Atrial fibrillation (AF) frequently progresses from paroxysmal to persistent AF (persAF). Unlike paroxysmal AF ablation, an optimal ablation strategy for persAF beyond pulmonary vein isolation (PVI) is unclear; long-term success rates remain low, and success varies depending upon the technique employed [1,2].
In patients with paroxysmal AF, use of a contact force (CF)-sensing catheter improves the success of catheter ablation compared to a traditional non–CF-sensing catheter (74%-96% vs. 64.1%-82%, respectively) [3-8]. However, limited data exist on long-term success rates in patients with persAF treated with CF-sensing catheters [1]. Based on the Heart Rhythm Society (HRS)/European Heart Rhythm Association (EHRA)/European Cardiac Arrhythmia Society (ECAS) recommendations, the minimum chronic acceptable success rate (objective effectiveness endpoint for a clinical trial) for persAF at the 12-month follow-up is 40% [9].
Although consensus is lacking regarding the preferred treatment strategy for persAF, improving the safety and quality of lesions by using a CF-sensing catheter may improve outcomes. This observational registry evaluated the real-world safety and 12-month success rate of catheter ablation in drug-refractory persAF ablation using an open-irrigated, CF-sensing catheter.
The THERMOCOOL SMARTTOUCH® registry, a prospective, open-label, multicenter, observational registry, was designed to evaluate the real-world safety and long-term success of persAF ablation using an open-irrigated, CF-sensing catheter (THERMOCOOL SMARTTOUCH® Catheter; Biosense Webster, Inc., Diamond Bar, California). Data were collected between August 30, 2012, and June 28, 2014, at 24 centers in Europe, Australia, and Canada. An institutional review board and/or ethics committee approved the study at each participating center. The study was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Harmonised Tripartite Guidelines for Good Clinical Practice. All patients provided written informed consent to the study protocol.
Data were included for all persAF patients enrolled in the registry who were ≥18 years of age and had failed at least 1 anti-arrhythmic drug (class I or class III/atrioventricular nodal blocker). Prior AF ablations were permitted. PersAF was defined in accordance with the HRS/EHRA/ECAS expert consensus statement as continuous AF that is sustained beyond 7 days [9]. Episodes of AF requiring electrical or pharmacological cardioversion after ≥48 hours of AF, but prior to 7 days, were also considered as persAF episodes. Continuous AF was further defined as AF that is documented to be present on all electrocardiogram (ECG) monitoring performed during a defined period of time [9]. Data from patients with long-standing persAF (continuous AF for >12 months duration) [9] were excluded. Patient exclusion criteria included AF secondary to electrolyte imbalance, thyroid disease, or reversible or non-cardiac causes; atrial myxoma, intramural thrombus, tumor, or other abnormalities preventing catheter use; unstable angina; congenital or medical abnormalities or any other disease preventing ablation; New York Heart Association functional class III or IV or uncontrolled heart failure; an implanted cardioverter-defibrillator; prior coronary artery bypass graft or other cardiac or valvular surgery or awaiting such procedures within 12 months; severe pulmonary disease; contraindication to anti-coagulation medications; a documented thromboembolic event in the previous 12 months; or life expectancy of <12 months.
The ablation catheter has been described in detail elsewhere [10,11]. Briefly, the 7.5-Fr THERMOCOOL SMARTTOUCH® CF-sensing catheter has a 3.5-mm electrode tip and 6 open-irrigation holes. Before ablation, transthoracic echocardiogram, cardiac imaging, or both were performed as warranted for detection of thrombus per each institution’s standard practice. PVI with confirmation of entrance block was verified for all targets [9], and pulmonary veins (PVs) were isolated as needed. Before ablation, 3-dimensional electro-anatomical mapping was performed using the CARTO® 3 system (Biosense Webster, Inc., Diamond Bar, California). The irrigation flow rate varied with radiofrequency (RF) power setting (recommended settings: 17 mL/minute for ≤30 W; 30 mL/minute for 31-50 W).
