve a number of time phases to form a temporal decomposition model and to estimate the shaping parameters at each phase[11]-[13]. PROC NLMIXED (SAS) was used to implement the temporal decomposition model. The prevalence of POAF over time was estimated by averaging the patient-specific profiles. Due to limited capabilities of variable selection in PROC NLMIXED, variable screening was done using ordinary multivariable logistic regression (PROC LOGISTIC) and a computer-intensive machine learning “bagging” method, with the assumption of independence of observations with entry criteria (.10) and stay criteria (.05)[14]. Isolated variables and their transformations were entered into the repeated measurements multivariable model one by one and a two-sided P value <0.05 was considered significant. All analyses used SAS statistical software (SAS v9.4, SAS Institute, Cary, NC).
10,461 patients undergoing cardiac valve surgery from 1/1/2003 to 12/31/2013 without a history of pre-operative AF, with at least one pre-operative and one post-operative adjudicated ECG were selected for this study. The baseline characteristics of the study cohort are described in [Table 1].
Table 1. Baseline characteristics of the study population.
| Variable |
Measure/ % of n |
Available data n (% of N) |
| Age |
61.1±13.9 |
10,461 (100) |
| Females (%) |
4,131 (39%) |
10,461 (100) |
| Race (%)
Caucasian
African-American
Other |
9,364 (90%)
548 (5.3%)
476 (4.6%) |
10,461 (100) |
| Hypertension (%) |
6,354 (61%) |
10,461 (100) |
| Peripheral artery disease (%) |
708 (6.8%) |
10,461 (100) |
| Diabetes mellitus (%)
Insulin treated
Non-insulin treated |
1,646 (15.8%)
665 (6.4%)
981 (9.4%) |
10,391 (99) |
| COPD (%) |
1,636 (16%) |
10,461 (100) |
| Smoking history (%) |
4,896 (47%) |
10,450 (99.8) |
| CHF (%) |
3,371 (32%) |
10,461 (100) |
| Myocardial infarction (%) |
2,054 (20%) |
10,461 (100) |
| Dialysis (%) |
201 (2%) |
10,461 (100) |
| CVA (%) |
808 (7.7%) |
10,461 (100) |
| Preoperative NYHA (%)
Class I
Class II
Class III
Class IV |
2,705 (27%)
4,403 (44%)
2,455 (25%)
448 (4.5%) |
10,011 (96) |
| Endocarditis (%) |
979 (9.4%) |
10,461 (100) |
| SURGICAL PROCEDURE |
|
|
| Coronary artery bypass graft |
2,900 (28%) |
10,461 (100) |
| Mitral valve surgery
Mitral valve repair
Mitral valve replacement |
9,873 (94%)
7,731 (74%)
2,142 (20%) |
10,461 (100) |
| Aortic valve surgery
Aortic valve repair
Aortic valve replacement |
2,234 (21.3%)
190 (1.8%)
2,044 (19.5%) |
10,461 (100) |
| Tricuspid valve surgery
Tricuspid valve repair
Tricuspid valve replacement |
2,019 (19%)
1,877 (18%)
142 (1%) |
10,461 (100) |
| ECHO parameters |
|
|
| Mitral valve regurgitation
Severity
1
2
3
4 |
9,469 (91%)
586 (5.6%)
1,172 (11%)
2,563 (25%)
5,148 (49%) |
10,411 (99.5) |
| Mitral valve stenosis |
592 (6.7%) |
8,734 (83) |
| Aortic valve stenosis |
1,417 (25%) |
5,701 (54) |
| Aortic valve regurgitation |
2,631 (26%) |
10,275 (98) |
| Tricuspid valve regurgitation |
5,008 (49%) |
10,321 (99) |
| Posterior wall thickness (mm) |
1.1±0.3 |
9,287 (89) |
| LVEDV Index (mL/m2) |
67.8±27 |
9,058 (87) |
| LVESV Index (mL/m2) |
27.4±19.8 |
8,911 (85) |
| LVEF (%) |
52.9±12.9 |
10,344 (99) |
| Left ventricle mass index (g/m2) |
126±43 |
8,995 (86) |
| Biochemistry |
|
|
| Creatinine (mg/dL) |
1.2±0.9 |
10,450 (99.9) |
| Blood urea nitrogen (mg/dL) |
21.6±15.3 |
