Prevalence and Characteristics of Venous Thrombosis after Catheter Ablation of Atrial Fibrillation in Patients Receiving Periprocedural Direct Oral Anticoagulants
Takehito Sasaki1, Kohki Nakamura1, Kentaro Minami1, Yutaka Take1, Keiko Koyama2, Eiji Yamashita1, Shigeto Naito1
1
Division of Cardiology, Gunma Prefectural Cardiovascular Center, 3-12 Kameizumi-machi, Maebashi City, Gunma 371-0004, Japan.2
Division of Radiology, Gunma Prefectural Cardiovascular Center, 3-12 Kameizumi-machi, Maebashi City, Gunma 371-0004, Japan.
Periprocedural venous thromboembolisms (VTEs) area rare occurrence but a critical complication after catheter ablation of atrial fibrillation (AF).The aim of this study was to investigate the incidence of symptomatic deep vein thromboses (DVTs) and pulmonary thromboembolisms (PTEs) in patients who underwent AF catheter ablation and received periprocedural oral anticoagulation with direct oral anticoagulants (DOACs).
A total of 2,193 consecutive patients undergoing AF catheter ablation with periprocedural DOACs were retrospectively analyzed.Two patients (0.091%) experienced symptomatic DVTs after the ablation, and no patients had any PTEs. One patient was a 72-year-old female who underwent cryoballoon ablation with periprocedural apixaban at a dose of 2.5 mg twice daily. The other patient was a 74-year-old male who underwent a Hot Balloon ablation and thereafter radiofrequency catheter ablation for recurrent AF with edoxaban at30 mg once daily. Both DVT patients underwent AF ablation by the right femoral vein approach, and after discharge had right leg pain and swelling on post-procedural days 4 and 8, respectively. TheDVT was treated by increasing the dose of apixaban and changing it from 30 mg/day of edoxaban to 15-30 mg/day of rivaroxaban, and the thrombi completely disappeared in both patients without any thromboembolic and hemorrhagic complications.
AF catheter ablation with periprocedural DOAC treatment revealed anextremely low incidence of symptomatic VTEs, which may be successfully treated by increasing the DOAC dose or changing the DOAC type.
Key Words : Atrial Fibrillation, Catheter Ablation, Deep Vein Thrombosis, Direct Oral Anticoagulant..
Correspondence to: Kohki Nakamura
Division of Cardiology, Gunma Prefectural Cardiovascular Center, 3-12 Kameizumi-machi, Maebashi City, Gunma 371-0004, Japan
Percutaneous catheter ablation has become an important therapeutic option for treating patients with atrial fibrillation (AF)[1].AF catheter ablation generally requires multiple sheaths inserted into a single femoral vein in order to introduce ablation and mapping catheters into the atria, and has a potential risk for the occurrence of venous thromboembolisms (VTEs) after the ablation. Periprocedural VTEs are a rare occurrence but a critical complication of AF ablation[2].
Adequate periprocedural anticoagulation using oral anticoagulants plays an important role in preventing thromboembolic complications associated with AF ablation[3,4]. Direct oral anticoagulants (DOACs) have been widely used for periprocedural anticoagulation management in AF ablation[5,6]. So far limited data are available on the incidence of VTEs after AF ablation among patients receiving periprocedural anticoagulation with DOACs. The present study aimed to investigate the incidence of symptomatic deep vein thromboses (DVTs) and pulmonary thromboembolisms(PTEs)among patients who underwent catheter ablation of AF and received periprocedural DOAC treatment.
We took advantage of the differential flow rates between these otherwise similar designed ACs to evaluate the measurable biochemical and clinical impact of the saline volume infused through the ACs in PAF patients during their RFA procedure in the immediate post operative period of up to 1 month.
This retrospective observational study enrolled consecutive AF patients who received periprocedural oral anticoagulation with DOACs prior to AF catheter ablation at Gunma Prefectural Cardiovascular Center betweenApril 2011 and April 2018. All patients underwent transthoracic echocardiography to evaluate the atrial and ventricular sizes and left ventricular function using standard parasternal and apical views before the procedure, and transesophageal echocardiography to rule out any intracardiac thrombi on the day of the procedure or the day before. Written informed consent for the electrophysiological study and catheter ablation of AF was obtained from all patients.