The investigator could perform additional ablation of non-PV targets such as left atrial (LA) linear lesions (e.g., left inferior PV-mitral annulus [LIPV-MA] and cavotricuspid isthmus), sites with complex fractionated atrial electrograms (CFAEs), superior vena cava isolation, and other AF focal lesions, as deemed necessary. Post-ablation isoproterenol infusion (≤20 μg/minute) or intravenous adenosine administration (6- to 12-mg bolus) was recommended to detect PV reconnection or confirm elimination of all AF foci. Operators were encouraged to check for bidirectional block after linear lesion delivery as per the institution's current best practices. Investigators were allowed to perform repeat ablations, as well as continue a previously ineffective drug at the same or lower dose during the effectiveness evaluation period.
Anti-coagulation was recommended 30 days before ablation, and an activated clotting time of 300-400 seconds was recommended during ablation. Anti-coagulation was recommended for the first 3 months after ablation and subsequently during the effectiveness evaluation period according to current guidelines [12].
A CF working range was pre-selected by each investigator based on experience. CF data points were sampled and stored every 50 milliseconds during RF application, translating into ≥90,000 data points per case. Each data point was analyzed to determine whether or not it was within the pre-specified working range for each case. The distribution of average CF per ablation was calculated across the collected data points. Thereafter, the percentage of time that the investigator was within the pre-selected CF working range was calculated by the number of data points within the working range/total data points × 100.
Effectiveness and Procedural Outcomes
Patients were followed-up by telephone at 3, 6, and 12 months after index ablation. Acute success was defined as confirmation of entrance block for all targeted PVs. Long-term (12 months) success was defined as patient-reported freedom from symptomatic AF assessed at each follow-up time point. Other assessments included total fluoroscopy time, fluoroscopy dose, total procedure time, RF application time, CF during ablation, and correlation of long-term success with CF. Quality of life (QoL) improvements were assessed at 6 and 12 months using the validated 20-item Atrial Fibrillation Effect on QualiTy-of-life (AFEQT) questionnaire, which contains 4 conceptual domains (symptoms, daily activities, treatment concern, and treatment satisfaction) from which global and individual domain scores are calculated [13].
Primary adverse events (AEs) were defined as the incidence of early-onset (≤7 days of the index procedure) procedure- or device-related serious AEs such as directly related death; atrioesophageal fistula; atrial perforation/pericardial effusion; cardiac tamponade; myocardial infarction; stroke/cerebrovascular accident; thromboembolism; transient ischemic attack; diaphragmatic paralysis; pneumothorax; heart block; PV stenosis or pulmonary edema; respiratory insufficiency; pericarditis; vascular access complication, including symptomatic PV stenosis (≥70% reduction in PV diameter from baseline computed tomography/magnetic resonance angiography scan or PV gradient >10 mm Hg on post-procedure echocardiography); and atrioesophageal fistulas (including those that occurred >7 days after the procedure). All AEs were adjudicated by an independent Clinical Events Adjudication Committee and were monitored until they were resolved.
The safety cohort comprised all patients who underwent insertion of the registry catheter, and the evaluable cohort comprised all patients who met eligibility criteria and underwent ablation with the THERMOCOOL SMARTTOUCH® catheter in compliance with the study protocol. Analysis of procedural data, effectiveness endpoints, and QoL was based on the evaluable cohort. The number and percentage of patients with confirmed entrance block for all targeted PVs, freedom from symptomatic AF recurrence (patient-reported), and procedural or peri-procedural AEs were summarized with corresponding 2-sided 95% exact binomial confidence intervals (CIs). Probability of freedom from patient-reported symptomatic AF recurrence through the 12-month follow-up in the evaluable cohort, as well as in patients with and without prior ablation and those with and without post-ablation isoproterenol/adenosine challenge, was determined using Kaplan-Meier estimates. Distributions of average CF and percentage of time with CF measurements within pre-selected ranges were plotted. Descriptive statistics and logistic regression models were used to assess the correlation of long-term success with average CF, percentage of time CF measurements were within the working range pre selected by the investigator, and percentage of time CF measurements were within the pre selected range dichotomized at a value of 80%. Change in QoL from baseline to each follow up visit, based on overall AFEQT and sub-scale measures, was assessed using the 1 sample Student’s t test. Logistic regression models were used to identify predictors of 12 month success. Covariates that were significant at P values <0.10 in the univariate regression analysis were entered into the multivariate regression analysis. Only those covariates that remained significant at P values <0.10 were included in the final multivariate regression model. The statistical significance level was set at 0.05 for 2-sided tests. All statistical analyses were performed using SAS software version 9.3 (SAS Institute Inc., Cary, North Carolina).
