Impact of Atrial Low-Voltage Areas on The Acute and Long-Term Outcomes of Persistent Atrial Fibrillation Ablation
Grebmer C2*, Tatzber A2, Reents T2, Bourier F2, Semmler V2, Telishevska M2, Kottmaier M2, Buiatti A2*, Hessling G2, Deisenhofer I2, Ammar-Busch S12
1Klinikum Coburg, II, Medizinische Klinik, Coburg, Deutschland.2Deutsches Herzzentrum München, Klinik für Herz- uns Kreislauferkrankungen, Klinik an der Technischen Universität München, München, Deutschland.
Ablation in patients with persistent atrial fibrillation is associated with an increased risk of recurrence. One of the reasons for this is extended left atrial scarring, which can be identified as low-voltage areas (LVA) during left atrial mapping. To increase the success of ablation, these areas should be adequately identified to estimate the success of ablation based on a cut-off value.Therefore, this study aimed to show the relationship between left atrial voltage and the risk of recurrence for patients after ablation of persistent atrial fibrillation.
In this prospective study, 70 patients with persistent AF underwentablation using a modified stepwise approach. We compared two groups according to the Utah fibrosis criteria: the mild group, with left atrial LVA smaller than 20%, and the severe group, withleft atrial LVA of 20% or larger.Both groups were compared based on freedom from any atrial arrhythmia recurrence (>30 secondswith repeated 7-day Holterelectrocardiogram) at 12 months and the use of antiarrhythmic drugs.
All patients with atrial fibrillation converted to sinus rhythm by ablation (n=7) had a scar area smaller than 20%. All patients with LVA of 20% or larger were externally cardioverted to to sinus rhythm at the end of the procedure. LVA of 20% or larger tended to show increased recurrence rates after ablation (p= 0.058), significantly shorter periods before recurrence (p=0.041), anda trend toward even shorter periods before recurrence after repeat ablation (p=0.059).
The extent of left atrial LVA influences the acute and long-term outcomes of persistent atrial fibrillation ablation. Patients with LVA smaller than 20% could benefit from a stepwise approach.
Key Words : .
Christian GrebmerDepartment of Electrophysiology, German Heart Center MunichMunich, Germany
Forpatients with paroxysmal atrial fibrillation (AF), pulmonary vein isolation (PVI) is the therapy of choice because of its high success rate ranging from 60% to 85% and freedom from recurrence within 1year1. However, for patients with persistent AF,the successrates in terms of stable restoration of sinus rhythm are reduced to 42% to 60% 2,3. Furthermore, patients with long standing persistent and persistent AF havesignificantly lower success rates with PVI andhigh recurrence rates of AF or any atrial tachycardia (AT) up to 68% within 1year4,5,6. Additionally, patient age, comorbidities, genetic predisposition, atrial size, and AF duration also have important roles in the success of PVI7. Different ablation techniques have different advantages and disadvantages and are variably applied8. Methods such as complex fractionated atrial electrogram ablation, rotor ablation, and linear lesion ablation, which are based on PVI, have not shown clearly superior results compared to PVI during previous studies8. However, the “philosopher’sstone” for the optimal treatment of persistent AF has not yet been found.Becauseneither linear lesions nor electrogram-guided ablation in addition to PVI have resulted in significantly better outcomes8, a combined approach or an individualised approach could be beneficial.
This study proposed a novel predictor of outcomesafter ablation of persistentAFin patients with left atrial (LA) low-voltage areas and the corresponding clinical implications for the affected patient population.
During February 2012 to January 2014, a total of 70 consecutive patients with persistent (49%) or long-term and persistent AF (51%) were included in a prospective registry study. Follow-up was performed until January 2015. The average age of the patients at the time of intervention was 62.8±9.8 years (minimum, 39.3 years; maximum, 85.7 years). The average body mass index was 27.73±3.90 kg/m2 (minimum, 19.81 kg/m2; maximum, 38.28 kg/m2). The proportion of male patients was 80.0% (n=56). Persistent AF was defined as AF for more than 7 days with or without prior cardioversion. For long-standing persistent AF, the period was defined as more than 12 months of continuous AF. All patients provided written consent.
