California study of Ablation (CAABL):early utilization after index hospitalization for non-valvular atrial fibrillation
Uma Srivatsa1, Beate Danielsenb2, Ezra Amsterdama1, Yingbo Yanga1, Dali Fan1, Nayereh Pezeshkiana1, Richard H Whiteb2
1Division of Cardiovascular Medicine, UC Davis.2Department of Internal Medicine, UC Davis.
Catheter ablation (ABL) for non-valvular AF (NVAF) is recommended for symptomatic patients refractory to medical therapy and its success is related to the duration of the arrhythmia prior to intervention.Our aim was to assess the early utilization and the factors that prompted ABL in patients hospitalized for new onset NVAF.
Using de-identified administrative discharge records for hospitalizations and emergency department (ED) visits, we determined the patients who had a first-time (since 1991) health record diagnosis of AF between2005 - 2011. We linked ambulatory surgery encounters for ABL based on ICD 9 code occurring within two years of initial hospitalization. After excluding other cardiac arrhythmias, atrio-ventricular nodal ablation or pacemaker/defibrillator placement and cardiac valve disease, bivariate comparisons were made with those who did not undergo ABL.
During the study period,3,440 of 424,592 patients (0.81%) hospitalized for new onset NVAF underwent ABL. Parameters significantly (p<0.001) associated with ABL compared tonon-ABL patientsincluded: principal diagnosis of AF (55% vs 25%), age 35-64 yrs (46.1% vs. 22.4%), male (58.9% vs. 48.2%), private insurance (46.6% vs. 21.1%), Caucasian (81.0% vs.71.6%), lower frequency of ED visit < 6 months before index AF hospitalization (10.7% vs. 15.9%), lower severityofillness at time of AF diagnosis (16.5% vs. 35.6%) anda lower prevalence ofmajor comorbidities (p< 0.001).
Ablation has low utilization for treatment of new onset NVAF within two years of diagnosis. Earlier utilization of ABL may reduce health care burden related to NVAF and requires further evaluation.
Key Words : Ablation, Atrial fibrillation, Frequency, Epidemiology.
Correspondence to: Uma Srivatsa, MBBS, MAS, FACC, FHRS 4860 Y street, ste 2820 Sacramento, CA, 95817 Phone: 916-734-3764 Fax: Fax: 916 7348394 Email: unsrivatsa@ucdavis.edu
The current age-adjusted incidence of atrial fibrillation (AF) is13.4 per 1000 person-years[1]and the prevalence ofAF is projected to be over 10 million in the United States by 2050.[2]These patients are at risk for several morbidities requiring recurrent hospitalization, thus contributing to a huge economic burden from direct and indirect costs. [3]-[5]Medical management of non-valvular (NV)AF for rhythm control has moderate success,with median time to recurrence ranging from 74 - 487 days, reflecting frequentrelapses within first two years. [6], [7]The natural history of AF typically progresses fromparoxysmal episodes (PAF) triggered by premature atrial complexes from pulmonary veins or non pulmonary vein locations such as superior vena cava and posterior wall of left atrium, to persistent AF (PeAF) due to rotors, and substrate remodeling.[8]-[13]These patients present frequently with symptoms, however somepatients areasymptomatic with persistent AF of unknown duration. The mean duration of PAF is approximately 1.7 yrs before progressing to PeAF as noted in data from tertiary care centers.[14]
Clinical trials have shown superiority of ABL over medical therapy when used as second line intervention, and equivalent as first line treatment.[15]-[19] The reported frequency of maintaining sinus rhythm after ABL at one year varies approximately from 60-80%,[16], [17], [19], [20]with PAF requiring less extensive ablation compared to PeAF, achievinggreater success in maintaining sinus rhythm,[21][22]and resulting in fewer procedure related adverse events. [23]The defined success of ABL (non-recurrence of AF > 30 sec) isdependent on the type of AF prior to intervention[24] and theoverall duration of AF.[14] Evidence reflects superior control of AF when ABL is performed early in the course of the disease and is thereforerecommended for those who are refractory or intolerant to therapy with at least one drug.[25]-[27]
Our aim was to determine the frequency and predictors of early catheter ablation (< 2 years) in Californiaby a case control study of new onset AF. We hypothesized that hospitalization or emergency department visits represent severely symptomatic AF and may reflect a population with increased likelihood of referral for ABL.
