Protocol for catheter ablation
Anti-arrhythmic drugs (AADs) were discontinued for ≥5 half-lives prior to ablation. Oral anticoagulant therapy was initiated at least 1 month prior to the procedure.
In the first procedure, the protocol was as follows: the first circumferential PVI and ablation of the carina were performed [Figure 1A]; Left atrium (LA) mapping during right atrium (RA) pacing was conducted to confirm PVI [Figure 1B]; roof and bottom linear ablation was performed for PWI [Figure 1C]; and lastly, when linear ablation failed to complete PWI, intra-box ablation was added [Figure 1D].
Figure 1. An example of PVI and PWI.
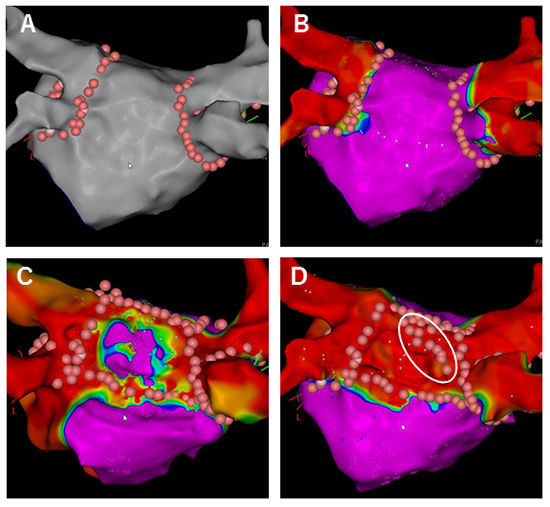
These figures show the procedure of PVI and PWI. A) First, PVI is performed. B) After PVI, LA mapping during RA pacing is performed to confirm PVI. This map is analyzed after the procedure. C) Linear ablation for PWI is performed. When compete PWI is not achieved, posterior wall mapping is performed. D) In this case, intra-box ablations (in white circle) are required to achieve complete PWI. After PWI, posterior wall mapping is performed again to confirm endpoints.
The electrophysiological study and ablation were performed under deep sedation, using an intravenous administration of propofol. A 20-polar superior vena cava (SVC)-RA-coronary sinus (CS) electrode catheter (BeeAT, Japan Lifeline, Tokyo, Japan or Inquiry, Abbott, Abbott Park, Illi, USA) was inserted via the right subclavian vein into the coronary sinus. The PVs and LA were mapped using a multielectrode mapping catheter (PentaRay, Biosense Webster, Diamond Bar, CA, USA) and a three-dimensional anatomical mapping system (CARTO, Biosense Webster). A 3.5-mm irrigated-tip catheter (ThermoCool Smart touch SF, Navistar, BiosenseWebster) was used for ablation. PVI was performed using a circular mapping catheter (Lasso, Biosense Webster) placed within the ipsilateral ostia of the superior and inferior PVs. The endpoint of PVI was the achievement of a bidirectional conduction block between the LA and PVs. After PVI, cardioversion was delivered to restore sinus rhythm. LA mapping was conducted by multielectrode catheter (PentaRay, Biosense Webster) during high RA pacing (basic cycle length, 600 msec), and then PWI was conducted.
During PWI, the PentaRay was placed at the PW to record its electrical potential. Roof line and bottom line ablation were conducted to achieve PWI. After linear ablation, LA mapping was conducted to confirm isolation of the PW. The area under 0.05 mV was defined as the scar area. The endpoint of PWI was defined as the absence of electrical activity in PW, and the inability to conduct from posterior wall to LA, which was confirmed by 5 mA output pacing from PentaRay at PW. Automaticity and local capture recorded by the PentaRay in the PW were also supportive findings of complete PWI.
When PWI was incomplete after linear ablation, PW mapping was performed to search for the gap. In case the propagation map showed excitement traversing the gap to the PW, the gap was ablated. When the gap ablation failed to complete PWI or the gap was unclear, applications in the “box” area, which were defined as intra-box ablation, were conducted. The intra-box area was defined as the area surrounded by the roof and bottom line with a margin of 4-mm. The area with electrical activity was ablated. In this case, the endpoint was the absence of electrical activity captured by high output pacing with 20 mA; if pacing was captured, ablation was added until pacing was not captured.