A total of 150 patients with persAF were enrolled in the registry: 150 patients who had the study catheter inserted comprised the safety cohort, and 142 patients who met the inclusion/exclusion criteria and underwent ablation using the study catheter in compliance with the study protocol comprised the evaluable cohort [Figure 1]. Baseline demographics and patient characteristics were similar between the safety and evaluable cohorts: mean ± standard deviation (SD) age was 61.6 ± 9.4 and 61.6 ± 9.6 years, respectively, and most patients were male (76.0% and 75.4%, respectively) and Caucasian (90.7% and 90.8%, respectively; [Table 1]).
Figure 1. Patient enrollment I/E, inclusion/exclusion; RF, radiofrequency
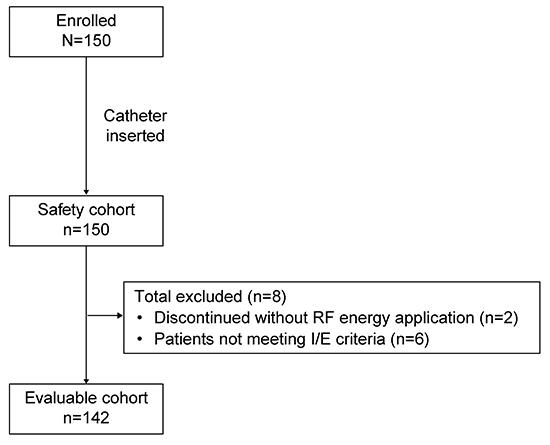
Table 1. Patient demographics and baseline characteristics
| Variable |
Safety cohort
(n=150)
|
Evaluable cohort
(n=142)
|
| Agea years |
| Mean ± SD, n |
61.6 ± 9.4 |
61.6 ± 9.6 |
| Median |
62.0 |
62.0 |
| Min/max |
36.0/80.0 |
36.0/80.0 |
| Sex, n (%) |
| Male |
114 (76.0) |
107 (75.4) |
| Female |
36 (24.0) |
35 (24.6) |
| Child-bearing potential |
1/36 (2.8) |
1/35 (2.9) |
| Not of child-bearing potential |
35/36 (97.2) |
34/35 (97.1) |
| Race, n (%) |
| Black or African American |
1 (0.7) |
1 (0.7) |
| White or Caucasian |
136 (90.7) |
129 (90.8) |
| NA |
13 (8.7) |
12 (8.5) |
| Patient history, n (%) |
| AF duration, mean ± SD, years |
4.6 ± 4.76 |
4.6 ± 4.78 |
| Atrial flutter |
42 (28.0) |
41 (28.9) |
| Hypertension |
82 (54.7) |
76 (53.5) |
| Diabetes |
18 (12.0) |
18 (12.7) |
| Structural heart disease |
34 (22.7) |
33 (23.2) |
| Prior thromboembolic events |
12 (8.0) |
11 (7.7) |
| NYHA class, n (%) |
| None |
70 (46.7) |
65 (45.8) |
| I |
34 (22.7) |
34 (23.9) |
| II |
45 (30.0) |
43 (30.3) |
| Unknown |
1 (0.7) |
0 (0.0) |
| Patients who had at least 1 previous AF ablation, n (%) |
36 (24%) |
33 (23.2) |
| Failed anti-arrhythmic drug class, n (%) |
| I/III at baseline |
117 (78.0) |
114 (80.3) |
| II/IV only |
26 (17.3) |
25 (17.6) |
| Baseline anti-arrhythmic medications, n (%) |
| I/III, using at baseline |
129 (86.0) |
124 (87.3) |
| II/IV, using at baseline |
74 (49.3) |
72 (50.7) |
| LVEF, %, mean ± SD, min/max |
56.9 ± 10.3b, 30.0/72.0 |
56.5 ± 10.7c,
30.0/72.0
|
| LA dimension, mm, mean ± SD, min/max |
41.5 ± 7.9d,
26.0/60.0
|
42.0 ± 8.2e,
26.0/60.0
|
Values are n (%) unless specified otherwise AF, atrial fibrillation; LA, left atrial; LVEF, left ventricular ejection fraction; NA, not available (from France and Monaco); NYHA, New York Heart Association; SD, standard deviation aAge at time of informed consent; bn=29; cn=26; dn=27; en=24