This case control study was approved by the State of California Committee for the Protection of Human Subjects, and by the UC Davis institutional review board. The database utilized constituted patient discharge information from hospitalizations (PDD), emergency department (ED) and ambulatory surgery (AS) encounters from California non-federal hospitals.After linking the PDD, ED and AS databases, we identifiedthe patientshospitalized with a diagnosis of AF (427.31)between Jan 1, 2005 to Dec 31, 2011, and then excluded all the cases with any prior discharge diagnosis of AF, back to 1990. Among these cases that had an incident hospitalization with a diagnosis of AF after Jan 1 2005, we identified all those who underwent an endovascular ablation (ICD-9-CM = 37.34) between Jan 1, 2005- Dec 31, 2011. We excluded all patientsthat also had a diagnosis of atrial flutter (427.32), supraventricular tachycardia (427.0), ventricular tachycardia (427.1), underwent an open surgical ablation (only procedure =37.34) and all cases that had pacemaker implant (37.80-37.87) coupled with a diagnosis of sino-atrial node dysfunction (427.81) or atrio-ventricular block (426.0-426.1). Rural and urban hospitals were defined basedon recommendations by Office of Statewide Health Planning and Development (OSHPD) with areas under 250 persons/ square mile considered as rural.Comorbidities were defined using the Elixhauser comorbidity index (Healthcare Cost and Utilization Project V3.7), which identifies 29 major comorbidities based on ICD-9-CM codeslisted as being present at the time the admission of first admission with AF.[28] Patients with valve disease were excluded and the remainder were considered to have NVAF. Patients with dementia, human immunodeficiency disease, alcohol abuse, active cancer or psychosis were also excluded. We reviewed approximately 200 hospitalization records to verify the accuracy of the inclusions and exclusions.
All patient refined (APR)-DRGs are measures to assess patient characteristics for resource utilization as an all payer alternative to Medicare system (MS)-DRG and has four levels of severity.We applied this previously described measure called “the severity-of-illness (SOI)” utilizing a software (APR-DRG version 24; 3M) at the time of the hospital admission (minor, moderate, severe and extreme).[29-31]Many of the co-morbidities defined by this algorithm are known risk factors associated with AF.
We compared demographic and clinical characteristics of cases that underwent ABL within two years to controls who never underwent ablation during the study period. Predictors undergoing ABL were analyzed using a proportional hazard model that included demographic variables, clinical variables, SOI, insurance status, and intercurrent hospitalization with a principal diagnosis of AF as a time dependent covariate. SAS version 9.3 was used for all statistical analyses. Continuous variables were expressed as mean + SD. Categorical variables were presented as percentages. Uni-variate analysis was performed with a χ2 test for nominal variables and Fisher’s exact test was applied for outcomes fewer than 5 events per cell. Analysis was performed using multivariable proportional hazard modeling to predict outcomes. A p-value < 0.05 was considered significant.
Among the total adult population in California (28,068,224), 424,492cases had a first-time hospitalization with a diagnosis of NVAF between 2005-2011, averaging 60,000 admissions per year. [Figure 1]Of these cases, 106,942 patients (25.2%) were admitted for a principal diagnosis of NVAF and 317,650patients (74.8%) had a secondary diagnosis of NVAF. The majority of these patients (75.9%) were >65 yrs old; the number of males (2.39/1000) and females (2.38/ 1000) were comparable.The payer source for the majority of the cases, was medicare (69%)and approximately one fifth had private insurance. [Table 1] There was a slight decrease in the number of cases with a first time admission for NVAF from 60,484 in 2005 to 56,829 in 2009; in 2011, there was an increase to 62,439.[Figure 1A] Most patients were hospitalized in an urban facility (94.3%). Two- thirds of the patients were admitted with moderate or major severity of illness, while a third were either EDadmissions or mild severity of illness.Approximately 60% the patients had hypertension (HTN); diabetes mellitus (DM), heart failure (HF),chronic obstructive pulmonary disease (COPD), obesity were relatively frequent. [Table 2]The prevalence of AFwas higher among Caucasians compared to other races/ethnic groups.[Figure 2]
