Incidence and Predictive Factors of Hidden Atrial Fibrillation Detected by Implantable Loop Recorder After an Embolic Stroke of Undetermined Source
Castro Urda Víctor1, Parra Esteban Carolina1, Toquero Ramos Jorge1, Carneado-Ruiz Joaquín5, Sánchez García Manuel1, Cobo Marcos Marta2, Fernández Villanueva José María1, Pham Trung Chinh1, Ortega Marcos Javier3, Mingo Santos Susana4, Jiménez Sánchez Diego1, Jiménez Ortiz Carlos5, Fernández Lozano Ignacio1
1Electrophysiology Unit. Cardiology Service. Hospital Puerta de Hierro Majadahonda. Spain..2Heart failure and Miocardiopathy Unit. Cardiology Service. Hospital Puerta de Hierro. Majadahonda. Spain..3Critical Care Unit. Cardiology Service. Hospital Puerta de Hierro. Majadahonda. Spain.4Ecocardiography Unit. Cardiology Service. Hospital Puerta de Hierro. Majadahonda. Spain.5Stroke Unit. Neurology Service. Hospital Puerta de Hierro. Majadahonda. Spain..
The term embolic stroke of undetermined source (ESUS) has been defined for patients with ischemic strokes, where neither a cardioembolic nor a non-cardiac source can be detected. These patients may have asymptomatic episodes of atrial fibrillation (AF). Prolonged monitoring with implantable loop recorder (ILR) and daily remote interrogation in patients after an ESUS has shown an incidence of AF of about 25%.
The main objective of this study was to analyze the incidence and predictive factors of atrial fibrillation in patients with ESUS who underwent an ILR implantation.
It was a single center study. From June 2013 to January 2017 all consecutive patients with an ESUS, who underwent an ILR implantation searching for hidden AF, were included. Possible predictive factors of AF were also analyzed.
65 patients were included (mean age 65.4±13.8 years, 55.4% males, mean CHA2DS2VASc score 2.3± 1.5). After a median follow-up of 17.1±10.7 months, AF was detected in 19 (29.2%) of patients. Variables associated with AF were:
age > 65 years (HR 9.45 (CI 95% 1.25-71.34); p= 0.02), CHA2DS2VASC score≥2 (HR 4.09 (CI 95% 0.93-17.87); p=0,06), left atrial enlargement (HR 2.29 (CI 95% 0.89-5.91); p=0.08) and presence of Supraventricular premature complex(SVC) on 24-hour Holter (HR 4.05 (CI 95% 1.55-10.57); p = 0.004) A cut-point of 0.15% for SVC was identified to predict AF with a sensitivity and specificity of 88.9 and 90%, respectively. A CHA2DS2VASc score<2 and age<65 years showed a negative predictive value to exclude AF of 91.3% and 96%, respectively.
A high incidence of AF was detected in this population. Age >65 years, LA enlargement, CHA2DS2VASC score≥2 and presence of SVC on 24-hour Holter are predictive factors of AF in patients with ESUS.
Key Words : Atrial Fibrillation, Embolic Stroke of Undetermined Source, CHA2DS2-VASC, Supraventricular Premature Complex, Left Atrial Enlargement, Implantable Loop Recorder.
Correspondence to: Dr. Víctor Castro Urda
Electrophysiology Unit. Cardiology Service. Hospital Puerta de Hierro Majadahonda. Spain.
Ischemic stroke is one of the leading causes of death and disability[1]. It is known as cryptogenic stroke when its origin is unknown, what happens in 20-40% of cases after an extensive diagnostic workup[2-6]. One of the most frequent causes is hidden atrial fibrillation (AF)[7], and risk of stroke recurrence is drastically reduced with anticoagulant therapy[7-8].
In patients with cryptogenic stroke, prolonged monitoring (for up to 36 months) with implantable loop recorder(ILR)[9], has shown and incidence of previously undiagnosed AF of about 30%, much higher than the one got by conventional follow-up. Similarly, incidence of AF was 16.1% in the subgroup of patients who were followed with an event recorder for a period of 30 days after a cryptogenic stroke[10].
The CHA2DS2VASc score is clearly validated to predict risk of stroke in patients with non-valvular AF[11]. Risk is estimated by the presence or absence of some clinical variables such as: heart failure, hypertension, age, diabetes mellitus, previous stroke or transient ischemic attack, vascular disease or sex.