Primary AEs occurred in 4% of patients (6/150; 95% CI: 1.5-8.5): atrioesophageal fistula (1), cardiac perforation (1), stroke (1), arteriovenous fistula (1), vessel puncture site hematoma (1), and vascular pseudoaneurysm (1; [Table 2]). The atrioesophageal fistula case resulted in death 1 month after the index ablation procedure and was considered procedure related and possibly device related. After discharge, this patient presented to a different institution with pulmonary symptoms and was diagnosed with an atrioesophageal fistula. The patient’s ablation procedure, which involved PVI with additional ablation of non-PV targets, was performed under general anesthesia without the use of esophageal probe or esophageal pre-imaging by an investigator who had previous experience with the study catheter. The patient had no significant comorbidities, and ablation parameters were within normal limits (average [min max] CF: 12 g [4-27 g]; the majority of ablation points were below 20 g of CF; average power: 19 W; highest infusion rate: 17 mL/minute; and average electrode temperature: 39°C). The case of cardiac perforation occurred at the time of mapping, and no RF energy was delivered. Other than the atrioesophageal fistula case, all other AEs were considered non–device-related and resolved without sequelae at follow-up.
Table 2. Primary adverse events
| System organ class/
preferred term
|
Patients,
n/N (%)
|
Events, n |
Device relatedness |
Procedure relatedness |
| Cardiac perforation |
1/150 (0.7) |
1 |
No |
Yes |
| Atrioesophageal fistula |
1/150 (0.7) |
1 |
Possibly |
Yes |
| Stroke |
1/150 (0.7) |
1 |
No |
Possibly |
| Vascular access complication |
| Arteriovenous fistula |
1/150 (0.7) |
1 |
No |
Yes |
| Vessel puncture site hematoma |
1/150 (0.7) |
1 |
No |
Yes |
| Vascular pseudoaneurysm |
1/150 (0.7) |
1 |
No |
Yes |
Acute Success and Procedural Outcomes
PVs were targeted in 141/142 (99.3%) ablation procedures. Acute success with confirmation of entrance block for all targeted PVs was achieved in 99.3% of patients (141/142; 95% CI: 96.1% 100.0%). Non-PV targets comprised LA linear lesions in 72 (50.7%) patients, including LIPV-MA in 23 (16.2%) patients and cavotricuspid isthmus in 31 (21.8%) patients. Other targets included sites with CFAEs in 26 (18.3%) patients and other AF foci in 13 (9.2%) patients. The mean (SD; n) fluoroscopy time and dose were 24.5 (20.7; 138) minutes and 1.8 (3.1; 73) Grays, respectively. The mean (SD; n) total procedure and RF application times were 171.3 (64.0; 138) and 42.8 (22.8; 132) minutes, respectively.
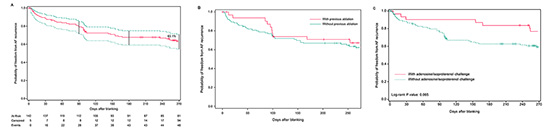
By Kaplan-Meier analysis, freedom from symptomatic AF at 12 months after the index ablation procedure was 63.1% (82/130; 95% CI: 54.2%-71.4%) with a mean of 1.03 ablations [Figure 2A]. Success rates did not differ between patients with or without prior AF ablation (P=0.557; [Figure 2B]). A non-significant trend towards a higher success rate was observed in patients who received an isoproterenol/adenosine challenge at the end of the ablation procedure (73.1% [95% CI: 0.55%-0.85%] vs. 60.2% [95% CI: 0.50%-0.69%], respectively; P=0.065; [Figure 2C]).
