Same Day versus Overnight Discharge in Patients Undergoing Ablation for Atrial Fibrillation (SODA) Study
Som Aftabi Bailey1, Karthik Subramanian1, Javier Sanchez2, Rodney P. Horton2, Andrea Natale2, Senthil Thambidorai12
1Medical City Fort Worth.2Texas Cardiac Arrhythmia.
Patients undergoing catheter ablation for atrial fibrillation (AF) are routinely admitted for observation overnight in the hospital. With the rising incidence of AF among the population, increased volumes of procedures are placing increased demands on hospital resources. The purpose of this study was to evaluate the efficacy and safety of same day discharge in patients undergoing ablation for AF when compared to patients admitted for overnight observation. We performed a retrospective analysis using a multicenter cohort among patients who were discharged home after elective pulmonary vein isolation (PVI) ablation for AF. In our analysis, we found no statistically significant difference between patients discharged on the day of their procedure when compared to patients admitted for overnight observation in terms of 90-day readmission, major adverse cardiovascular events and death. This study shows that same day discharge after AF ablation is a feasible option. Future studies are needed to elicit the appropriate protocol to use.
Key Words : .
Aftabi Bailey, 900 8th Ave, Fort Worth, TX 76104
Atrial Fibrillation (AF) is the most commonly diagnosed cardiac arrhythmia, with an estimated 6.1 million cases in the United States and is expected to double by 2030 1. Catheter ablation for AF is a common procedure performed to scar or eliminate the triggers that cause AF. It is an effective treatment and has been shown to be superior to antiarrhythmic therapy in patients with symptomatic AF. With continued advancement in pulmonary vein (PV) ablation, procedural outcomes have seen tremendous improvement while complications have gone down significantly These factors have led to an increased number of AF ablation procedures being performed 2-4.
It is common practice and expert medical consensus to keep patients overnight in the hospital after an AF ablation procedure. However, the inpatient costs are extremely high and the increased number of procedures being performed place increased demand on the healthcare system 5. Furthermore, the emergence of the COVID-19 pandemic has greatly affected health care delivery worldwide. A massive reallocation of health care resources has created major obstacles to routine medical care in addition to the need to limit disease transmission as infected patients fill hospital beds. As a result, research is being done to evaluate more cost-efficient models of post-ablation care without compromising the quality of the current practice or risking further complications in patients. This has led to research being performed on the efficacy and safety of early or same-day discharge after AF ablation. Research has already been performed showing same-day discharge is safe and effective for less complex ablations such as atrial flutter. AF ablation is generally a more complex procedure with longer sedation times and higher levels of anticoagulation 6-7.
The purpose of this study is to examine the potential relationship between patients undergoing AF ablation being discharged on the same day versus the standard overnight hospital admission.
This is a retrospective multicenter cohort study among patients who were discharged home after elective pulmonary vein isolation (PVI) ablation for AF at hospitals and surgical centers in the United States run by Hospital Corporations of America (HCA) between January 2015 and December 2018. All outpatient procedures in adults over 18 years of age were included. Patients who were inpatient or were hospitalized over 48 hours were excluded.
Inclusion Criteria:
. Age > 18 years
. Outpatient PVI ablation
. Hospital stay <48 hours.
Exclusion Criteria
. An inpatient stay prior to the procedure
. Hospital stay > 48 hours post-procedure.
Using the above-mentioned inclusion-exclusion criteria, patient encounters were pulled by data analysts using CPT codes for PVI ablation. Patient encounters that met the exclusion criteria were eliminated and resultant encounters were used for the study. 17,724 ablation procedures were pulled from HCA’s electronic data warehouse. 14,290 of these patients underwent PVI ablation on the day they presented to the hospital. Admissions < 48hours were randomly selected from these patients leaving a patient population of 13,567 patients.
Patient data included patient demographics, date of admission, date of discharge and home medications. Limited medical history was obtained through ICD 10 codes. Readmission at 90 days was evaluated by reviewing the patient encounters and matching with the patient account number (e.g., if the same account number had a second encounter within 90 days after the date of the procedure, it qualifies for all-cause readmission). Principal and sub investigators were blinded and provided with de-identified data only [Table 1].