All anti arrhythmic drugs except beta-blockers were discontinued for at least 4 weeks before the ablation procedure. Computed tomography or magnetic resonance imaging was performed before the planned procedure to visualise the anatomy of the atria. The LA thrombus was ruled out using computed tomography or transoesophageal echo cardiographyas described previously2.
Examination and ablation procedures
Anticoagulation for at least 4 weeks before ablation was required. Antiplatelet therapy was maintained during the procedure. Continuous novel oral anticoagulants such asrivaroxaban, dabigatran, apixaban, or vitamin K antagonists (phenprocoumon) were used with a target international normalized ratio of 2.0 to 2.8 during the procedure. These oral anticoagulants were continued on the day of the procedure. Periprocedural management and postprocedural management of oral anticoagulation werebased on in-house standards.
All patients presented forablation withongoing AF. After accessing the left atrium, electroanatomical mapping was performed with a circular steerable mapping catheter (14 Bipole Orbiter® PV;C. R. Bard, Lowell, MA, USA) under the guidance of an electroanatomical mapping system (EnSite Velocity NavX; Abbott Medical Inc., St. Paul, MN,USA). LAmaps were recorded in AF. Bipolar endocardial signals were filtered from 30 to 300 Hz. All acquired electromyograms were subsequently visually inspected to ensure homogeneous distribution of measurement points across the LA assuming a minimum map density of 500 points for each LA map. The mapping points were measured after 5 seconds with a stable catheter. A steerable bidirectional sheath (Agillis sheath;Abbott Medical Inc., St. Paul, MN, USA) was used to allow contact with and positioning of the mapping catheter in all positions. The surface colour projection included an interpolation threshold of 8 mm and a minimum colour temperature. The map density was ensured in all parts of the LA. Bipolar endocardial signals with a mean voltage less than 0.1 mV were defined as scarring3,9,10.
The ablation strategy was performed according to a modified stepwise approach. Circumferential PVI was performed as the first step. After successful PVI, electrogram-guided ablation of sites with voltage between 0.1 and 0.5mVwas performed successively in the left atrium, right atrium, and coronary sinus. In case of occurrence of macroreentries, linear lesions were deployed: a roofline was used for roof-dependent atrial flutter;an anterior line was used for perimitralatrial flutter; and a cavotricuspidal line was used for atypical atrial flutter. Localised reentries were ablated focally. Further details of the ablation strategy and its endpoints have been described previously 2,11.
The endpoint of ablation was the conversion to sinus rhythm by ablation, whether via external cardioversion or ablation.Before external cardioversion could beperformed,exit and entrance blockage (pulmonary veins) had to be present,blockage across drawn lines had to be confirmed, and local electrograms had to be ablated.
After the procedure, a 3-month course of anticoagulants was prescribed, which was subsequently re-evaluated after 3 months using the CHA2DS2 VASc score and continued or discontinued if necessary
The follow-up duration was 12 months after the first ablation. Atrial arrhythmia (AF or AT) recurrence was evaluated after 3, 6, and 12 months via in-person outpatient visits at the follow-up outpatient clinic or by the patients’ general practitioners. During the examinations, the physician evaluatedthe medical history and focused particular attention onpersistent or recurrent palpitations and arrhythmias. A Holterelectrocardiogram was performed at each examination for 7 days.
The first 2months after ablation have been defined as a blanking period,and recurrences thatoccurred during that period were notnoted. The blanking period was defined by an in-house standard.If relapse occurred after the blanking period, then the time and type of the relapse arrhythmia were evaluated. The number and type of repeat ablation procedures were noted.
Electroanatomical map analysis
After the procedure, the electroanatomical maps that were created were analysed by a second investigator. The total mapped atrial surface area and low-voltage area were measured based on the electrode size and interelectrode spacing of the introduced catheters (field scaling). Two groups of patients were defined: group 1, with a low-voltage areasmaller than 20%, and group 2,with a low-voltage areaof 20% or larger.