10,450 (99.9) |
| eGFR (MDRD) (mL/min/m2) |
75.7±27.1 |
10,450 (99.9) |
| Total cholesterol (mg/dL) |
175±44.3 |
9,073 (87) |
| HDL cholesterol (mg/dL) |
52.2±17.7 |
9,070 (87) |
| LDL cholesterol (mg/dL) |
99.3±36.1 |
9,070 (87) |
LDL cholesterol (mg/dL) 99.3±36.1 9,070 (87) COPD: Chronic obstructive pulmonary disease CHF: Congestive heart failure CVA: Cerebrovascular accident LVEDV: Left ventricle end diastolic volume LVESV: Left ventricle end systolic volume LVEF: Left ventricle ejection fraction eGFR: Estimated glomerular filtration rate HDL: High density lipoprotein LDL: Low density lipoprotein
The mean age of patients undergoing surgery was 61 (±13.9) years, 39% of the patients were females and majority were Caucasians (90%). Hypertension was the most prevalent risk factor (61%) at baseline followed by congestive heart failure (32%). Almost half of the patients (44%) had NYHA class II symptoms. Mean ejection fraction was 53% (±13). Majority of surgeries were elective, with <1% being emergent. Mitral valve (94%) surgeries in isolation or in combination with other valves was the commonest valve surgery with three quarters being mitral valve repair. Yearly distribution of surgeries is given in [].
Supplementary Table 1. Yearly distribution of surgeries
| Year |
N = 10,461 |
Total % |
| 2003 |
1,102 |
10.5 |
| 2004 |
1,036 |
9.9 |
| 2005 |
978 |
9.3 |
| 2006 |
913 |
8.7 |
| 2007 |
868 |
8.3 |
| 200 |
1,025 |
9.8 |
| 2009 |
1,140 |
10.9 |
| 2010 |
1,217 |
11.6 |
| 2011 |
822 |
7.9 |
| 2012 |
668 |
6.4 |
| 2013 |
692 |
6.6 |
100,149 post-operative ECGs were available with a median follow-up time of 4 months (25th-75th centile 2 days- 2 years) with a range of half day to 14 years. Distribution by post-operative time is given in [].
Supplementary Table 2. ECG distribution based on post-operative time
| Time |
Number of ECGs |
Number of Patients (%) |
| ≥24 hour |
100,146 |
10,461(100) |
| ≥ 2 weeks |
48,338 |
4,962 (47.4) |
| ≥ 1 month |
43,640 |
4,278 (40.9) |
| ≥ 3 months |
38,319 |
3,641 (34.8) |
| ≥ 6 months |
35,558 |
3,444 (32.9) |
| ≥ 1 year |
31,814 |
3,161 (30.2) |
| ≥ 1.5 years |
28,823 |
2,913 (27.8) |
| ≥ 2 years |
26,250 |
2,714 (25.9) |
| ≥ 3 years |
21,993 |
2,428 (23.2) |
| ≥ 5 years |
14,564 |
1,816 (17.4) |
| ≥ 7 years |
8,569 |
1,161 (11.1) |
| ≥ 8 years |
6,146 |
893 (8.5) |
| ≥ 9 years |
4,347 |
667 (6.3) |
| ≥ 10 years |
2,933 |
468 (4.5) |
| ≥ 11 years |
1,910 |
330 (3.2) |
Temporal trend of post-operative atrial fibrillation
Prevalence of POAF changed with time since surgery. The non-linear logistic mixed-effects model yielded 2 distinct phases for the risk of being in atrial fibrillation since valve surgery. There was a sharp early peaking phase around 2 weeks post-surgery with a peak prevalence of 13% for POAF which sharply decreased to 3% at 3 months. This was followed by a gradually increasing late phase with peak prevalence of 9% at 7 years [Figure 1].
Figure 1. Temporal trend of post-operative atrial fibrillation. The table shows the corresponding values varying with time surgery.
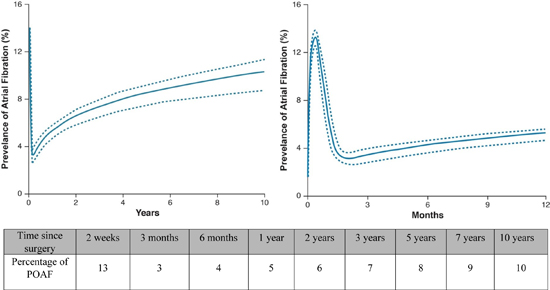
1a: Temporal trend of prevalence of post-operative atrial fibrillation. Solid lines represent the estimated parametric model of percentage of atrial fibrillation (mean effect) enclosed within a 95% bootstrap percentile confidence interval.