Recently, embolic stroke of undetermined source (ESUS), and complementary tests needed for its diagnosis, has been described as a new clinical entity[12]. The clinical construct ESUS was introduced to identify patients with non lacunar cryptogenic ischemic strokes in whom embolism was the likely stroke mechanism.
This new definition allows a more homogeneous comparison between studies of what was previously defined as cryptogenic stroke.
From June 2013 to January 2017, all consecutive patients that had suffered an ESUS and who, according to the opinion of the Cardiology and Neurology departments, were candidates for an ILR were included. The diagnosis of stroke was made by a neurologist, based on symptoms and radiological (Magnetic resonance imaging, MRI; or computed tomography, CT) findings. The diagnosis of ESUS was made after an extensive study that included: blood test with complete blood count, coagulation, biochemistry with lipid profile, chest X-ray, supra-aortic vessels echo-Doppler, transcranial Doppler, and CT angiography or angio-MRI, if needed. A 12 lead Electrocardiogram (ECG) was also performed, 24-hour Holter monitoring, transthoracic or transesophageal echocardiogram or thrombophilia screening (in subjects under 55 years). Complementary tests did not show a clear cause for the stroke. Patients with a patent foramen ovale (diagnosed by transesophageal echocardiography) were included.
All patients signed an informed consent form before entering the study. They underwent implantation of an ILR Reveal XT (@Medtronic) or Reveal LINQ (@Medtronic) [Figure 1] by the Arrhythmia Unit of the participant center. It was an ambulatory procedure and the device was implanted subcutaneously in the prepectoral left area with local anesthesia. These devices can detect and store automatically episodes of AF, independently of symptoms or heart rate[14].
Figure 1. Reveal LINQ and Reveal XT. Reveal LINQ size is noticeably smaller

Follow-up was performed through remote monitoring with the Care-Link (@Medtronic) system. A monthly report from each patient was obtained. With the Reveal LINQ device, transmission of data was done automatically whilst the Reveal XT system needed patient interaction to send the information.
Episodes of AF were defined as presence of an irregular rhythm, without P waves and with a duration of at least 30 seconds in Reveal XT and 2 minutes in Reveal Linq. All episodes were analyzed and reviewed by a technician and 2 electrophysiologists who were blinded to the clinical information of the patient whose records were analyzing [Figure 2].
Figure 2. Atrial fibrillation episode in patient with a Reveal LINQ.

The following variables were evaluated as possible predictors of AF: age, sex, arterial hypertension, diabetes mellitus, presence of cardiomyopathy, prior stroke, peripheral artery disease, ischemic heart disease, atrial tachycardia, supraventricular premature complexes (SVC), percentage of SVC on 24-hour Holter monitoring, smoking habits, CHA2DS2-VASC score and left atrial volume measured with transthoracic or transesophageal echocardiography. Atrial tachycardia was defined as presence of a tachyarrhythmia of at least 4 beats, at a rate faster than 100 beats per minute with a P wave that looked different from the one in sinus rhythm. Presence of SVC was defined as at least 1% of SVC during the 24-hour Holter monitoring. All these tests were performed using a Holter “210 Plus with Zymed Algorithm, Philips Medical, Andover, MA, USA”, with simultaneous 3-channel recording capacity and 12 lead ECG estimation. The stroke that triggered loop recorder implantation was not taken into account for the calculation of CHA2DS2-VASC score, what means that subjects with CHA2DS2-VASC< 2 could be included in the study. Left atrial enlargement was defined as a left atrial volume corrected per body surface area > 34 ml/m2, calculated by biplane disc summation method in apical 2 and 4-chamber apical view. All echocardiographic studies were performed with a Philips Echocardiogram IE33 from Philips Medical, Andover, MA, USA.
Main endpoint of the study was detection of AF through the use of an ILR.
Categorical variables are expressed as number of observations (frequency) and percentage. Exact Fischer test was used to compare this type of variables. Continuous variables are expressed as mean ± standard deviation (SD) or median and interquartile range, if not normally distributed. Kolmogorov-Smirnoff or Shapiro- Wilk tests were used to check if variables had a normal distribution.
T Student or U Mann-Whitney tests were used to analyze differences between groups.
The Kaplan-Meier method was performed to analyze survival free of AF. Kaplan-Meier curves and log Rank tests were applied to check differences in survival free of AF between subgroups according to: CHA2DS2VASc score, age, presence of SVC and left atrial size. Fischer test was used to analyze predictive variables of AF. A ROC (Receiver Operating Characteristic) analysis was performed to find out a cut off point for % SVC on 24h Holter monitoring to predict AF.
