What is the Impact of Frailty on Prescription of Anticoagulation in Elderly Patients with Atrial Fibrillation? A Systematic Review and Meta-Analysis
Zardasht Oqab1, Payam Pournazari1, Robert S Sheldon1
1Libin Cardiovascular Institute of Alberta, University of Calgary, Calgary, Alberta, Canada
.
Atrial fibrillation (AF) and frailty are both associated with advanced age. Oral anticoagulants (OAC) effectively prevent strokes in AF patients but are underutilized in the elderly, possibly due to misperception of frailty.
We performed a systematic review to determine the prevalence of frailty in patients with AF, and whether frailty was associated with reduced prescription of OAC.
We systematically searched Cochrane, MEDLINE, EMBASE, and PubMed databases. Search terms combined relevant words and MeSH headings: 1) atrial fibrillation, 2) frail elderly, and 3) geriatric assessments. Studies that measured frailty using a validated instrument, and involved OAC for AF in frail and non-frail patients were eligible for inclusion. Pooled odds ratios were calculated using random-effects model.
Of 166 reviewed titles, only 3 studies (1204 patients) met the inclusion criteria. Two used the Reported Edmonton Frail Scale (total 509 patients), and one used the Canadian Study of Health and Aging Clinical Frailty Scale (682 patients). All 3 studies involved hospitalized patients with an average age of 85 ± 6 and 45% were male. The weighted mean prevalence of frailty in patients with atrial fibrillation was 39% (95%CI 36-42). The weighted mean rate of OAC use was 57±11%. Frailty was associated with non-prescription of OAC compared to non-frail (OR 0.49, 95% CI 0.32-0.74, I2 =45%).
The prevalence of frailty in hospitalized elderly patients with AF is high, and the use of OAC is low in these patients. Frail elderly are significantly less likely to receive OAC.
Key Words : Atrial fibrillation, Elderly, Frail, Anticoagulation Prescription, Stroke Prevention.
Correspondence to: Zardasht Oqab
GAC 82-3280 Hospital Drive NW
Calgary, AB, Canada T2N 4Z6
Atrial fibrillation (AF) is the most common arrhythmia in the elderly and its prevalence increases with age[1]. AF substantially increases the risk of ischemic stroke[2] and is associated with increased mortality[3]. Stroke prevention using oral anticoagulants (OAC) effectively reduces this risk by 64%[4]. Paradoxically, though the prevalence of AF is the highest in the very elderly, the rate of appropriate anticoagulation decreases with age[5-7]. One potential reason for this could frailty.
Frailty is a biologic syndrome of decreased reserve to stressors, resulting from cumulative declines across multiple physiologic systems leading to a decline in homeostatic reserve and resiliency[8]. Frailty is associated with adverse outcomes such as increased falls, hospitalizations, worsening disability, nursing home admissions and mortality[9]. Frailty in community-dwelling adults increases with age, affecting 11% of elderly over the age of 65 years and 25% over the age of 85 years[10]. Although it is also not well known whether frailty affects long term outcomes in elderly patients with AF, it may influence management decisions.
We conducted a systematic review to determine the prevalence of frailty in patients with AF and whether measured frailty is associated with reduced rates of oral anticoagulation in these patients.
Details of the protocol for this systematic review were registered on PROSPERO CRD42017056795.
We systematically searched Cochrane, MEDLINE, EMBASE, and PubMed databases. Our search strategy was designed to provide high sensitivity for finding all relevant studies and was not restricted by language. This was accomplished by using both Medical Subject Headings (MeSH) terminology and key words related to: 1) atrial fibrillation, 2) frail elderly, and 3) geriatric assessments. A search of references and free text search of world wide web was also conducted. Appendix A shows a sample search strategy.
We included randomized control trials, cohort studies, case control studies and other nonrandomized comparative studies if they compared rates of oral anticoagulation (using warfarin or direct-acting oral anticoagulants) in frail versus non-frail elderly and used any validated frailty instrument to measure frailty. We included studies with either accumulation of deficits (frailty index) model[11]or the phenotype model[12]. Studies without a comparison group of non-frail elderly were excluded. We also excluded articles that were not full length.