Periprocedural Anticoagulation
Periprocedural oral anticoagulation was performed with the standard or reduced DOAC dosage approved in Japan: dabigatran at a dose of 110 or 150 mg twice daily, rivaroxaban at 10 or 15 mg once daily in the morning, apixaban at 2.5 or 5 mg twice daily, or edoxaban at 30 or 60 mg once daily in the morning.
All patients received oral anticoagulation for more than one week before the ablation procedure; most of the patients received that for more than one month. The DOACs were continued throughout the periprocedural period, or discontinued only on the day of the procedure and reinitiated on the next morning after the procedure[7,8].
Immediately after the femoral venous puncture, a heparin bolus of 5,000-10,000 units was administered intravenously, followed by a continuous and additional bolus heparin infusion to maintain an activated clotting time (ACT) between 300 and 400 seconds. The ACT was measured every 10 minutes until the ACT value reached 300 seconds and there after every 10-30 minutes. The intravenous heparin administration was once stopped at the end of the procedure, and protamine was administered to partially reverse the anticoagulation effects of heparin at the operator’s discretion. The venous sheaths for the ablation were removed, and hemostasis of the femoral venous puncture sites was achieved by manual compression for at least five minutes or figure-of-eight sutures[9,10].All patients underwent bed rest foreight hours to maintain hemostasis, and received a continuous infusion of unfractionated heparin at a dose of 10,000 units per 24 hours until the DOACs were administered on the next morning after the procedure. Post-ablation oral anticoagulation was continued for at least three months.
The catheter ablation procedures have been previously described in detail[7,8]. All patients were kept under deep conscious sedation throughout the procedure, using propofol or dexmedetomidine and pentazocine.
The ablation strategy using an open-irrigated radiofrequency ablation catheter consisted of a pulmonary vein (PV) isolation (PVI) in patients undergoing an initial AF ablation and in those with PV reconnections after one or more PVI procedures, and additional ablation for non-PV foci and substrate modification for AF including a continuous fractionated atrial electrogram ablation and/or linear ablation if necessary.During the procedure, a total of four sheaths, three 8-Fr or 8.5-Fr transseptal sheaths (SL0 or Agilis™ NxT, St. Jude Medical, St. Paul,MN, USA) and one 6-Fr sheath
for a multielectrode catheter positioned in the coronary sinus (CS), were inserted into the right femoral vein.
A balloon-based PVI using a 28-mm second generation cryoballoon catheter (Arctic Front Advance® cardiac ablation catheter, Medtronic, Minneapolis, MN, USA) or radiofrequency Hot Balloon catheter (SATAKE Hot Balloon, Toray Industries, Inc., Tokyo, Japan) was performed in patients undergoing an initial AF ablation. If a PVI could not be completed by multiple balloon ablation applications, touch-up ablation for the remaining gaps was performed using an irrigated radiofrequency catheter.A total of three sheaths were inserted into the right femoral vein. During the cryoballoon ablation, one 15-Fr transseptal sheath (FlexCath Advance® Steerable Sheath, Medtronic, Inc.), and two 6-Fr sheaths for multielectrode catheters for CS and phrenic nerve pacing were used. The 6-Fr sheath was exchanged to an 8-Fr transseptal sheath (SL0, St. Jude Medical.) if touch-up ablation was performed. During the radiofrequency Hotballoon ablation, two transseptal sheaths, a 17-Fr steerable sheath (TRESWALTZ, Toray Industries, Inc.) and 8-Fr sheath (SL0, St. Jude Medical.) for a circular mapping catheter, and one 6-Fr sheath for a multielectrode catheter for CS and phrenic nerve pacing, were used.
Diagnosis of Symptomatic VTEs
If patients exhibited clinical signs or symptoms suggesting the presence of a VTE following the ablation procedure, such as pain, swelling, redness, and superficial venous dilatation of the leg, chest pain, and dyspnea, those patients underwent venous ultrasonography, contrast-enhanced computed tomography (CT), and D-dimer testing to evaluate any presence of DVT or PTE.
Normally distributed continuous variables are expressed as the mean ± standard deviation (SD), non-normally distributed continuous variables areexpressed as the median and interquartile range (IQR, 25th–75th percentile), and categorical variables are expressed as the number and percentage of patients.