Table 1. Patient Encounters
|
Number of Patient Encounters |
| Same-day discharge |
1255 |
| Overnight stay |
12312 |
| Total |
13567 |
Table 1 table 1
The resultant data was entered into SPSS software for analysis. Logistic regression analysis was made to evaluate for 90-day readmission rates. Multiple logistic regression was performed for both 90-day all cause readmission and 90-day AF readmission. Variables included in the model are overnight status, age, sex, race (white/other), hypertension without CKD, hypertension with CKD, CHF, diabetes type II, anticoagulants, antiplatelets, rate control medications, and rhythm control medications.
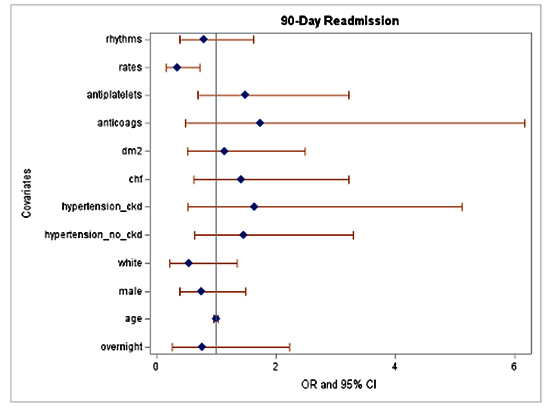
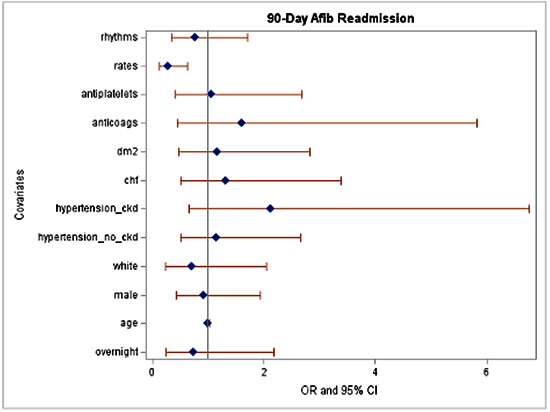
There was no statistically significant difference in mortality, major adverse cardiovascular events, 90-day all-cause readmission or 90-day AF readmissions. A logistic regression analysis was performed and found no statistically significant difference between patients who were admitted overnight when compared to patients discharged on the same day as their AF ablation in terms of 90-day all-cause readmission and 90-day AF readmission. In a subgroup analysis, there was a statistically significant decrease in 90-day all-cause readmission in patients discharged on rate lowering medications versus those who were not (p-value 0.005, OR 0.358, 95% CI 0.175-0.734) [Table 2]-[Table 3]-[Table 4].
Table 2. Patient Distribution
|
Same-day discharge (N=1255) |
|
Overnight Stay (N=12312) |
|
|
Yes |
No |
% |
Yes |
No |
% |
| Mortality |
1 |
1254 |
0.08 |
4 |
12308 |
0.03 |
| 90-day all-cause readmission |
5 |
1250 |
0.4 |
31 |
12281 |
0.25 |
| 90-day AFib readmission |
5 |
1250 |
0.40 |
24 |
12288 |
0.20 |
Table 2 table 2
AF is the most prevalent cardiac arrhythmia in clinical practice. The incidence and prevalence of AF are expected to increase drastically over the next decades, further increasing procedural volumes for AF ablation and hospital demand. Catheter ablation for AF is the most common ablation procedure and typically requires at least one overnight hospital stay 8-10. The new burdens placed upon the healthcare industry by the COVID-19 pandemic have further compromised the delivery of these procedures for many institutions worldwide. Given the current state of the COVID-19 pandemic, many institutions have elected to reduce non-urgent procedures to preserve resources, reduce viral transmission and maximize hospital capacity. A model of same day discharge for patients undergoing ablation for atrial fibrillation may play an important role in the post-surge period as well as throughout seasonal pandemic fluctuations in the future.
Census projection estimated approximately three million individuals in the U.S. with a diagnosis of AF in 2020, with a projected increase to ~5.6 million people by 2050 11. With the growing number of diagnoses, AF ablation procedures have continued to rise with a decrease in complications. Thus far there is no standardized recommendation regarding discharge time after catheter ablation. Historically, the majority of centers have and many still admit patients for at least one overnight stay following AF ablation procedures 12-15. A same day discharge approach can not only improve patient experience and satisfaction, but it can reduce the burden on our healthcare system and cut down on unnecessary healthcare costs.