Statistical data evaluation
The descriptive and inferential statistical data analyses were performed using SPSS Statistics 22 (IBM®) for Mac OSX. The significance level was determined in advance at 5% according to the probability of error; therefore, a result within the framework of the hypothesis-testing tests with p≤0.05 was considered significant.
To describe the characteristic values of metric parameters, mean values and standard deviations as well as minimum and maximum values were determined. Additionally, the median alternative position measurement was used for oblique measurement distribution of a parameter. Descriptive statistics were used to determine the frequencies and their corresponding proportional values for categorical variables. To show the range in which the true value was in the population, the corresponding confidence interval (CI) was determined.For the 5% error probability of the CI, acorresponding two-sided z-value of 1.96 was used, whereby the interval limits were calculated by taking into account the relative frequency of the probability based on the sample value.
As part of the inferential statistical tests, mean value comparisons of metric parameters were performed using the Welch t test for independent samples.The Mann Whitney Utest was used as a parameter-free alternative to the ttest for independent samples in the case of obliquely distributed data. These inferential statistics evaluated the differences between the two samples based on the least ranked data (i.e., an ordinal scale level was assumed).
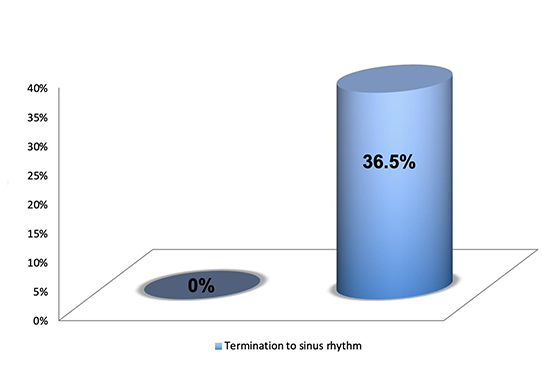
For all patients with sinus rhythm that could be achieved by ablation (n=7), the scar area was smaller than 20%. In the group withlow-voltage areasof 20% or larger(n= 19), sinus rhythm could not be achieved by ablation. The ablation parameters did not differ significantly between groups (p>0.05)([Table 1] & [Table 2]).
Table 1. Baseline characteristics
|
LVA <20% (n=52) |
LVA ≥20% (n=18) |
P-value |
| Age (years) |
60 (±9.2) |
70.7 (±7.0) |
<0.001 |
| BMI |
27.91 (±4.05) |
27.21 (±3.49) |
0.520 |
| Male (n) |
86.5 % (45) |
61.1 % (11) |
0.037 |
| Arterialhypertension |
61.5 % (32) |
83.3 % (15) |
0.145 |
| CAD |
11.5 % (6) |
22.2% (4) |
0.268 |
| DM II |
17.3% (9) |
11.1% (2) |
0.716 |
| Pacemaker |
13.5 % (7) |
27.8 % (5) |
0.274 |
BMI, body mass index; CAD, coronary artery disease; DM II, type 2 diabetes mellitus; LVA, lowvoltage area.
In the present patient population, 66 experienced recurrenceduringthe blanking period. A totalof 43 (65.2%) of the 66 patients were affected by relapseof any atrial arrhythmia (AF or AT) for more than 30secondswhen not usingantiarrhythmic drugs. Of these 43 patients, 28 patients (58.3%) were in group 1 (28 of 48 in group 1) and 15 patients (83.3%) were in group 2 (15 of 18 in group 2)(p=0.058). The Kaplan Meier curve revealed a significant difference in terms of recurrence rates for AF and AT between the groups withlow-voltage areas smaller than 20% and low-voltage areas of 20% or larger (p=0.04) within 1year [Figure 1].The test of the distribution difference regarding the incidence of recurrence depending on the low-voltage area showed an overall trend toward a higher recurrence rate for patients with lowvoltage areas of 20% or larger (x² (1)=3.604;p=0.058).
Figure 1. Kaplan Meier curves indicating noatrial fibrillation (AF)/atrial tachycardia (AT) recurrence after single ablation (%) without antiarrhythmic drugs (AAD).LVA, low-voltage area.