All statistical analysis was performed using software SPSS 20 Statistics of IBM Corp., Armonk, NY, USA
An ILR was implanted in 65 patients. Reveal XT was implanted in 13,8%. Reveal Linq was implanted in 86,2%. Baseline characteristics of study population are shown in [Table 1]. Mean age was 65.4 ±13.8 years. 55.4% were males. All patients had normal left ventricular ejection fraction and none of them had a severe valvular heart disease. Mean CHA2DS2VASc score was 2.3±1.5. 64.6% of patients had a CHA2DS2VASc score ≥2.
The ILR was implanted after a median time of 56 days [Q1-Q3; 28-109] from the diagnosis of ESUS.
Table 1. Baseline characteristics of study population.
| Variable |
|
| Age (years) |
65.43±13.8 |
| Males (%) |
36 (55.4) |
| HTA (%) |
37 (56.9) |
| DM (%) |
10 (15.4) |
| Dyslipidemia (%) |
17 (26.2) |
| Current smoker (%) |
22 (28.2) |
| Ex-smoker (%) |
4 (5.1) |
| Valvulopathy (%) |
0 (0) |
| Normal LVEF (%) |
65 (100) |
| Ischemic cardiomiopathy (%) |
4 (6.2) |
| Peripheral vascular disease (%) |
2 (3.1) |
| CHA2DS2VASc score |
2.26 ± 1.5 |
DM: Diabetes mellitus, LVEF: Left ventricular ejection fraction, HTA: arterial hypertension.
[Table 2] shows imaging tests and Holter results. 21.5% of patients had left atrial enlargement, defined by volume parameters. 13.8% of patients had SVC and 21.5% atrial tachycardia as defined per protocol.
After a mean follow-up of 17.1 ± 10.7 months, AF was detected in 19 (29.2%.) of patients. [Figure 3] shows survival free of AF curves.
Figure 3. Atrial fibrillation-free survival curve. AF: atrial fibrillation
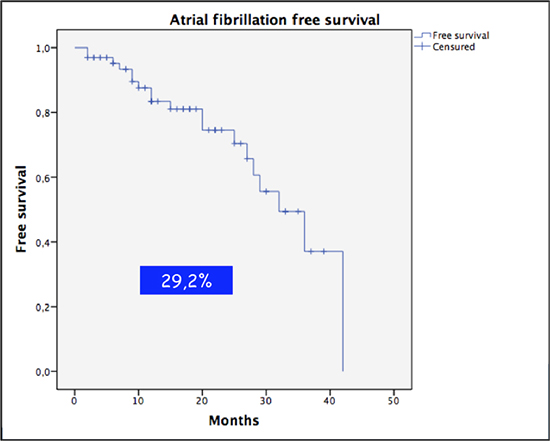
Table 2. Complementary data from Holter and echocardiogram
| Variable |
|
| PFO (%) |
9 (13.8) |
| Left atrial diameter (mm) |
35.27±5.13 |
| Left atrial volume (ml/m2) |
27.74±8 |
| Enlarged left atrium (%) |
14 (21.5) |
| AT on Holter (%) |
14 (21.5) |
| SVC on Holter (%) |
9 (13,8) |
PFO: patent foramen ovale; SVC: supraventricular premature complex; AT. Atrial tachycardia;
The incidence of AF at 1, 2 and 3 years is showed in [Table 3].
Table 3. AF incidence according to year of FU.
| Variable |
PORCENTAGE |
| AF incidence at 1 year FU |
13 (95% CI, 5-22) |
| AF incidence at 2 year FU |
18 (95% CI, 8,7-28) |
| AF incidence at 2 year FU |
27 (95% CI, 16-38) |
AF: Atrial fibrillation. FU: Follow up
Mean episode duration was 12,3 hours (SD 15,52)
The first episode of AF was diagnosed at a median time of 31 days [Q1-Q3; 11-59] from ILR implantation. Anticoagulant therapy was started in every patient with AF diagnosis as soon as the physician was aware of it. Median time to detection was not different according to device type (28 days (Q1-Q3 20,5-117) vs 31 days (Q1-Q3 11-56) p=0,84) with XT compared to Linq respectively.