The titles and abstracts of potential papers were independently reviewed by two authors. Full text articles were obtained when there was uncertainty in the studies. Data extraction and assessment of validity were also performed by both reviewers and confirmed by a third reviewer.
The quality of studies was evaluated independently by two reviewers using the Newcastle-Ottawa Scale (NOS)[13]. Disagreements between reviewers were resolved by discussion. A score above 6 is considered as high quality.
Data was analyzed using Comprehensive Meta-Analysis software version 3 (Biostat Inc. Englewood, NJ). Prescription of anticoagulation for each study were expressed as odds ratios and 95% confidence intervals. Weighted mean differences and 95% confidence intervals were calculated for each variable. Pooled odds ratios were calculated using random-effects model. Heterogeneity was estimated using I2 statistic in a fixed effect analysis; a value <25% (low), 25-50% (moderate) and >75% (high)[14].
Search strategy and characteristics of studies
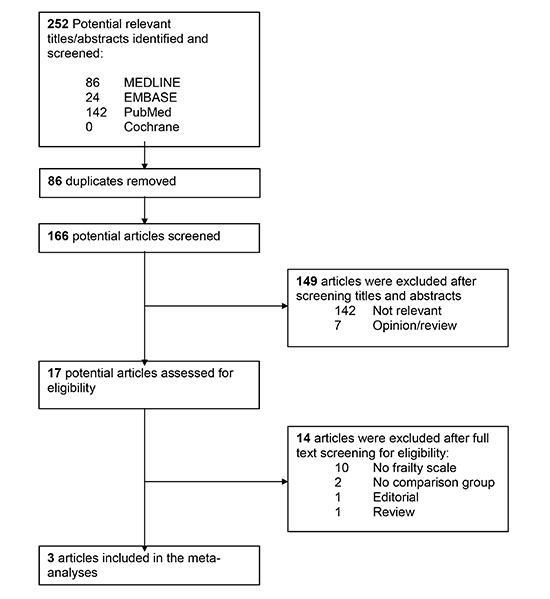
[Figure 1] shows the details of the systematic literature search. We screened 166 relevant titles and abstracts, of which 17 full text articles were assessed for eligibility. Three studies met inclusion criteria and included a total of 1204 patients. The characteristics of each study including co-morbidities and risk factors for stroke and bleeding are described in [Table 1].
Table 1. Characteristics of studies included in the meta-analysis
| First author, Year |
Perera, 2009 |
Nguyen, 2015 |
Lefebvre, 2015 |
| Study design |
Prospective observational |
Prospective observational |
Cross-sectional |
| Frailty instrument |
Edmonton Frail Scale |
Edmonton Frail Scale |
Clinical Frailty Scale |
| Sample size |
207 |
302 |
682 |
| Age in Years, Mean ± SD |
82.7 ± 6.3 |
84.7±7.1 |
85.0 ±4.4 |
| Male % |
46 |
50 |
40 |
| Frail n (%) |
64 |
53 |
25* |
| % anticoagulated |
50 |
55.7 |
70 |
| # of medications ± SD |
8.0 ± 3.4 |
11.3 ± 4.0 |
13.5 ± 4.5 |
| Stroke Risks |
|
|
|
| CHF |
35 |
43 |
32 |
| Hypertension |
71 |
69 |
88 |
| Age≥75 |
88 |
90 |
NR |
| Diabetes |
25 |
21 |
31 |
| Previous stroke/TIA |
20 |
25 |
33 |
| Vascular disease |
NA |
37 |
16 |
| Bleeding Risks % |
Applied to all 220 patients |
Applied to 161/302 receiving anticoagulation at discharge |
Applied to all 682 patients |
| Hypertension |
71 |
69 |
88 |
| Hepatic or Chronic Kidney Disease |
22 |
14 |
16 |
| Bleeding history |
NA |
48 |
20 |
| Anemia |
17 |
NR |
73 |
| Alcohol use |
3 |
3 |
4 |
| Malignancy |
25 |
25 |
NR |
| Falls |
69 |
NR |
59 |
| Other % |
|
|
|
| Dementia |
NA |
9 |
26 |
| Findings |
Frailty was associated with underprescription of OAC |
Frailty was not associated with anticoagulation rates |
Frailty was associated with underprescription of OAC |
*Lefebvre et al dichotomized frailty into non-frail/mildly to moderately frail (<7) and severely frail (>=7). Frailty prevalence reported is based on their cut offs.