Figure 2. Kaplan-Meier analysis of 12-month success; freedom from symptomatic AF in (A) evaluable cohort (n=142), (B) evaluable cohort stratified as patients with or without prior AF ablation, and (C) evaluable cohort stratified as patients with or without a post-ablation isoproterenol/adenosine challenge AF, atrial fibrillation
CF and its Correlation With 12-Month Success
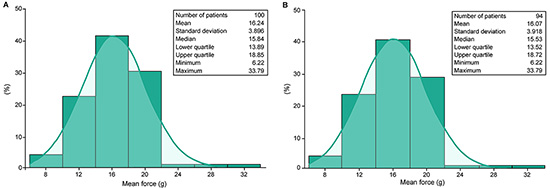
The mean (SD) CF recorded during the index ablation procedures was 16.2 (4.0) g in the safety cohort and 16.1 (4.0) g in the evaluable cohort [Figure 3]. When dichotomized at a mean CF of 16 g, a non-significant trend of correlation was observed between higher average CF and 12 month effectiveness (odds ratio [OR]: 1.12; 95% CI: 0.99-1.27; P=0.08).
Figure 3. Distribution of average CF per ablation procedure by continuous variable analysis in (A) safety cohort (n=150) and (B) evaluable cohort (n=142) CF, contact force
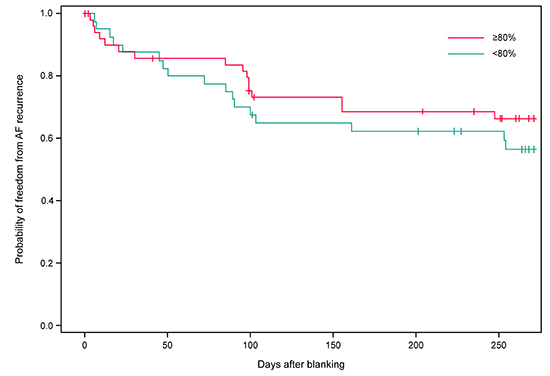
For the index ablation procedures in which CF data were available in the evaluable cohort, the majority of the CF working ranges pre-selected by the investigators were set between a low of 5 g and a high of 40 g (71.8% [61/85] between 5 and 40 g; 18.8% [16/85] between 10 and 40 g). Investigators remained within their pre-selected CF working ranges for a mean (SD) of 79.7% (12.7%) of the time in the evaluable cohort. Sub-group analysis (dichotomized at the mean) showed that long-term success tended to increase when investigators remained within their pre selected CF working range ≥80% vs. <80% of the time; however, this difference did not reach statistical significance (69.2% vs. 58.5%, respectively; P=0.285; [Figure 4]).
Figure 4. Kaplan-Meier estimates for time to first AF recurrence through 12 months stratified at 80% (investigators working in their pre-selected CF ranges ≥80% vs. <80% of the time) (evaluable cohort, n=142) AF, atrial fibrillation; CF, contact force
Predictors of 12-Month Success
Multivariate logistic regression analysis of factors for 12-month effectiveness outcomes showed that male gender and isoproterenol/adenosine challenge after ablation were associated positively with the odds of 12-month success, with the association being statistically significant for the latter (OR: 2.84; 95% CI: 1.05-7.67). The presence of prior thromboembolic events and pre existing congestive heart failure trended towards a negative association with 12-month success [Table 3].