Patients who had AF were significantly older (75.8±7.9 vs. 61.1±13.4 years; p=0.005), had more frequently SVC (44.4% vs 2.5%; p<0.001) and a higher left atrial volume (31.5±6.9 vs 26.1±6.1 ml/m2; p=0.003). Percentage of patients with a CHA2DS2VASc score ≥2 was also higher in the AF group (89.5% vs 54.3%; p=0.009) compared with those patients in which AF was not detected[Table 4]. Anticoagulant therapy was started in all patients with newly detected AF.
Table 4. Differences between patients with/without atrial fibrillation during follow-up.
|
Atrial fibrillation (19) |
No Atrial fibrillation (46) |
P value |
| Age (years) |
75.8±7.9 |
61.1±13,4 |
0.005 |
| Males (%) |
9 (47.4) |
27 (58.7) |
0.4 |
| HTA (%) |
14 (73.7) |
23 (50) |
0.08 |
| DM (%) |
2(10.5) |
8 (17.4) |
0.71 |
| Dyslipidemia (%) |
3 (15.8) |
14 (30.4) |
0,.5 |
| CHA2DSVASC≥2 (%) |
17 (89.5) |
25 (54.3) |
0.009 |
| IC (%) |
0 (0) |
4 (8.7) |
0.31 |
| PVD (%) |
1 (5.3) |
1 (2.1) |
0.5 |
| AT on Holter (%) |
8 (44.4) |
6 (15) |
0.31 |
| SVC on Holter (%) |
8 (44.4) |
1 (2.5) |
< 0.001 |
| LA diameter (mm) |
34.7±4.9 |
31..5±6.9 |
0.15 |
| LA volume (ml/m2) |
31.5±6.9 |
36.1±6.1 |
0.003 |
LA: left atrium, DM: Diabetes Mellitus, SVC: supraventricular premature complex; HTA: hypertension; AT: atrial tachycardia. IC: ischemic cardiomyopathy; PVD: peripheral vascular disease.
In the univariate analysis, the following variables were predictive of AF: age > 65 years (HR 9.45 (CI 95% 1.25-71.34); p= 0.02), age as a continuous variable (HR for a 10-year increase in age 1.83 (CI 95% 1.15-2.92); p=0.01), CHA2DS2VASC score≥2 (HR 4.09 (CI 95% 0.93-17.87); p=0,06), left atrial enlargement (HR 2.29 (CI 95% 0.89-5.91); p=0.08) and presence of SVC on 24-hour Holter (HR 4.05 (CI 95% 1.55-10.57); p = 0.004), [Table 5].
Table 5. Univariate analysis.
|
HR (IC 95%) |
P value |
| Age> 65 years |
9.45 (1.25-71.34) |
0.002 |
| Age (10 years) |
1.83 (1.15-2.92) |
0.01 |
| Male sex |
0.49 (0.18-1.31) |
0.21 |
| HTA |
1.37 (0.47-3.92) |
0.54 |
| DM |
0.27 (0.03-2.07) |
0.12 |
| FOP |
0.33 (0.04-2.53) |
0.29 |
| Dyslipidemia |
0.69 (0.20-2.41) |
0.69 |
| CHA2DS2VASC≥2 |
4.09 (0.93-17.87) |
0.06 |
| LA enlargement |
2.29 (0.89-5.91) |
0.08 |
| AT on Holter |
2.01 (0.75-5.35) |
0.16 |
| SVC on Holter |
4.05 (1.55-10.57) |
0.004 |
LA: left atrium; DM: Diabetes mellitus; SVC: supraventricular premature complex; HTA: Hypertension; AT: atrial tachycardia.
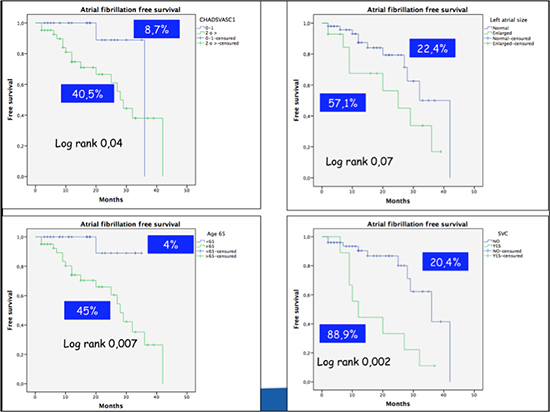
A CHA2DS2VASC score < 2 and age < 65 years showed a high negative predictive value (91.3% and 96%, respectively) to exclude the development of AF. Only 8.7% of patients with a CHA2DS2VASC score < 2 and 4% of patients under 65 years developed AF during the follow-up. On the other hand, presence of SVC on 24-hour Holter monitoring showed a high positive predictive value, detecting AF in 88.9% of these patients during the study period [Figure 4].