The demographics and baseline characteristics of the study population are summarized in [Table 1]. The age was 64±10years, percentage of male gender72.5%, and body mass index (BMI) 23.9± 3.5 kg/m2.Out of the 2,193 patients, 2,062 patients (94.0%) underwent radiofrequency catheter-based ablation,80 (3.7%)cryoballoon ablation, and 51 (2.3%) radiofrequency Hot Balloon ablation.
Table 1. Demographics and baseline characteristics of the study population
| Number of patients |
2193 |
| Age (years) |
64 ± 10 |
| Male gender |
1589 (72.5) |
| Body weight (kg) |
65.5 ± 12.1 |
| Body mass index (kg/m2) |
23.9 ± 3.5 |
| Type of atrial fibrillation |
|
| Paroxysmal |
1210 (55.2) |
| Persistent |
662 (30.2) |
| Long-standing persistent |
322 (14.7) |
| Structural heart disease |
276 (12.6) |
| Hypertension |
1200 (54.8) |
| Diabetes mellitus |
328 (15.0) |
| Heart failure |
182 (8.3) |
| Stroke/transient ischemic attack |
158 (7.2) |
| Past history of venous thromboembolisms |
2 (0.091) |
| CHADS2 score |
1 (0–2) |
| CHA2DS2-VASc score |
2 (1–3) |
| HAS-BLED score |
1 (0–2) |
| BNP (pg/ml) |
59.5 (12.5-132) |
| Creatinine (mg/dl) |
0.74 (0.63-0.97) |
| Estimated GFR (mL/min/1.73m2) |
66 (58-76) |
| D-dimer (μg/ml) |
0.4 (0.3-0.5) |
| Left atrial diameter (mm) |
41(37-45) |
| Left ventricular ejection fraction (%) |
65 (59-69) |
| Type of direct oral anticoagulants |
|
| Dabigatran |
619 (28.3) |
| Rivaroxaban |
648 (29.5) |
| Apixaban |
565 (25.8) |
| Edoxaban |
361(16.5) |
| Left atrial ablation device |
|
| Irrigated radiofrequency ablation catheter |
2062 (94.0) |
| Cryoballoon |
80 (3.7) |
| HotBalloon |
51 (2.3) |
Data are given as the mean ± SD, median (IQR), or number of patients (%).
The clinical characteristics and outcomes of the two symptomatic DVT patients are described in detail as follows, and are summarized in [Table 2].
No symptomatic PTE occurred in this series.
Table 2. Clinical and procedural characteristics ofthe twopatients with symptomatic DVTs
|
Case 1 |
Case 2 |
| Age (years) |
72 |
74 |
| Gender |
Female |
Male |
| BMI (kg/m2) |
18.5 |
17.8 |
| Type of atrial fibrillation |
Paroxysmal |
Paroxysmal |
| Periprocedural oral anticoagulation |
Apixaban 2.5 mg twice daily |
Edoxaban 30 mg once daily |
| Ablation procedure |
Cryoballoon-based PVI + CTI linear ablation |
HotBalloon-based PVI + CTI linear ablation*
SVC isolation**
|
| Number of sheathsfor the ablation |
3 |
3* |
|
|
3* |
| Total procedure time (minutes) |
111 |
101* |
|
|
77** |
| Period from the procedure to VTE occurrence (days) |
72 |
74 |
| Age (years) |
|
23* |
|
8 |
4** |
| Post-VTE oral anticoagulation |
Apixaban 10 mg twice daily for the first 7 days, followed by 5 mg twice daily |
Rivaroxaban 15 mg twice daily for the first 21 days, followed by 15 mg once daily |
| Age (years) |
72 |
74 |
| Clinical outcome |
1Disappearance of the thrombi after 30 days |
Disappearance of the thrombi after 22 days |
CTI, cavotricuspid isthmus; PVI, pulmonary vein isolation; SVC, superior vena cava; VTE, venous thromboembolism. The ablation procedures and procedure-related data during the first (*) and second (**) ablation procedures, and period from the first (*) and second (**) procedure to the VTE occurrence are shown.