Table 3. Potential risk factors for 12-month success (evaluable cohort, n=142)
|
|
Univariate analysis |
|
|
Multivariate analysis |
|
| Factors |
n |
OR (95% CI) |
P value |
n |
OR (95% CI) |
P value |
| Age |
130 |
0.98 (0.94 1.01) |
0.202 |
| Male vs. female |
130 |
2.03 (0.89 4.65) |
0.094 |
130 |
2.26 (0.936 5.446) |
0.070 |
| Isoproterenol/adenosine challenge |
130 |
2.42 (0.95 6.16) |
0.063 |
130 |
2.84 (1.049 7.671) |
0.040 |
| Total fluoroscopy dose, Grays |
66 |
1.01 (0.84 1.21) |
0.952 |
| Total fluoroscopy time, minutes |
126 |
0.99 (0.97 1.01) |
0.166 |
| Highest infusion rate, mL/minute |
97 |
1.01 (0.97 1.05) |
0.734 |
| Total procedure time, minutes |
126 |
1.00 (0.99 1.01) |
0.997 |
| Longest power duration, seconds |
89 |
1.00 (1.00 1.00) |
0.268 |
| Number of RF applications |
115 |
1.00 (0.99 1.01) |
0.912 |
| Total RF application time, minutes |
121 |
1.00 (0.99 1.02) |
0.811 |
| Any thromboembolic event |
130 |
0.27 (0.06 1.12) |
0.071 |
130 |
0.22 (0.048 1.047) |
0.057 |
| Percentage of CF in range >80% |
85 |
1.45 (0.60 3.48) |
0.407 |
| Mean distal temperature, °C |
86 |
0.89 (0.74 1.08) |
0.226 |
| Mean CF, g |
86 |
1.08 (0.96 1.23) |
0.199 |
| Mean impedance, Ω |
86 |
1.02 (1.00 1.04) |
0.114 |
| Time of lateral inaccuracy, % |
86 |
1.00 (0.93 1.07) |
0.920 |
| Time of force metal severity: 2 or above, % |
86 |
1.00 (0.97 1.03) |
0.910 |
| AF episode in past 12 months |
129 |
0.98 (0.36 2.69) |
0.971 |
| Duration of AF, years |
129 |
0.97 (0.90 1.04) |
0.399 |
| History of congestive heart failure |
130 |
0.34 (0.11 1.03) |
0.057 |
130 |
0.37 (0.116 1.152) |
0.086 |
| History of hypertension |
129 |
0.88 (0.43 1.80) |
0.727 |
| History of ischemic cardiomyopathy |
130 |
1.18 (0.21 6.69) |
0.852 |
| History of non-ischemic dilated cardiomyopathy |
129 |
0.27 (0.05 1.53) |
0.138 |
| History of significant valve disease |
130 |
0.58 (0.04 9.49) |
0.703 |
| History of diabetes |
130 |
0.81 (0.29 2.30) |
0.697 |
| History of transient ischemic attacks |
130 |
0.19 (0.02 1.83) |
0.149 |
| History of pulmonary embolus |
129 |
1.19 (0.11 13.48) |
0.888 |
| History of atrial flutter |
130 |
1.74 (0.77 3.93) |
0.180 |
| History of atrial tachycardia (LAT and RAT) |
130 |
1.18 (0.21 6.69) |
0.852 |
| History of AV node re-entry tachycardia |
130 |
1.17 (0.10 13.31) |
0.896 |
| History of ventricular tachycardia |
130 |
0.28 (0.05 1.56) |
0.145 |
| History of ventricular fibrillation |
130 |
0.19 (0.02 1.83) |
0.149 |
| History of left ventricular hypertrophy |
130 |
1.03 (0.28 3.71) |
0.968 |
| Mean power, W |
86 |
0.96 (0.86 1.07) |
0.481 |
| LA diameter parasternal long axis view |
21 |
0.93 (0.82 1.05) |
0.262 |
| LVEF (%) |
23 |
1.04 (0.96 1.12) |
0.367 |
AF, atrial fibrillation; AV, atrioventricular; CF, contact force; CI, confidence interval; LA, left atrial; LAT, left atrial tachycardia; LVEF, left ventricular ejection fraction; OR, odds ratio; RAT, right atrial tachycardia; RF, radiofrequency; W, watts
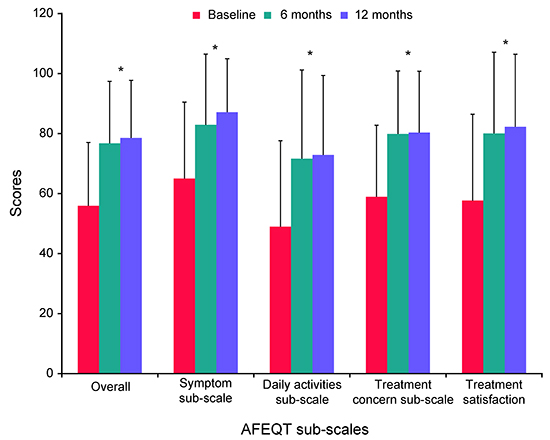
Patients’ QoL improved significantly overall and on all sub-scales of the AFEQT questionnaire (P<0.0001) at 6 months; these improvements were sustained through the 12-month follow-up [Figure 5].