Figure 4. Atrial fibrillation-free survival curves according to CHA2DS2VASc score, age, left atrial size and presence of supraventricular premature complex (SVC). AF: atrial fibrillation
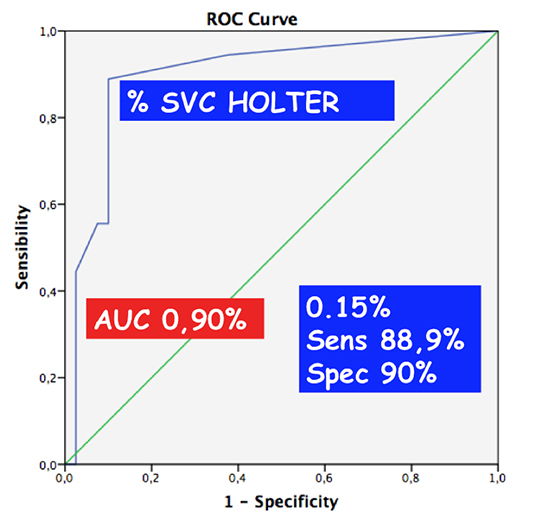
A ROC curve analysis was performed to find the optimal cut-point value of percentage of SVC, showing that figures over 0.15% on Holter monitoring had a sensitivity of 88.9% and a specificity of 90% to predict the development of AF [Figure 5].
Figure 5. ROC curve for the percentage of SVC on Holter monitoring. SVC: supraventricular premature complexes.
An Active search for AF in patients with ESUS is of vital importance, due to its clinical implications. American Heart Association and American Stroke Association guidelines for the prevention of stroke in patients with stroke and transient ischemic attack considers prolonged rhythm monitorin as reasonable (IIa) after acute ischaemic stroke or TIA with no other apparent cause[15]
If AF is detected, oral anticoagulation with acenocumarol or novel anticoagulants is highly recommended. Patients with paroxysmal, persistent or permanent AF exhibit a similar risk of stroke[14] and benefit from anticoagulation[16].
The main variable of the study was incidence of AF lasting at least 30 seconds. This definition is in accordance with guidelines[17] and although this is an arbitrary figure, it is a fundamental finding to assess the need for anticoagulation.
New generation ILR are equipped with remote monitoring technology. Devices are able to transmit daily diagnostic data and arrhythmic episode snapshots through a wireless receiver without any active patient or physician interaction. These transmission are reviewed by hospital staff and the time needed to adopt therapeutic measures is shortened.
In our study, AF was detected in 29.2% of patients which is in line with the results of the CRYSTAL AF study[9] (30%), though that study had a longer period of follow-up (36 months). In the CRYSTAL AF study, after an 18-month follow-up AF was detected in 17% of patients, a lower figure than the one found in our study where the mean follow-up was 17.1 ± 10.7 months. Baseline characteristics of both study populations were similar, with regard to hypertension (65.2% vs. 56.9%) and diabetes (15.4% vs. 15.4%). However, our patients were a bit older (65.4 ±13.8 vs. 61.6 ±11.4 years) compared to the ones included in the CRYSTAL AF study.
In the EMBRACE[10]study, AF was diagnosed in 16.1% of patients after a 90-day follow-up period. This high incidence of AF in a short period of time could be explained by the inclusion of an older population (mean age 72.5 ±8.5 years) and a higher rate of hypertensive (71.3%) and diabetic (19.2%) patients compared with our study and the CRYSTAL AF.
According to the results of our study, occurrence of AF in patients with ESUS is clearly determined by the presence of SVC and left atrial enlargement. Presence of SVC, defined as a quantity of SVC >1% of all heart beats analyzed during a 24-h Holter monitoring, was related to new-onset AF. This finding has been previously reported in the Cardiovascular Health Study[18] and in the Copenhagen holter study[19], where patients with a frequency of SVC over 30/hour or with 20 or more consecutive SVC had a higher incidence of AF, stroke or death. The findings of Johnson´s study[20], in which presence of SVC preceded AF, corroborate previous results. A cut-point of 0.15% for SVC showed high sensitivity and specificity values in our study, so that this figure could be taken into account to evaluate the risk of new-onset AF in that population.