A 72-year-old female underwent cryoballoon ablation of paroxysmal AF and received oral anticoagulation with apixaban at a dose of 2.5 mg twice daily. The reduced dose of apixaban was used because two of the three dose reduction criteria (age, ≥80 years; body weight, ≤60 kg; serum creatinine, ≥1.5 mg/dL) were met as follows: Body weight, 59kg and serum creatinine, 1.52 mg/dL. The total procedure time was 111 minutes. Complete hemostasis of the right femoral venous puncture sites was achieved with figure-of-eight sutures, which were removed on the next morning after the procedure. The patient was discharged without any complications on the second post-procedural day.
The patient presented with right leg pain and swelling on the 8th post-procedural day. Duplex ultrasonography and contrast-enhanced CT identified a DVT in theright common femoral vein [Figure 1]. Apixaban was given at a dose of 10 mg twice daily for the first 7 days, followed by 5 mg twice daily. Duplex ultrasonography verified the complete disappearance of the thrombi by oral anticoagulation with an increased apixaban dose for 30 days. Neither a DVT recurrence nor bleeding events occurred during the follow-up period.
Figure 1. Duplex ultrasonography showingthe presence of a DVT in the right common femoral vein in Case 1.A B-mode examination revealed a hypoechoicthrombus within the vein (dotted-line area) in the long axis view (Panel A). A Color-flow Doppler examination revealed the absence of Doppler signals within the venous lumen, indicating the absence of blood flow, and the presence of noncompressibility of the venous segment in the long and short axis views (Panels B and C).
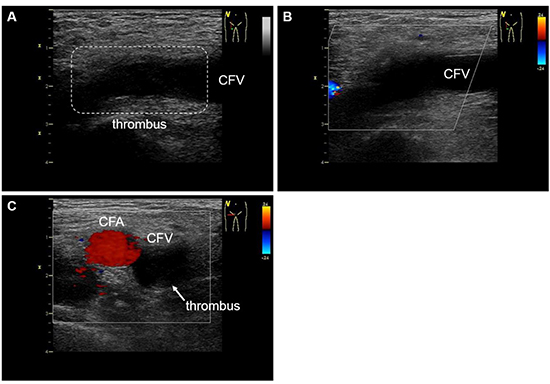
CFA, common femoral artery; CFV, common femoral vein.
A 74-year-old male underwenta radiofrequencyHotBalloon ablation of paroxysmal AF and received oral anticoagulation with edoxaban at a dose of 30 mg once daily. The patient’s body weight was 43 kg, and a reduced edoxaban dose was used according to the dose reduction criteria (body weight, ≤60 kg). The total procedure time was 101 minutes. Complete hemostasis of the right femoral venous puncture sites was achieved with figure-of-eight sutures, and the patient was discharged on the second post-procedural day.
The patient underwent a second ablation procedure for recurrent AF on the 19thday after the first procedure. During the second procedure, the femoral venous punctures were very difficult, but two transseptal sheaths and one 6-Fr sheath were inserted into the right femoral vein. All PVscontinued to be isolated, and an electrical isolation of the superior vena cava (SVC) was performed using an irrigated radiofrequency catheter because AF triggers originating from the SVC were documented. The total procedure time was 77 minutes, and complete hemostasis of the venous puncture sites was achieved with figure-of-eight sutures. The patient was discharged without any complications on the second day after the second procedure.
The patient presented with right leg pain and swelling on the 4th day after the second procedure. Duplex ultrasonography and contrast-enhanced CT identified a DVT in the right common femoral vein [Figure 2]. Edoxaban was changed to rivaroxaban at a dose of 15 mg twice daily for the first 21 days, followed by 15 mg once daily. Duplex ultrasonography verified the complete disappearance of the thrombi after 22 days of oral anticoagulation with rivaroxaban. Neither a DVT recurrence nor bleeding events occurred during the follow-up period.
Figure 2. Duplex ultrasonography showing the presence of a DVT in the right common femoral vein in Case 2.A B-mode examination revealed a hypoechoic thrombus within the vein (dotted-line area) in the long axis view (Panel A). A Color-flow Doppler examination revealed the absence of Doppler signals within the venous lumen, indicating the absence of blood flow, and the presence of noncompressibility of the venous segment in the long and short axis views (Panels B and C).