Risk factors associated with POAF
The statistical model yielded a set of risk factors with time-independent and dependent effects associated with POAF. Age, mitral valve replacement [OR 1.44 (1.28-1.63)], tricuspid regurgitation [OR 1.13 (1.09-1.18)] and prior cardiac surgery [OR 1.29 (1.18-1.26)] were associated with an increased risk of POAF irrespective of time since valve surgery.
In contrast, tricuspid valve repair [OR 0.86 (0.75-0.98)] was associated with a reduced risk of POAF in the early phase. Elevated blood-urea-nitrogen (BUN) levels, hypertension and peripheral artery disease were associated with an elevated risk of late-phase POAF [Table 2]. For continuous risk factors, nomograms instead of point estimates are used, and are presented in [Figure 2].
Figure 2. Nomograms for age and BUN obtained by solving the equation in table 2
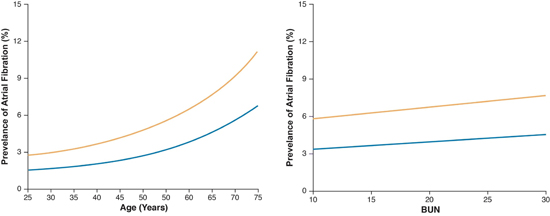
2a: Predicted effect of age on risk of POAF: Solid lines are parametric estimates of prevalence of atrial fibrillation. The 1-Year prevalence of atrial fibrillation profile is shown in blue and the 5-Year prevalence of atrial fibrillation profile is shown in yellow.
Table 2. Risk factors associated with post-operative atrial fibrillation.
| Factor |
Estimate ± SE |
P-value |
Odds Ratios (95% CI) |
| Overall |
|
|
|
| Older Agea |
0.822±0.0350 |
<.0001 |
See Figure 2a |
| Mitral Valve Replacement |
0.367±0.0616 |
<.0001 |
1.44 (1.28, 1.63) |
| Preoperative TV Regurgitation |
0.124±0.0204 |
<.0001 |
1.13 (1.09, 1.18) |
| Prior Cardiac Surgery |
0.277±0.0533 |
<.0001 |
1.29 (1.18, 1.46) |
| Early peaking phase |
|
|
|
| Surgery: Tricuspid Valve Repair (less likely) |
- 0.150±0.0691 |
0.0313 |
.86 (.75, .98) |
| Late increasing phase |
|
|
|
| Higher Preop Blood Urea Nitrogen |
0.333±0.0264 |
<.0001 |
See Figure 2b |
| History of Peripheral Arterial Disease |
0.402±0.0934 |
<.0001 |
1.49 (1.24, 1.80) |
| History of Hypertension |
0.284±0.0691 |
<.0001 |
1.33 (1.16, 1.52) |
LDL cholesterol (mg/dL) 99.3±36.1 9,070 (87) COPD: Chronic obstructive pulmonary disease CHF: Congestive heart failure CVA: Cerebrovascular accident LVEDV: Left ventricle end diastolic volume LVESV: Left ventricle end systolic volume LVEF: Left ventricle ejection fraction eGFR: Estimated glomerular filtration rate HDL: High density lipoprotein LDL: Low density lipoprotein
Risk factors associated with post-operative atrial fibrillation. Only statistically significant variables are listed in this table. The effect of risk factors listed under “overall” remained constant with time. Risk factors with time-varying effect are listed under the “early peaking phase” or “late increasing phase” as determined by the statistical model. Of note, tricuspid valve repair was associated with a decreased risk for POAF, thereby a negative precedes the point estimate Predicted prevalence of POAF with age and blood urea nitrogen.
This single-center cohort study evaluated the temporal trend of POAF prevalence since surgery and its associated risk factors following cardiac valve surgery, either in isolation or in combination with coronary artery bypass grafting at a tertiary care center from 2003 to 2013. It identified two distinct phases in the post-operative period associated with increased risk of atrial fibrillation.