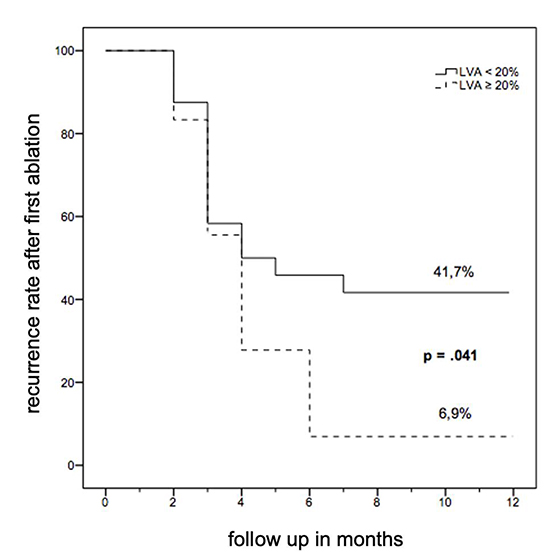
For patients with low-voltage areas smaller than 20%, a longer interval without recurrence can be expected. The median recurrencefree time for low-voltage areassmaller than 20% was 6.96 months (95% CI, 5.72-8.20 months)and that forlow-voltage areasof 20% or largerwas 4.36 months (95% CI, 3.14-5.58months).
Table 2. Procedural data
|
LVA <20% (n=52) |
LVA ≥20% (n=18) |
P-value |
| Age (years) |
60 (±9.2) |
70.7 (±7.0) |
<0.001 |
| BMI |
27.91 (±4.05) |
27.21 (±3.49) |
0.520 |
| Male (n) |
86.5 % (45) |
61.1 % (11) |
0.037 |
| Arterialhypertension |
61.5 % (32) |
83.3 % (15) |
0.145 |
| CAD |
11.5 % (6) |
22.2% (4) |
0.268 |
| DM II |
17.3% (9) |
11.1% (2) |
0.716 |
| Pacemaker |
13.5 % (7) |
27.8 % (5) |
0.274 |
BMI, body mass index; CAD, coronary artery disease; DM II, type 2 diabetes mellitus; LVA, lowvoltage area.
Sixty-six patients completed 12 months offollow-up.Thirty-five patients (53%) required either a single ablation procedure or multiple repeat ablation procedures: 26 (39.4%) required a single ablation procedure, 6 (9.1%) required a second ablation procedure, and 2 (3%) required a third ablation procedure.
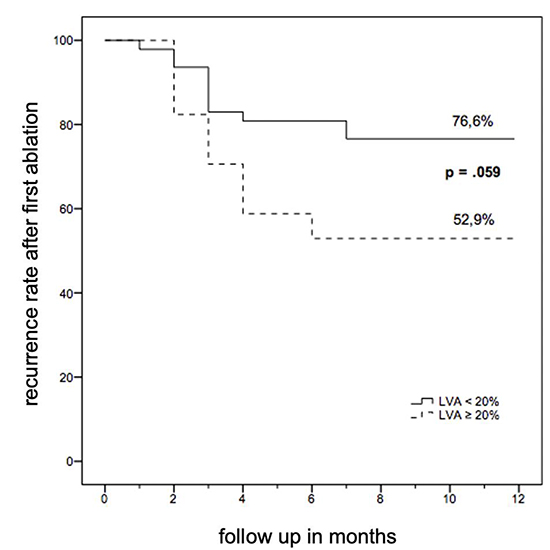
The log-rank comparison (Mantel-Cox) of event distributions showed a trend toward (x²(1)=3.554; p=0.059) longer recurrence-free times after repeat ablation for patients with low-voltage areassmaller than 20%.The mean absence of recurrence for low-voltage areassmaller than 20% after repeat ablation was 10.00 months (95% CI, 8.94-11.07 months),and that forlow-voltage areasof 20% or larger was 7.88 months(95% CI, 5.76-10.00months) [Figure 2].
Figure 2. Kaplan Meier curves indicating noatrial fibrillation (AF)/atrial tachycardia (AT) recurrence after repeat ablation. LVA, lowvoltage area.