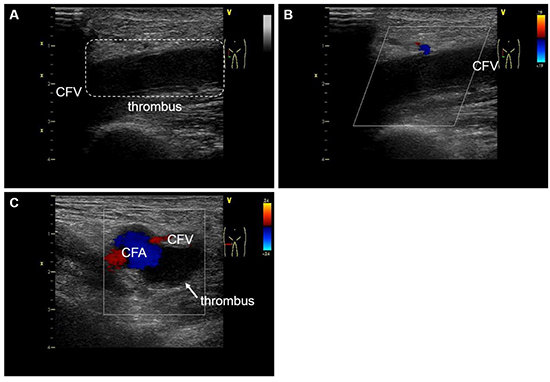
CFA, common femoral artery; CFV, common femoral vein.
To the best of our knowledge, this is the first report to describe the incidence of symptomatic VTEs in patients who underwent catheter ablation of AF with periprocedural oral anticoagulation using DOACs.We demonstrated that the occurrence of symptomatic DVTs was extremely rare, and no symptomatic PTEs occurred during the periprocedural period of AF ablation under periprocedural DOAC treatment.
The incidence of symptomatic DVTs after AF catheter ablation has been reported to be 0-0.39% in previous retrospective[11] and prospective[112,15] studies, and is comparable to that of the present study. Those previous studiesincludedpatients receiving periprocedural anticoagulation with either warfarin[11,13] orlow-molecular-weight heparin[14,15], but no patients receivedperiprocedural anticoagulation with DOACs. Winkle et al.[16] reported that the incidence of PTEs was 0.29% in a retrospective registry with interrupted oral anticoagulation with warfarin.
Factors associated with VTEs
The occurrence of periprocedural VTEs is associated with various factors: the procedure time[17]
, bed rest duration[18], number and size of the sheaths for ablation[17], periprocedural anticoagulation regimen[102,19] and patient characteristics including the age[20] and BMI[18,21]. AF catheter ablation usuallyrequires multiple venous sheaths inserted into a single femoral vein and a relatively long bed rest duration for hemostasis of the venous puncture sitesafter the procedure.Several preliminary studieshave suggested that injuries to the vascular endothelium caused by the placement of venous sheathsand venous stasis are possible mechanisms for venous thrombus formation[22,23].In addition, percutaneous catheter ablation itself is capable of activating the coagulation system, possibly increasing the risk of a thrombosis[19,24].Moubarak et al. demonstrated that large sheaths and a long proceduretimewere risk factors for a DVT after right-sided electrophysiological procedures[17]. The procedure time in the two DVT patients in our studywas not so long: 77-111 minutes. On the other hand, 15-Fr and 17-Fr large sheaths for the balloon-based procedures were used in both DVT patients, which may have been a risk for a DVT. In Case 2 of our study, a DVT was detected on the fourth day after the second procedure. However, it is probable that a pre-symptomatic DVT had already occurred after the first HotBalloon ablation procedure, because the right femoral venous punctures were very difficult during the second procedure.Ultrasonographic guidance during the femoral venous puncture for AF ablation can be useful for detecting venous occlusions[25], and a reduction in vascular access complications[26].
Periproceduraloral anticoagulation with DOACs may be associated with an extremely low incidence of a VTE. Burstein et al.[2] reported that AF ablation revealed a lower incidence of symptomatic DVTs and PTEs than non-AF ablation, which was likely due to the use of routine periprocedural anticoagulation.In the present study, either of the two anticoagulation protocols were used at the physicians’ discretion: uninterruption of the DOACs throughout the periprocedural period or interruption of the DOACs on the procedural day and reinitiation of the DOACs in the next morning after the procedure. The interrupted DOAC protocol was used in both DVT patients, which may have contributed to the DVT occurrence, despite a minimal interrupted period of the DOACs. However, it probably does not seem that the anticoagulation protocol was directly related to the occurrence of the DVT,becausethe DVT was detected on the fourth and eighth day after reinitiating the DOACs, respectively, for those two patients.
Periprocedural symptomatic VTEs were an extremely rare occurrence in the patients who underwent catheter ablation of AF and received periprocedural oral anticoagulation with DOACs. Symptomatic DVTs after AF catheter ablation may be adequately treated by increasing the DOAC dose or changing the DOAC type.