Comparison with previous studies
Previous studies have been performed studying POAF and associated risk factors with varying results[4]. However, majority of these studies were done in patients undergoing primary CABG with or without concomitant valve surgery, and calculated POAF incidence which ranged from 14-47%. The peak POAF prevalence in our study was 13%, which was around 2 weeks following surgery. This is lower than the incidence rates reported in most of the previous studies. In comparison to previous studies, we excluded patients with pre-existing AF which partly explains the lower than expected prevalence in our study[4]-[9]. In addition, use of adjudicated ECGs alone without the use of continuous monitoring devices to define POAF also contributed to the lower prevalence in our study. Lastly, this is a single center study and differences in surgical techniques, intraoperative and post-operative care potentially influenced POAF rates.
Time-varying prevalence and risk factors
Although POAF risk with cardiac surgery has been extensively studied as mentioned before, utilization of a time-varying risk model has been infrequent[15]. POAF risk prediction utilizing conventional methods have yielded modest results signaling the need for novel risk prediction techniques[7]. POAF risk is not constant, with an early phase peaking near 2 weeks followed by a gradually increasing risk with peak near 7 years. The early post-operative AF risk is consistent with prior studies, although the peak time of POAF risk in our study is different compared to previous studies (2 weeks compared to 2 days). Differences in adjudicating POAF, surgical techniques and post-operative care might account for this difference. It is however, similar to the increased risk seen in phase II of a similarly modeled study by Melby et al[15]. In addition, our study evaluated the long-term risk of AF following surgery and noted late increase in risk after the initial post-operative period. This is also consistent with earlier studies[16]-[18].
Increasing age, a history of cardiac surgery as well as mitral valve replacement were time-independent risk factors for POAF. Although the mechanism underlying AF and POAF is multifactorial and incompletely understood, a combination of degenerating efficiency of myocyte electrical conduction, increased arrhythmogenicity and scarring from prior cardiac surgeries is potentially at play[3]. Preoperative tricuspid regurgitation was also a time-independent risk factor, which likely represents a surrogate marker for right atrial volume. The association of tricuspid repair in the early phase with a decrease in risk of POAF further corroborate this hypothesis, with correction of regurgitant pressure and volume load on the right atrium leading to a reduction in POAF. Late phase risk factors associated with atrial fibrillation might indicate increasing risk associated with the natural history of AF progression in general rather than POAF.
This study has limitations. Utilization of ECGs alone for diagnosis of POAF without continuous monitoring possibly underestimated POAF prevalence. Post-operative telemetry data for patients was not available and thereby unable to be included in the model. This is a limitation of the study design because this was a retrospective study incorporating patient data spanning multiple years. As mentioned before, this likely resulted in a lower reported prevalence compared to previous studies. However, description of POAF rates following cardiac surgery was not the main objective of this study since multiple elegant studies describing these rates are already available. Our aim was to highlight and analyze the variance in POAF with time and its associated risk factors. Secondly, this was a single center study at a tertiary care hospital. These results may not be generalizable to different institutions due to inter-institutional variations in surgical techniques and post-operative care. In addition, pre and post-operative bloodwork including electrolytes and medication use, including anti-arrhythmic medications, was not available for patients undergoing surgery prior to 2007 due to a change in the EMR software and was not included in the model which could be a source of bias. Despite these shortcomings, the study cohort was sizeable, all ECGs were adjudicated by board certified cardiologists, with considerable time of follow-up post-surgery and a novel but validated statistical method to model longitudinal binary outcome was used to report the time-varying change in risk of POAF.
This single center, observational study validates the risk for POAF in a cohort undergoing cardiac valve surgery, either alone or in combination with other surgical procedures. In addition, it adds incremental information on the time-varying nature of POAF, emphasizing the increasing risk of AF with the passage of time after the initial reduction in POAF risk, along with associated risk factors. Patients with these risk factors could be targeted for longer follow-up. Randomized controlled trials are needed to establish superiority of longer follow-up compared to routine post-operative follow up before widespread acceptance. In addition, cost-effectiveness, frequency and duration of long-term monitoring was not addressed in this study and are questions for future research, especially in the current era of value-based practice.
