Atrial Arrhythmias in Chagas’ Disease
Jorge O. Diaz1, Camilo A. Rueda2
1
Central Florida Regional Hospital, Sanford, Fl; Fundación Cardiovascular de Colombia, Bucaramanga, Colombia.2
Pontificia Universidad Javeriana, Bogota, Colombia.
There is extensive knowledge in the ablation of ventricular arrhythmias in patients with Chagas’ cardiomyopathy, as well as specific characteristics of the arrhythmogenic substrate, and the need for an epicardial approach to achieve success. On the contrary, no publications currently address the ablation of atrial fibrillation in these patients or the characteristics of the arrhythmia such as the successful ablation sites. Our two case reports highlight the association of Chagas’ disease with atrial arrhythmias, the tailored approach that was needed to give an appropriate treatment and a discussion of our current knowledge of Chagas’ cardiomyopathy as a substrate for atrial arrhythmias.
Key Words : Atrial, Arrythmias, Chagas, Atrial Fibrillation.
Correspondence to: Dr. Jorge O. Diaz,South International Parkway, Suite 1261, Lake Mary
Since the first description of pulmonary vein depolarizations as triggers of atrial fibrillation (AF) by Haïssaguerre, there has been a widespread use of ablation techniques for the treatment of paroxysmal atrial fibrillation. Furthermore, the techniques have been modified and have also included patients with persistent atrial fibrillation as candidates for ablation procedures [1]. In most of the industrialized countries, atrial fibrillation is the result of many etiologies, including hypertensive heart disease, obesity, obstructive sleep apnea, heart failure and coronary artery disease. This is also valid for third world countries; however, other causes of heart disease, such as malnutrition and parasitic infections including Chagas’ disease are of importance, especially in areas where there is a high prevalence [2].
Pulmonary vein isolation (PVI) is the cornerstone for all the existing ablation techniques targeting paroxysmal atrial fibrillation. PVI has been extrapolated to persistent atrial fibrillation, with limited results, due to the presence of atrial fibrosis and other abnormalities acting as substrate. Therefore, modification of the arrhythmogenic substrate has been postulated, with better, although not satisfactory results. Linear ablation, elimination of complex fractionated atrial electrograms and ganglionic plexi, ablation of low voltage bridges (areas of fibrosis) and lately, targeting focal impulses and rotors (FIRM).
Chagas’ cardiomyopathy manifests as conduction system disease, ventricular arrhythmias and sudden cardiac death. There is extensive knowledge in the ablation of ventricular arrhythmias in these population, as well as specific characteristics of the arrhythmogenic substrate, and the need for an epicardial approach to achieve success. On the contrary, no publications currently address the ablation of atrial fibrillation in these patients or the characteristics of the arrhythmia such as successful ablation sites.
We present two cases of atrial arrhythmias in patients with Chagas’ cardiomyopathy in which a conventional approach would have been unsuccessful due to the specific characteristics of the arrhythmia, in regards to the origin, substrate and successful ablation sites.
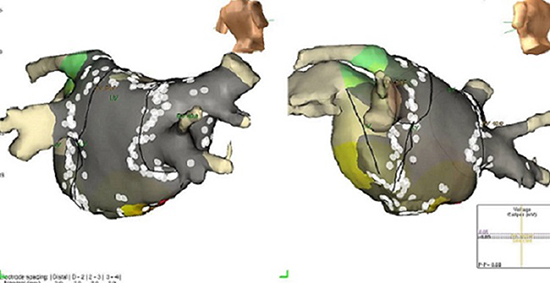
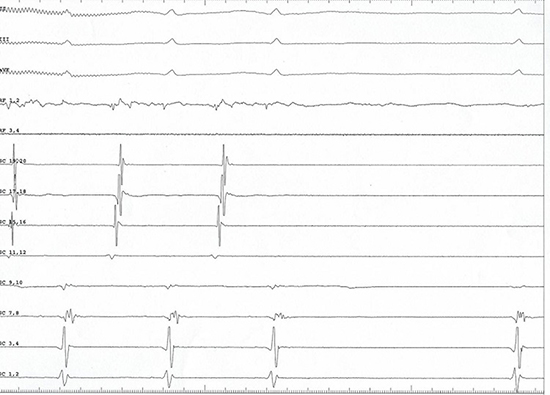
A 56 years old male patient with a history of Chagas’ cardiomyopathy, ventricular tachycardia and implantation of a dual chamber defibrillator, who experienced inappropriate shocks for atrial fibrillation, despite treatment with beta-blockers and amiodarone. Echocardiogram showed an ejection fraction of 30%, with left and right atrial areas measured at end systole of 17 and 19 cm2, respectively. A duo decapolar catheter was placed along the Crista Terminalis(CT) and in the Coronary Sinus (CS). A quadripolar catheter was placed in the His bundle position. Single transeptal technique was used. St. Jude Agilis steerable sheath, a Reflection Spiral decapolar catheter and a Cool Flex ablation catheter, were used for 3D mapping and ablation purposes. The initial approach included Wide Area Circumferential Ablation (WACA) followed by elimination of Complex Fractionated Atrial Electrograms (CFAE) and linear ablation of the roof, posterior wall of the left atrium and the mitral isthmus. Despite demonstration of pulmonary vein and posterior wall isolation as well as complete electrical silence in the left atrium [Figure 1], AF persisted.