Figure 5. Quality of life based on the AFEQT questionnaire (evaluable cohort, n=142) *P˂0.0001 compared with baseline AFEQT, Atrial Fibrillation Effect on QualiTy-of-life
Results from this prospective, multicenter registry demonstrate the real-world experience of persAF ablation with the THERMOCOOL SMARTTOUCH® catheter with a 12-month success rate of 63.1% and significant improvements in patients’ QoL. Success rates did not differ between patients with and without prior AF ablation, but increased substantially to 73.1% in patients who received an isoproterenol/adenosine challenge after ablation (73.1% vs. 60.2%; P=0.065). Of note, the reported success rates were with a mean of 1.03 ablations per patient suggesting that these observations mimicked/were similar to a single procedure setting. Overall, 6 of the 150 patients who underwent catheter insertion experienced a primary AE, resulting in an AE rate of 4%. Three of these 6 AEs were vascular access complications, which could have been avoided by performing ultrasound-guided puncture.
We identified weak associations between CF and clinical outcomes. An increase in the percentage of time (≥80%) within the CF working range pre-selected by the investigator, which is indicative of catheter-tissue stability, was associated with significant improvement in long term success in the paroxysmal AF population [6], whereas a non-significant trend was observed in the present study involving patients with persAF. Additionally, a non-significant trend of correlation was observed between higher average CF dichotomized at 16 g and 12 month effectiveness. We did not perform any correlation analysis of CF with safety, as the event rate was too low and would preclude any clinically meaningful conclusions. The lack of any strong findings of correlation between CF parameters examined and clinical outcomes suggests that factors in addition to CF, such as optimal ablation strategy and patient selection, may be important to consider in persAF ablation.
Unlike paroxysmal AF ablation where PVI has long been considered the cornerstone of ablation strategy, variations in ablation strategies exist, and much is unknown or debatable with regard to what is considered the optimal treatment strategy in persAF ablation [1,2]. In the STAR AF II trial, no differences in clinical outcomes were observed between persAF ablation groups who received PVI only and those who received additional linear ablation or CFAE ablation [1]. A meta-analysis of persAF ablation, however, suggested that additional linear ablation, but not CFAE ablation, within the left atrium may result in reduction of AF recurrence [14]. In addition, atrial fibrosis was associated with a likelihood of recurrent arrhythmia [15], and box isolation of fibrotic areas in a sub-group of non-paroxysmal AF patients with identified low-voltage areas resulted in a long-term (12-month) success rate of 72% [16]. Taken together, a tailored ablation strategy based on appropriate patient selection and the extent of cardiac disease presentation appears to be a logical approach. In our registry, approximately half of the ablation procedures included additional LA linear ablations, and a small number of procedures included other ablation targets such as CFAE and other AF foci. The contribution of these additional ablation targets to the overall success rate needs to be examined further, especially in an era in which operators can now be more certain of creating lesions with the advent of CF-sensing catheters and CF stability algorithms.
Comparison of our observed 12-month success rates with those of other studies is difficult due to differences in ablation strategies employed and definitions of endpoints. Nonetheless, the overall success rate reported from this registry is, for the most part, similar to or slightly better than previously reported outcomes in other persAF studies using non–CF-sensing catheters [1,17,18]. Together with the observed non-significant trend of CF stability towards improved effectiveness outcome, the data suggest a role of the real-time CF-sensing catheter in persAF ablation.
This registry was conducted when the CF-sensing catheter was newly available and, therefore, the investigators’ use of CF technology represents that of early experience. At the time of enrollment, workflow was less defined, and CF stability was less understood and may not have been achieved in some cases. The importance of CF stability in ablation outcomes is supported by a recent sub-analysis of the SMART-AF trial showing that adequate and stable CF correlates with optimal long-term success in paroxysmal AF ablation [19]. It is conceivable that with more experience and proper use of CF, the weak CF trend observed in the current registry may be amplified. Also, the use of CF in linear ablation strategies makes intuitive sense if the underlying hypothesis of benefit from additional linear lesions holds true. While conflicting data exist in the percutaneous ablation space [1,2], the outcomes of surgical intervention for persAF are more encouraging, and it is at least theoretically possible that improved tools will improve outcomes for percutaneous linear ablation strategies [20]. The combination of CF technology and a tailored ablation strategy based on patient selection or cardiac disease presentation might therefore result in better treatment success for persAF ablation. This hypothesis needs to be evaluated in future studies.