Perera et al.[15] conducted a single center prospective study of 220 hospitalized adults in Australia with a mean age of 83 ± 6. Frailty was evaluated using Reported Edmonton Frail Scale (REFS)[16] and anticoagulant use was confirmed by medications in the discharge summary. They found that 64% of subjects were frail and 39% received anticoagulation at discharge. Frail patients were less likely to receive warfarin than non-frail on hospital admission (P = 0.002) and discharge (P < 0.001). Nguyen et al.[17] conducted a prospective observational study of 302 hospitalized patients in Australia with a mean age of 85 ± 7. Frailty was assessed using REFS and prescription of anticoagulation was confirmed from medications in the discharge summary. They found that 52% of subjects were frail and 56% received anticoagulation at discharge. Frailty decreased the likelihood of anticoagulant prescription (odds ratio (OR) 0.58, 95%CI 0.36–0.93) on univariate analysis but not on multivariable analysis (OR 0.66, 95%CI 0.40–1.11). Lefebvre et al.[18] conducted a cross-sectional study of 682 hospitalized patients in Canada with a mean age of 85 ± 4. Frailty was determined using the Canadian Study of Health and Aging Clinical Frailty Scale (CFS)[11] through chart review and the presence of anticoagulation was confirmed from documentation in medical chart. They found that 25% of subjects were frail and 70% received anticoagulation. The absence of severe frailty (CFS < 7; OR, 3.41; 95% CI, 1.84-6.33) was independently associated with anticoagulant use in multivariable analyses.
Figure 1. Flow diagram for the systematic literature review
The cohort studies included in the final analysis were prone to bias. There is potential selection bias amongst all three studies based on differences in study participant’s age of eligibility[15,17,18] and higher bleeding risks.[17] Lefebvre et al also included more females (60%) who are more prone to being frail.[10] These studies also had information bias based on methods of confirmation of anticoagulation. Nevertheless, the quality of the three studies assessed was high based on average NOS score of 6 out of possible maximum of 9.
Table 2. Quality assessment of studies using Newcastle Ottawa Scale. A cohort study can be awarded maximum of 4 stars for Selection, 2 stars for Comparability and 3 stars for Outcome.
| Study |
Selection |
Comparability |
Outcome |
| Perera (2009) |
*** |
* |
** |
| Nguyen (2015) |
*** |
** |
* |
| Lefebvre (2015) |
*** |
** |
* |
The weighted mean prevalence of frailty in patients with atrial fibrillation was 39% (95%CI 36-42). Perera et al reported the highest prevalence of frailty at 64%. The authors used a REFS cut off score of 8 as frail and ≤7 as non-frail. Nguyen et al also used REFS cut of 8 as frail and reported a prevalence of frailty of 53%. Lefebvre et al used the CFS score and a cut of ≥7 as frail and <7 as non-frail by combining non-frail/mildly and moderately frail. Using their cut off, the prevalence of frailty was 25%.
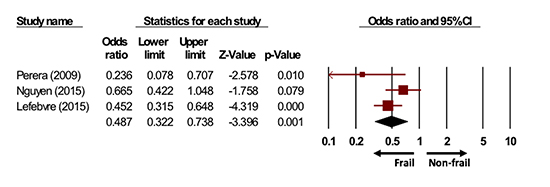
Anticoagulant use and frailty [Figure 2]
The weighted mean prevalence of anticoagulation was 63%. Elderly patients who were classified as frail were significantly less likely to receive oral anticoagulation compared to non-frail elderly (pooled OR 0.49, 95% CI 0.32-0.74). There was a moderate degree of heterogeneity amongst the studies (I2=45%).
Figure 2. Random effects model meta-analysis of prescription of anticoagulation in frail versus non-frail elderly. Frail elderly subjects were less likely to receive anticoagulation compared to non-frail elderly subjects.
We performed a systematic review to assess the prevalence of frailty and whether measured frailty affected rates of anticoagulation in hospitalized elderly with atrial fibrillation. Only three qualified reports could be identified and the overall quality of evidence was low.