Figure 1. PVIand Posterior Wall isolation.
Fibrillatory activity persistedin the channels recording the right atrium[Figure 2]. Therefore, we proceeded with CFAE mapping of this chamber. CFAE were eliminated in the RA, resulting in organization of tachycardia into an atrial flutter with a cycle length of 290 ms [Figure 3], successfully entrained in the lower lateral wall of the right atrium [Figure 4]. Interestingly, there was a large area of scar encompassing the posterior and lateral wall of the RA. An ablation line from the superior vena cava to the inferior vena cava further increased the cycle length and changed the activation, findings consistent with an atrial tachycardia from the low Crista Terminalis [Figure 5], which was successfully terminated with restoration of sinus rhythm. Clinically, the patient has been asymptomatic and interrogation of his device has not shown any recurrent atrial arrhythmias.
Figure 2. AF continues in the right atrium.
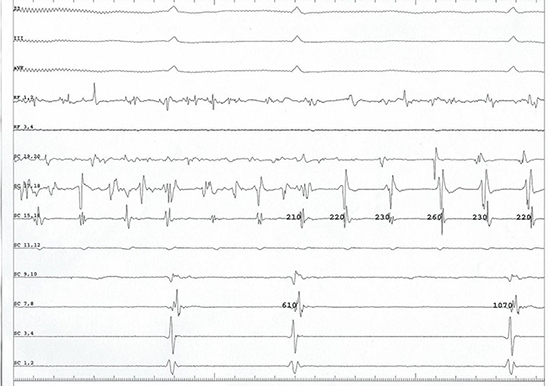
Figure 3. Organization of fibrillatory activity into atrial flutter.
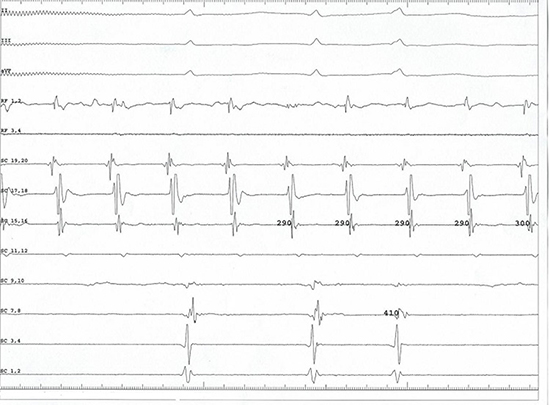
Figure 4. Right atrium activation map and ablation.
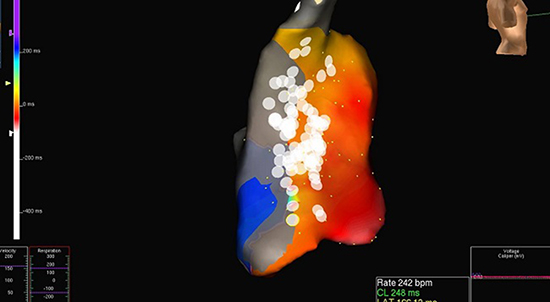
Figure 5. Termination of right atrial tachycardia
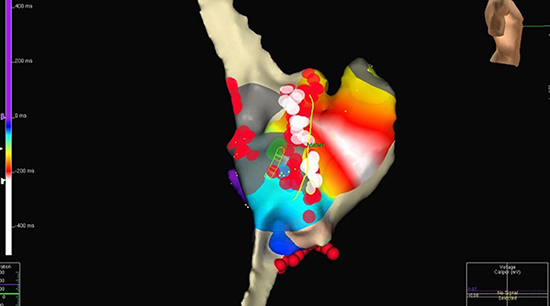
A 63 years old male patient who presented with sustained palpitations due to a narrow complex tachycardia with hemodynamic instability. Echocardiogram revealed an ejection fraction of 55%, mild left ventricular dilatation, moderate aortic insufficiency and mild biatrial enlargement. The left atrial area at end systole is 27 cm2. Antibodies against T. cruziwere positive by enzyme immunosorbent assay (EIA). Initial ECG is consistent with atrial flutter with a cycle length of approximately 280 ms [Figure 6]. A duo decapolar catheter was placed along the CT and in CS. A quadripolar catheter was placed in the His bundle position but later was placed in the distal CS. A St. Jude Cool Flex catheter was used for mapping and ablation purposes. During the anesthesia induction, the patient became hemodynamically unstable, therefore he was cardioverted. After his vital signs normalized, he was easily induced into a fast atrial flutter with a cycle length of 180 to 200 ms.Occasionally, there were episodes that resembleAF. An initial cavotricuspid isthmus ablation line did not impact the tachycardia;therefore, we proceeded with activation mapping. An ablation line from the superior vena cava to the inferior vena cava further increased the cycle length and subsequently terminated the tachycardia [Figure 7]. Isuprel was given up to 20 mcg/min and aggressive pacing maneuvers were performed with no induction on any other atrial arrhythmias.