Left atrial enlargement was also an independent predictor of AF, though with a lower impact than SVC. This factor is not only related with incidence of AF but also with risk of recurrence of AF after a rhythm control strategy using antiarrhythmic drugs, electrical cardioversion or pulmonary vein ablation[21]. In a study of hospitalized patients with AF, those with left atrial enlargement showed higher values of CHADS2 or CHA2DS2VASc scores than those with a normal left atrial size[22].
Two variables (CHA2DS2VASc score< 2 and age< 65 years) showed a very high negative predictive value for the absence of AF during follow-up. CHA2DS2VASc score includes the main risk factors for developing AF. In the study performed by Mitchell et al[23], where risk of stroke in a population naive of AF was analyzed according to CHADS2 and CHA2DS2VASc scores, incidence of new-onset AF was related to both scores and reached 3.85% in subjects with a CHADS2 score≥3 and 2.52% in those with a CHA2DS2VASc score ≥ 4. Therefore, high values of these scores identify a higher risk population for new onset AF, which in most cases may be asymptomatic. Similarly, the study by Chao et al[24] also reported that incidence of AF progressively increased with number of patients’ comorbidities, which are represented by the CHADS2 score. In our study, only 8.7% of patients with a CHA2DS2VASc score 0-1 showed AF during the follow-up. The combination of a CHA2DS2VASc score < 2 and age < 65 years could make the use of ILR less worthwhile in this low embolic risk population.
On the contrary, AF was detected in 40.5% of patients with a CHA2DS2VASc score ≥ 2, despite a relatively short follow-up period of 17 months, percentage that could be higher with longer periods of follow-up. This factor, in association with presence of SVC >1% (that showed a highly positive predictive value for AF), could create a point of controversy: the possibility of starting oral anticoagulant therapy in ESUS patients with a CHA2DS2VASc score ≥ 2 and with a certain burden of SVC on Holter monitoring, without the need of searching for hidden AF. In this sense, there are an ongoing clinical trials in patients with ESUS that analyze the routine use dabigatran - RE-SPECT ESUS, ClinicalTrials.gov Identifier: NCT02239120, trials.) and will probably give answers to this question.
Nonetheless, the evidence of a direct relationship between the detected episode of AF and embolic stroke is controverted. In fact, there are several monitoring studies, using pacemakers or defibrillators[25-26], in which risk of stroke is analyzed according to the presence or absence of AF. These studies show that there is not a temporal relationship between AF episodes and stroke, being arrhythmia episodes considered a risk marker more than a direct causative factor. In the study of Turakhia et al [27], only 13 over 187 acute ischemic stroke patients and continuous rhythm monitoring, had AF episodes longer than 5,5h in the 30 days before the event, compared to a period of 120-30 days before the stroke. However OR for stroke was highest in the five days immediately following and AF episode lasting at least 5,5h.
AF has been detected widely in patients with risk factors that were implanted with an ILR and had no previous AF documentation. AF was detected in 40% patients at 30 months[29], and at an incidence of 34,4% per person-year[30] in REVEAL AF trial and ASSERT II trial respectively. Almost 40% in REVEAL AF and 48% in ASSERT II had a previous history of stroke, TIA or embolism.
The main limitation of the present study is its small sample size. It was also a unicenter study and results may not be extrapolated to populations with other baseline characteristics.
AF episodes were documented by a Reveal registry that has only one derivation, and there is a remote possibility of having confused episodes of multifocal atrial tachycardia with AF.
AF algorithm of ILR are not the gold standard for heart rhythm monitoring as they are affected by false positive and false negative results[30].
We analyzed incidence of AF but not clinical response to initiation of anticoagulant therapy (reduction of recurrence after stroke). The small sample size and the absence of stroke recurrence in any patient during follow-up make this analysis undoable. However, that kind of study could be done in the future with a larger sample size.
Median time since stroke episode to ILR implantation was around 60 days. Incidence of new-onset AF may be higher during the first weeks after the ischemic event. An earlier (closer to ESUS episode) placement of the device could have provided a higher rate of AF.
Incidence of new-onset AF was 29.2% in our study population. Presence of SVC (>1% on 24-hour Holter monitoring) and left atrial enlargement were independent predictors of AF after an ESUS. SVC on Holter showed a high positive predictive value whereas age < 65 years and a CHA2DSVasC score < 2 showed a high negative predictive value for absence of AF.
The authors declare no conflicts of interest