We found that approximately 40% of adults with AF over the age of 80 who are admitted to an acute care hospital are diagnosed as frail. This is higher than a previous large study of community dwelling adults that found the prevalence of frailty to be 15.7% (aged 80–84) and 26.1% (≥85)[10]. It is also higher than a recent study involving patients admitted to an inpatient ward that found the overall prevalence of frailty to be 13.9%[19]. These studies however did not report on participants’ co-morbidities or presence of cardiovascular disease. Therefore, one possible explanation could be that patients with AF are more prone to frailty compared to patients with no AF, a finding supported by a prior study[20].
The differences might also be due to the type frailty instrument used. It has been shown that the prevalence of frailty can range from 3.6-34% in the same patient cohort depending on the frailty instrument that is used[21]. Similar findings were reported in another study involving acute care admissions which found the prevalence of frailty varying between 17.9-66.4% according to frailty instrument used[22]. These variabilities highlight the dynamic and complex nature of the frailty syndrome. It also highlights a potential area of opportunity to identify a “gold standard” which is yet to be defined.
Reporting anticoagulant use in frail patients
This analysis showed that the rate of OAC prescription is lower in frail elderly as compared to non-frail. Geriatric characteristics such as cognitive impairment, malnutrition risk, depression and falls are frequently cited reasons for underprescription of oral anticoagulants[23]. However, evidence supporting these reasons are lacking. Falls are not a strong contraindication to receiving OAC and patients who are prone to falls still receive the benefits of OAC for stroke prevention[24]. Age alone should not be a contraindication to anticoagulation as the absolute risk of intracranial hemorrhage among elderly patients on an anticoagulant is relatively low at 0.2% per year[25]. Furthermore, the use of NOACs in patients aged 75 and older was shown to be safe and effective for stroke reduction[26].
In all three studies the measurement of frailty was not performed by the prescribing physician. Therefore, it remains unclear if the physicians’ behavior towards anticoagulation would change if the most responsible physician were to measure frailty. Furthermore, the observed heterogeneity of the studies could be due to different populations of elderly in Canada and Australia, differences in clinical practice in hospitalized patients and stroke prevention management in patients with AF. Accordingly, we can only tentatively conclude that apprehension of frailty was associated with under-prescription of anticoagulants.
Our study has several limitations. We eliminated studies in which the methods of measuring frailty were not clearly defined. We also limited studies that did not have a comparison group of non-frail reported. This may have decreased our overall sample size but we think a comparison group of non-frail subjects is essential to ascertain the effect of frailty on anticoagulation prescription. The methods of confirming anticoagulation prescription were done by chart review, a method prone to error. Discharge summaries can contain errors in 12-13% of handwritten and electronic summaries, with errors of omission being particularly common[27]. Medication error rates in hospital and at time of discharge can be as high 50-65%[28]. Therefore, prescription of anticoagulation in elderly patients have inherent limitations, but overall do show an inverse relationship with presence of frailty.
Our results are subject to the limitation of meta-analyses which includes the aggregation of data from different studies with variable methods, definitions of frailty, baseline characteristics and from countries where frailty prevalence maybe different. There is inherent heterogeneity between the frailty instruments used in our studies as such pooling the studies might affect conclusions. However, regardless of the instrument used, all three studies used a cut of severely frail and those who were pre-frail to moderately frail were classified in the non-frail group. Therefore, the conclusions would be more applicable to elderly diagnosed as severely frail. The current studies involved only hospitalized patients and whether the results apply to community dwelling healthy elderly is unknown.
None of the authors have any conflict, financial or otherwise.
These studies were conducted in acute care settings and corresponding community data are unknown. As well whether frailty should be measured in all patients > 65 years or limited to those over the age 80 is unknown. It is also unknown what to do with the severely frail patients in terms of anticoagulation as the majority have a poor prognosis[29]. The current Canadian Cardiovascular Society and international guidelines do not provide advice in this patient population[4,30]. Future studies are needed to determine to what extent are frailty instruments are used in the community by physicians and how do they impact anticoagulation decisions. It would also be important to determine whether measurement of frailty in community dwelling adults prospectively using a validated instrument would increase prescription rates of anticoagulation and study outcomes of stroke prevention and adverse bleeding events.