Figure 6. EGMs of Atrial Flutter
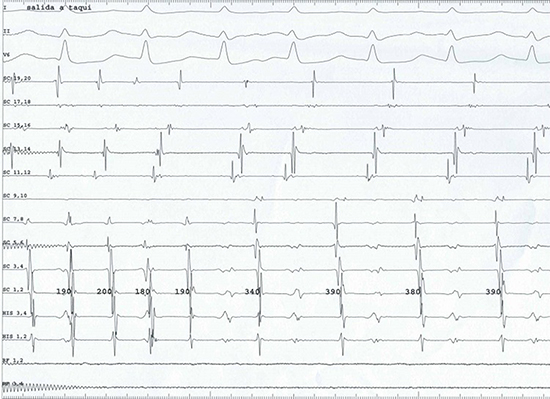
Figure 7. Right atrium activation map and ablation line
CD affects8-12 million people in Latin America and for the US it is estimated that 300,000 people suffer of chronic Chagas’ disease [3,4].Although the pathogenesis of CD is not completely understood, it is known that reparative fibrosis is the hallmark of chronic CD [3]. In CD, fibrosis promotes the development of dilated cardiomyopathy and usually affects the ventricular myocardium. Furthermore, the fibrotic process generally becomes the substrate for ventricular tachyarrhythmias, but its association with the development of AF is controversial [4].
Over the past 20 years, there has been an explosion of knowledge about AF etiologies and mechanisms and new forms of heart disease. Clinical AF results from an interaction between triggers and sustaining mechanisms, such as substrates, composed of electrical and/or structural components. AF is often triggered by ectopy from the pulmonary veins. Pulmonary vein triggers may be promoted by activity from nearby ganglionatedplexi, and relate to structural-functional abnormalities at the junction between left atrial and pulmonary vein tissue [5,8]. Although pulmonary veins accounts for a majority of cases of AF, less defined atrial sites can have an association with atrial fibrillation. This may explain, in part, why some patients with presumed paroxysmal AF respond poorly where as others with presumed persistent AF respond favorably to pulmonary vein isolation alone. Furthermore, recent data suggests that atrial fibrosis, a marker of the underlying substrate, can be visualized using cardiac magnetic resonance imaging and be used to individualize the strategy for catheter ablation [9].
The reported cases illustrate how CD can produce non-common arrhythmogenic substrate and possible foci as well. For instance, the first case shows how traditional PVI, although successfully done, was not able to eliminate the arrythmogenic substrate and AF persisted in the right atrium. Furthermore, the second case illustrates how atrial fibrosis developed in the posterior wall of the right atrium and acted as substrate for a reentrant atrial tachycardia. In general, these findings support the hypothesis that fibrosis and Chagasic cardiomyopathy serve as substrate for multiple atrial arrhythmias and that traditional ablation approaches can fail to treat atrial arrhythmias in patients with CD.
Finally, we believe that future directions in AF management and research will be better served if AF is classified in a more utilitarian and precise fashion, perhaps using terms that assign both etiologic and mechanical information when appropriate.Furthermore, it would be of great interest to correlate the relationship between more objective data (i.e., device-derived) about the temporal persistence of AF with cardiac magnetic resonance imaging findings.
Chagas disease affects the heart tissue and promotes the development of fibrosis and cardiomyopathy, which may be the substrate for arrhythmogenic foci and substrate. Clinicians should be aware of these changes and be prepared to properly map the arrhythmia activation in order to deal with them appropriately during ablation procedures.