Table 3. 90-day All-Cause Readmissions
|
Adjusted Odds Ratio |
95% CI |
P-value |
| Overnight |
0.771 |
0.266-2.238 |
0.633 |
| Age |
0.994 |
0.962-1.026 |
0.709 |
| Male |
0.754 |
0.385-1.477 |
0.411 |
| HTN/no CKD |
1.472 |
0.653-3.315 |
0.351 |
| HTN/CKD |
1.724 |
0.557-5.334 |
0.344 |
| CHF |
1.433 |
0.632-3.246 |
0.389 |
| DM 2 |
1.178 |
0.539-2.577 |
0.682 |
| Anticoagulant Medication |
1.732 |
0.487-6.154 |
0.396 |
| Anti-platelet Medication |
1.472 |
0.684-3.167 |
0.322 |
| Rate Control Therapy |
0.358 |
0.175-0.734 |
0.005 |
| Rhythm Control Therapy |
0.805 |
0.398-1.629 |
0.545 |
There are a growing number of studies investigating same-day discharge. Deyell et al reported on over 3,000 patients at two centers in Canada undergoing same-day discharge for AF ablation. In their study, the primary reason for later discharge were access site problems, intraprocedural complications, late procedure times, and complications related to anesthesia 13-19. Other studies have shown up to 80% of patients undergoing AF ablation may be amenable to same-day discharge if avoidable delays in care and complications had been anticipated. Many studies were conducted at single centers and have used protocols and patient selection when addressing same-day discharge 20-25. Our study is unique in that it was conducted across multiple centers across the nation and no patient selection or protocols were implemented. Despite this, our results still showed no significant difference in mortality, MACE, or 90-day readmission in patients undergoing PVI ablation for AF when discharge on the same day as the procedure.
This retrospective multicenter cohort study among patients who were discharged home after elective PVI ablation for AF showed that same-day discharge was not associated with a statistically increased rate of morbidity, mortality, or 90-day readmission rates. In fact, our subgroup analysis showed that being on rate control medications may have a higher impact on readmission than same day discharge. We included this subgroup along with patients on rhythm control medications to be included in our logistical regression analysis to control for confounding variables. Interestingly, being on rate control and not rhythm control was associated with a decrease in readmission rates.
Same day discharge after AF ablation has the potential to reduce healthcare utilization, increase patient satisfaction and lessen the cost per patient encounter. Delivering cost effective healthcare while not compromising the quality of care should be of utmost importance. This study should provide more data reassuring that same-day discharge is safe for the majority of patients undergoing AF ablation. Future research regarding the design of specific protocols and the optimal patient selection are needed.
Table 4. 90- Day AF Readmission
|
Adjusted Odds Ratio |
95% CI |
P-value |
| Overnight |
0.736 |
0.248-2.183 |
0.58 |
| Overnight |
0.999 |
0.975-1.024 |
0.949 |
| Male |
0.91 |
0.427-1.94 |
0.807 |
| HTN/no CKD |
1.148 |
0.498-2.645 |
0.745 |
| HTN/with CKD |
2.171 |
0.684-6.894 |
0.188 |
| CHF |
1.323 |
0.515-3.398 |
0.56 |
| DM 2 |
1.187 |
0.49-2.878 |
0.704 |
| Anticoagulant Medication |
1.602 |
0.441-5.819 |
0.474 |
| Anti-platelet Medication |
1.036 |
0.405-2.649 |
0.941 |
| Rate Control Therapy |
0.276 |
0.12-0.638 |
0.003 |
| Rhythm Control Therapy |
0.767 |
0.344-1.71 |
0.516 |
Discharging patients on the same day after the AF ablation procedure is not a common practice. Due to this, our study is limited to an unevenly low distribution of patients who were discharged on the same day. It also affected the distribution of patients based on various demographics. This is a multicenter study involving patient encounters in hospital settings and hospitals. Due to this, there are various confounding factors like operator skill, lab facility, post-operative care management, recognition of immediate complications and follow up care. Regarding decreased readmission in patients on rate control therapy, we included this subgroup along with patients on rhythm control medications to be included in our logistical regression analysis to control for confounding variables. Interestingly, being on rate control and not rhythm control was associated with a decrease in readmission rates. This may be because patients on rhythm control had more refractory or medication-resistant atrial fibrillation. The study was also not specifically powered to look at rate vs. rhythm control, so results should be interpreted with caution.
Our study adds to the growing amount of evidence pointing to the safety and efficacy of same day discharge in patients undergoing AF ablation. Further studies are warranted investigating factors that place patients at increased risk for adverse events at same day discharge.