An interesting observation from this registry is the improved odds of success at 12 months in patients who received an isoproterenol/adenosine challenge immediately after ablation to uncover dormant conduction (OR: 2.84; 95% CI: 1.05-7.67), suggesting that complete PVI and/or AF non-inducibility is important to achieve optimal success. This is consistent with a previous meta-analysis of persAF ablation showing that PVI is important in improving success rates [14].
Atrioesophageal fistula is a known, but rare and potentially devastating, complication of AF ablation. In the present study, an unfortunate fatal atrioesophageal fistula case was reported. Although the CF and ablation parameters used in this patient were within normal ranges, the event further emphasizes the need to exercise strong caution when creating lesions involving ablation on the posterior LA wall, especially in close proximity to the esophagus. Esophageal visualization or luminal temperature monitoring may be helpful to minimize the occurrence of esophageal injury, which was not used in this case. In addition, the biophysical benefits of using a catheter with stable CF and its impact on lesion creation and energy delivery while performing a PVI cannot be overlooked [21]. Also, PVI alone is insufficient for treatment of persistent AF. This is again borne out of the fact that there is a trend to better outcomes when vein isolation via isoprenaline/adenosine is checked suggesting that additional ablation may be needed in this patient population [22,23].
Some limitations need to be considered when interpreting the results of this study. Firstly, the study lacked a control group. Also, the long-term success of ablation was patient-reported, and documentation by ECG and trans-telephonic monitoring were not mandated. Data regarding persistent AF ablation using CF-sensing catheters with a modest sample size are limited; therefore, correlations observed in this study do not imply causative mechanisms as the dataset was not designed for formal hypothesis testing. Information on achievement of bidirectional block was not recorded in the database. No restrictions were placed on the ablation technique, potentially affecting outcomes; however, this scenario reflects real-world clinical practice. Furthermore, patients with long-standing persAF and those with advanced heart failure were excluded from enrollment in the registry; therefore, the results may not be generalizable to these patient populations.
This study was sponsored by Biosense Webster, Inc.
Tom De Potter, Hugo Van Herendael, Richard Balasubramaniam, Decebal-Gabriel Laţcu, Sharad C. Agarwal, and Antonio Pani have no conflicts of interest to declare.
Matthew Wright has received support for travel to meetings for the study or other purposes from Biosense Webster, Inc. Baohui Zhang and Lee Ming Boo hold stocks and are employees of Johnson & Johnson Pharmaceuticals. The results have been presented in part as a poster in CARDIOSTIM EHRA EUROPACE, June 08-11, 2016, Nice, France.
We wish to express our appreciation to all the trial investigators (Supplementary Table S1). The authors wish to thank the following individuals for their contribution to the study conduct, statistical analysis, and editorial assistance with the manuscript: Carmen Rousseeuw, Nathalie Macours, Tiffany Tan, and Robert Stagg. Additional editorial support, in the form of assembling tables and creating high-resolution images based on authors’ detailed directions, collating authors’ comments, copyediting, and referencing, was provided by Cactus Communications, and funded by Biosense Webster, Inc. The manuscript content was developed by the authors; the authors retained full control of all content and revisions during its preparation. The data were provided by the sponsor company, with the authors having full access to all data collected during the execution of the study protocol.
Tom De Potter and Matthew Wright have contributed towards conception/design, acquisition/analysis/interpretation of data, drafting the article, and critical revision of the article. Hugo Van Herendael has contributed towards acquisition/interpretation of data and critical revision of the article. Richard Balasubramaniam has contributed towards conception/design, acquisition of data, and critical revision of the article. Decebal-Gabriel Laţcu, Sharad C. Agarwal, and Antonio Pani have contributed towards acquisition of data and critical revision of the article. Lee Ming Boo has contributed towards data analysis/interpretation, drafting the article, and critical revision of the article. Baohui Zhang has contributed towards conception/design, data analysis/interpretation, statistical analysis, and critical revision of the article. All authors have approved the manuscript and are accountable for all aspects of the work.






