Atrial Fibrillation as a Cause of Incident Heart Failure: A Discrete Clinical Phenotype
George Louridas1, Katerina Lourida2
1Department of Cardiology, Aristotle University, Thessaloniki,Greece.2MSc in Information Security.
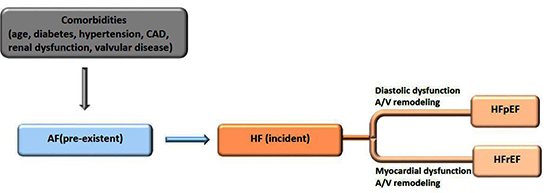
In a recently published research paper by Dhawan and Gopinathannair [1] it was presented the clinically important relationship between arrhythmia and induced cardiomyopathy. It was stated correctly that this association is under-recognized and potentially reversible. In the present letter, it is underlined the clinical conundrum of the atrial fibrillation (AF) and heart failure (HF) coexistence with the appearance of multiple clinical phenotypes. Both AF and HF are common cardiac disorders with significant cardiovascular morbidity and mortality. The generation of multiple heterogeneous syndromes that follows the AF-HF coexistence is not always clearly defined and often each clinical entity begets the other one. But, among the clinical phenotypes produced it is possible to identify an under-recognized and concealed subgroup of patients with pre-existent AF followed by incident HF that represents a distinct clinical phenotype. This subgroup represents a sizeable cohort of patients with a variety of important contributing clinical comorbidities or predictors or risk factors and ill defined pathophysiological mechanisms. In such complex clinical phenotypes the clinical problem is multifaceted with potential interconnections and interactions with comorbidities and other risk factors. Most probably this cohort of patients with AF is predisposed to incident HF because of myocardial or volume-related structural changes like ventricular hypertrophy, left atrial or ventricular dilatation and diastolic dysfunction. Recognition of this vulnerable subgroup of patients with AF will permit specific therapeutic interventions aiming to change the unfavorable electrical and mechanical remodeling of left atrium or left ventricle. While the intimate relationship between AF and HF has been recognized, the frequency and clinical significance of the proposed phenotype has not been adequately evaluated and remains a clinical and therapeutic conundrum [Figure 1]. In the 2013 report of the American College of Cardiology Foundation/American Heart Association Task Force (ACCF/AHA) on Practice Guidelines for the “management of heart failure”, the AF section is included under the chapter of “Important Comorbidities in HF” [2]. Also, in the AF section, it is recorded that “for patients who develop HF as a result of AF, a rhythm control strategy should be pursued” and “it is important to recognize that AF with a rapid ventricular response is one of the few potentially reversible causes of HF” [2]. Despite this recognition, in both sections was underrated the existence of a separate clinical phenotype characterized by pre-existent AF followed by incident HF. Singh et al [3] state that “there is a subset of patients with AF who are predisposed to HF” and “identifying the exact phenotype is challenging due to the complexity of many contributing parameters”. Acknowledgement of the clinical importance of AF-HF association and recognition of the primary role of AF as a cause of HF should change the general notion that AF is only a comorbidity of HF. This clinically concealed subgroup should be given the status of a discrete clinical phenotype and recognized as such in medical disease taxonomy. It must be recognized that the proposed clinical syndrome is a separate phenotype of high epidemiological and clinical importance. Moreover, this recognition underlines the therapeutic strategy involved with prompt rhythm or rate control in order to avoid further HF progression and clinical deterioration. Two pertinent questions are raised related to the nature of AF-HF coexistence of the proposed clinical phenotype: what exactly causes the emergence of incident HF only in some of the patients with pre-existent AF and if the clinical subtype of HF with preserved ejection fraction (HFpEF) is more common than HF with reduced ejection fraction (HFrEF) [Figure 2]. For this purpose, large number of patients with AF should be followed-up both in observational and prospective randomized future clinical trials. Network data mining in patients with HF and AF is an important tool together with information and communication technologies to collect biological and clinical material related to pre-existent AF / incident HF phenotype. Technologies like network data mining may tract down from medical and other scientific literature relevant biological and clinical networks of importance for HF and AF patients. Network data mining from a variety of published or future clinical trials could detect relevant networks from genetics to clinical phenotypes and unveil specific robust networks related to comorbidities and genomic or nongenomic risk factors involved in the genesis of pre-existent AF / incident HF phenotype [4]. This approach may facilitate to understand and interpret the hidden pathophysiology and pathoetiology of the pre-existent AF and its progression to clinically significant HF. Future extensive clinical research in this field will facilitate the establishment of new diagnostic and therapeutic approaches.
Figure 1. Comorbidities and pathophysiological changes are driving the clinical coexistence between AF and HF.
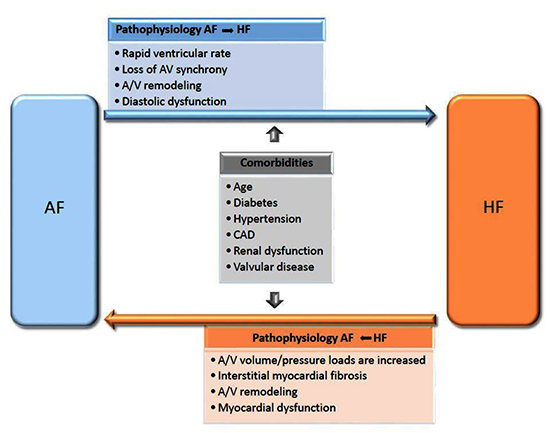
Figure 2. A distinct phenotype of pre-existent AF progressing to incident HF, either as HFpEF or HFrEF subtype.