The main finding of this study was that low-voltage areas of 20% or largerin the LA impact the acute and long-term outcomes of patients with persistent or long-term and persistent AF, as shown by their high rate of recurrence during follow-up. It is of importance that the atrial voltage was measured in AF and not in sinus rhythm, which, according to Qureshi et al., provides significantly better data regarding atrial voltage 10.
Figure 3. Acute outcomes after ablation.Periprocedural conversion to sinusrhythm during ablation.
The patient population was divided according to the Utah fibrosis classification to analyse the influence of the extension of scar areas. The Utah classification assumes worsening of the prognosis starting from grade 3,resulting in a separation value of 20% for the two patient groups12.
Voltage maps were recorded in AF, andthe mean voltage was evaluated during a period of 5 seconds. This method was described previously 3.In contrast to the ventricle, where the scar cutoffis clearly defined, scar definition in the atrium has been less well-evaluated. Considering the possible prognostic impact of low-voltage areas, as defined by our study, scarring can be evaluated in AF using a cutoff of 0.1mV.Restoration of sinus rhythm seems to be important to the risk of early recurrence and late recurrence. Depending on which approach is chosen, the risk of provoking AT remains. PVI has been proven to be an effective method of rhythm controlin paroxysmal AF 12,13. For patients with persistent AF, only moderate success can be achieved with PVI alone2,3,14,15. During follow-up, only 20% of patients did not experience recurrence 5 years after a single ablation. With multiple ablations, this rate increases to 45% 16,17. To improve the results of ablation for persistent AFusing targeted substrate modification, different approaches can be pursued. Relevant strategiesinclude linear lesions, atrial defragmentation,or both in combination 3. The randomised, multicentre STAR AF II study demonstrated that substrate modification with PVI compared to PVI alone did not result in any benefitsforpatients who underwent ablation forpersistent AF. Atrial arrhythmia withoutantiarrhythmic drugs after a single procedure was possible after PVI alone for 41%, after PVI with complex fractionated atrial electrogram ablation for 33%, and after PVI with linear lesions for 29%8. These results suggest that none of these approaches is optimal. Therefore,there is no clear recommendation regarding substrate ablation. Moreover,it has been suggested that extensive ablation may result in iatrogenically induced arrhythmogenic areas, such as incomplete ablation or incomplete linear blockage18–20.
A large portion of our study population had long-termandpersistent AF, and the ablation outcomes of a modified stepwise approach using two procedures wererelatively good for patients with small low-voltage areas. However, the high recurrence ratesof the group with largerlowvoltage areas suggest that a different ablation strategy is necessary. Further approaches such as box isolation of low-voltage areasor an individualised approach with limited ablation at the borders of lowvoltage areas21,22,23 have been described. The present results highlight the need to identify critical structures of persistent AF to achieve success through individualised ablation strategies.
During our study, we used the automated NavX® cycle length algorithm (NavXsystem automated algorithm of cycle length) to define low-voltage areas. It cannot be excluded that different results might have been achieved with a different mapping system and different automated algorithms. LA scar characterisation by bipolar voltage mapping remains poorly defined. For maps acquired during ongoing AF, a cutoffless than 0.1 mV is considered appropriate fortracing LA scar distribution. However, the extent to which LA scarring can be identified using electroanatomical mapping during AF requires further investigation. The present study shows a statistically significant reduction only in the rate of recurrence. Other results only showed tendencies toward statistical significance. Of course, this is attributable to the very small number of patients.
Current mapping systems can measure atrial voltage even more precisely because of progress in technology and the further development of ablation and mapping catheters.Therefore, evaluation susing new technology could be of great relevance to the further development of ablation strategies.
Our study shows that the extent of LA low-voltage areas influences the acute and long-term outcomes of persistent AF ablation.Patients with low-voltage areas of 20% or larger have significantly worse outcomes after single ablation; however, they might benefit from other ablation methods. Patients withlow-voltage areas smaller than 20%could benefit from a modified stepwise ablation approach.
Christian Grebmer: main author, drafting article, approval, correspondence, concept and design, statistics.
Sonia Ammar- Busch: senior author, concept and design, fundings critical revision, approval of the article, statistics.
All the other authors: critical revision, data collection, concept and design.