Radiofrequency (RF) energy was applied point-by-point, and the setting differed per term as [Table 1] shows.
Table 1. Radiofrequency energy settings
|
PVI except for posterior PVs |
posterior PVs |
PWI roof line |
PWI bottom line |
| from Jun 2017 to Mar 2018 |
30 W, 30 sec |
25 W, 30 sec |
30 W, 30 sec |
25 W, 30 sec |
| From Mar 2018 to Jan 2020 |
40 W, AI 500 |
30W, AI 450 |
40 W, AI 500 |
30W, AI 450 |
| From Feb 2020 to Mar 2020 |
50 W, AI 500 |
50 W, AI 400 |
40 W, AI 500 |
30W, AI 450 |
AI, ablation index; PVs, pulmonary veins; PVI, pulmonary vein isolation; PWI, posterior wall isolation; sec, seconds.
The esophageal temperature was monitored using CIRC-S-CATH (CIRCA Scientific, Englewood, CO, USA), and application was abandoned when the temperature was over 41℃.
After confirming the achievement of endpoints, we administered a bolus injection of 20 mg of adenosine triphosphate (ATP) to exclude ATP-provoked dormant conduction of PVs and PW. Catheter ablation was performed to eliminate the presence of reconnection and/or dormant conduction.
LA mapping was performed after PVI and before PWI during RA pacing by a SVC-RA-CS electrode catheter in most patients, and LA mapping data were analyzed after the procedure. LA mapping was abandoned in cases of ongoing AF after cardioversion and the inability to stabilize RA pacing. Box area was defined as the area surrounded by PVI, roof, and bottom lines. Voltage was measured in the para-line area, which was defined as the area of the roof and bottom line with a margin of 4-mm above and below, and the intra-box area was defined as the “box” area excluding the para-line area. Total activation time of the box area were measured. Activation time reflects how much time the excitement takes to propagate to the whole PW.
CARTO version 7’s propagation map and vector map were used to observe the conduction pattern of the PW. The cycle length of the vector map was set to the LA activation time in the propagation map. The excitatory wave front is highlighted in the propagation map; the vector map follows the propagation path of an excitatory wave front.
After undergoing PVI and posterior isolation, patients were discharged from the hospital with a prescription for oral anticoagulants. The use of AADs could be discontinued three months after ablation, at the physician’s discretion. The rhythm and presence of arrhythmias were evaluated based on the patient’s symptoms and a resting 12-lead electrocardiogram, which was recorded during regular visits to our outpatient clinic. To detect AF recurrence and atrial tachyarrhythmia, we performed a 24-h Holter monitoring at 1, 3, and 6 months after the first procedure. AF recurrence was defined as AF and other atrial tachyarrhythmias documented lasting longer than 30 seconds regardless of AADs usage. The blanking period was three months, and AF recurrence was evaluated until 6 months after the first procedure.
Patients underwent a follow-up electrophysiological study and additional ablation for PV reconnection, PW reconnection, and/or non-pulmonary vein foci, if present as the second procedure, 6 months after the first procedure, regardless of AF recurrence. All patients were eligible for the second procedure except for those who rejected it. PV and PW reconnection were evaluated by LA mapping and catheters positioned in the PW and PVs, respectively. When there was PV and/or PW reconnection, applications for gaps were conducted after sites of gaps were searched by using propagation map. After applications for gaps failed to achieve PW re-isolation, intra-box ablation was added. Procedural endpoints were same as the first procedure.
Primary outcomes were findings of LA mapping after PVI before PWI in the first procedure, such as PW voltage, activation time, and propagation/vector map pattern, abundant applications because of esophageal temperature rise, and reconnection of PW in the second procedure. Secondary outcomes were reconnection of PVs in the second procedure and AF recurrence at six months after the first procedure.
Outcomes and patient characteristics were compared between patients with intra-box ablation and without intra-box ablation (intra-box group vs non-intra-box group).