- Boriani G, Fauchier L, Aguinaga L, Beattie JM, Blomstrom Lundqvist C, Cohen A, Dan G-A, Genovesi S, Israel C, Joung B, Kalarus Z, Lampert R, Malavasi VL, Mansourati J, Mont L, Potpara T, Thornton A, Lip GYH and Group ESCSD. European Heart Rhythm Association (EHRA) consensus document on management of arrhythmias and cardiac electronic devices in the critically ill and post-surgery patient, endorsed by Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), Cardiac Arrhythmia Society of Southern Africa (CASSA), and Latin American Heart Rhythm Society (LAHRS). EP Europace. 2018:euy110-euy110.
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM and Yancy CW. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation. Journal of the American College of Cardiology. 2014;64:e1.
- Maesen B, Nijs J, Maessen J, Allessie M and Schotten U. Post-operative atrial fibrillation: a maze of mechanisms. Europace. 2012;14:159-174.
- Mathew JP, Fontes ML, Tudor IC and et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA. 2004;291:1720-1729.
- Mahoney EM, Thompson TD, Veledar E, Williams J and Weintraub WS. Cost-effectiveness of targeting patients undergoing cardiac surgery for therapy with intravenous amiodarone to prevent atrial fibrillation. Journal of the American College of Cardiology. 2002;40:737-45.
- Villareal RP, Hariharan R, Liu BC, Kar B, Lee VV, Elayda M, Lopez JA, Rasekh A, Wilson JM and Massumi A. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. Journal of the American College of Cardiology. 2004;43:742-8.
- Shen J, Lall S, Zheng V, Buckley P, Damiano RJ, Jr. and Schuessler RB. The persistent problem of new-onset postoperative atrial fibrillation: a single-institution experience over two decades. The Journal of thoracic and cardiovascular surgery. 2011;141:559-70.
- Mariscalco G and Engstrom KG. Postoperative atrial fibrillation is associated with late mortality after coronary surgery, but not after valvular surgery. The Annals of thoracic surgery. 2009;88:1871-6.
- Ahlsson A, Fengsrud E, Bodin L and Englund A. Postoperative atrial fibrillation in patients undergoing aortocoronary bypass surgery carries an eightfold risk of future atrial fibrillation and a doubled cardiovascular mortality. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2010;37:1353-9.
- Frendl G, Sodickson AC, Chung MK, Waldo AL, Gersh BJ, Tisdale JE, Calkins H, Aranki S, Kaneko T, Cassivi S, Smith SC, Jr., Darbar D, Wee JO, Waddell TK, Amar D and Adler D. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. The Journal of thoracic and cardiovascular surgery. 2014;148:e153-93.
- Rajeswaran J, Blackstone EH, Ehrlinger J, Li L, Ishwaran H and Parides MK. Probability of atrial fibrillation after ablation: Using a parametric nonlinear temporal decomposition mixed effects model. Statistical methods in medical research. 2016.
- Blackstone EH. Breaking down barriers: helpful breakthrough statistical methods you need to understand better. The Journal of thoracic and cardiovascular surgery. 2001;122:430-9.
- Diggle PJ HP, Liang KY, Zeger SL. Analysis of longitudanal data New York: Oxford University Press; 2002(2nd edition).
- Efron B TR. An introduction to the Bootstrap method New York: Chapman and Hall/ CRC; 1998.
- Melby SJ, George JF, Picone DJ, Wallace JP, Davies JE, George DJ and Kirklin JK. A time-related parametric risk factor analysis for postoperative atrial fibrillation after heart surgery. The Journal of thoracic and cardiovascular surgery. 2015;149:886-92.
- Park YM, Cha MS, Park CH, Choi CH, Jeon YB, Kang WC, Choi IS and Park KY. Newly developed post-operative atrial fibrillation is associated with an increased risk of late recurrence of atrial fibrillation in patients who underwent open heart surgery: Long-term follow up. Cardiology journal. 2017.
- Lee SH, Kang DR, Uhm JS, Shim J, Sung JH, Kim JY, Pak HN, Lee MH and Joung B. New-onset atrial fibrillation predicts long-term newly developed atrial fibrillation after coronary artery bypass graft. American heart journal. 2014;167:593-600.e1.
- Melduni RM, Schaff HV, Bailey KR, Cha SS, Ammash NM, Seward JB and Gersh BJ. Implications of new-onset atrial fibrillation after cardiac surgery on long-term prognosis: a community-based study. American heart journal. 2015;170:659-68.