Figure 1A. Number of hospitalizations or emergency department visits for non valvular atrial fibrillation (NVAF) between 2005-2011
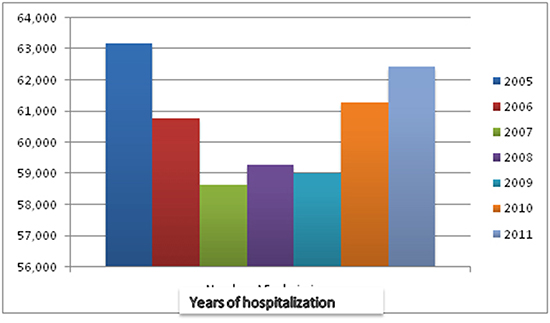
Figure 1B. Percentage of ablations for NVAF every year
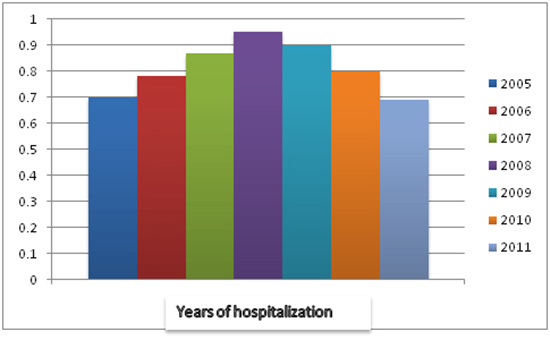
Table 1. Baseline characteristics of patients admitted for first time diagnosis of Non valvular atrial fibrillation (NVAF) 2005-2011 in non federal hospitals in California
| Characteristics |
Total population |
Percent |
| All Patients with new AF in 2005 though 2011 |
424,592 |
100.0 |
| New AF prin DX (427.31) |
|
106,942 |
25.2 |
| New AF any secondary diagnosis (427.31) |
317,650 |
74.8 |
| Patient Age |
18-34 |
6,335 |
1.5 |
|
35-49 |
21,640 |
5.1 |
|
50-64 |
74,212 |
17.5 |
|
65-79 |
155,568 |
36.6 |
|
80 or older |
166,837 |
39.3 |
| Patient sex |
Male |
209,371 |
49.3 |
|
Female |
215,221 |
50.7 |
| Payer source (index admission) |
Medicare |
293,791 |
69.2 |
|
Medicaid |
20,782 |
4.9 |
|
Private, incl. HMO |
90,337 |
21.3 |
|
Self-pay |
10,561 |
2.5 |
|
No charge |
8,463 |
2.0 |
|
Other |
658 |
0.2 |
| Race/ethnicity (index admission) |
White |
304,451 |
71.7 |
|
Hispanic |
51,114 |
12.0 |
|
Black |
21,000 |
4.9 |
|
Asian/Pacific Islander |
31,500 |
7.4 |
|
Other |
16,527 |
3.9 |
| Inpatient admission within 6 months preceding new AF admission |
56,017 |
13.2 |
| ED visit within 6 month of new AF admission |
67,502 |
15.9 |
| Outpatient admission within 6 months preceding new AF admission |
32,834 |
7.7 |
| Rural location (index admission hospital) |
Urban |
400,317 |
94.3 |
|
Rural
|
24,275 |
5.7 |
| Admission year |
2005 |
63,164 |
14.9 |
|
2006 |
60,787 |
14.3 |
| Admission year |
2007 |
58,625 |
13.8 |
|
2008 |
59,275 |
14.0 |
|
2009 |
59,010 |
13.9 |
|
2010 |
61,292 |
14.4 |
|
2011 |
62,439 |
14.7 |
AF- Atrial fibrillation
Table 2. Comorbidities associated with new diagnosis of Non valvular Atrial Fibrillation
| Co morbidities |
|
n |
% |
| Discharge severity |
ED Case |
98,478 |
23.2 |
|
Minor |
43,355 |
10.2 |
|
Moderate |
132,453 |
31.2 |
|
Major |
115,209 |
27.1 |
|
Extreme |
35,097 |
8.3 |
| Congestive heart failure |
|
105,645 |
24.9 |
| Valvular disease |
|
40,071 |
9.4 |
| Pulmonary circulation disease |
|
20,283 |
4.8 |
| Peripheral vascular disease |
|
38,312 |
9.0 |
| Paralysis/Other neurological disorders |
45,540 |
10.7 |
| Chronic pulmonary disease |
|
92,533 |
21.8 |
| Diabetes |
|
109,886 |
25.9 |
| Hypertension |
|
254,573 |
60.0 |
| Renal failure |
|
56,342 |
13.3 |
| Liver disease |
|
8,629 |
2.0 |
| Rheumatoid arthritis/collagen vas |
11,981 |
2.8 |
| Coagulopthy |
|
17,387 |
4.1 |
| Obesity |
|
50,225 |
11.8 |
| Deficiency Anemias |
|
88,903 |
20.9 |
| Depression |
|
33,786 |
8.0 |
| Coronary artery disease |
|
54,968 |
12.9 |
ED- Emergency department
ABL was performed < 2 years from the first hospitalization/ ED visit in 3440 (0.81%) of the total number of cases admitted during the study period.[Table 3] The number of ablations peaked at 564 (0.95%) in this population in 2008, followed by a decline [Figure 1B] (p<0.0001). ABL wasmorelikely to be performed in cases admitted specifically for NVAF (1.8%) as opposed those that had to a secondary diagnosis of NVAF(0.49%) (p<0001). Males were more likely to undergo ABL (1%) compared to females (0.7%, p<0.001) and Caucasians (0.92%) morethan other ethnicities (p<0.001).There were no differences in rural vs urban ABL.Patients with private insurance (1.8%) were more likely to have ABL than those with Medicare (0.5%, p<0.001) or other insurance, although a majority of the patients were > 65 yrs and had Medicare coverage.[Table 3]
Figure 2A. Gender variation is ablation for non valvular atrial fibrillation (NVAF) among all patients admitted with new onset NVAF
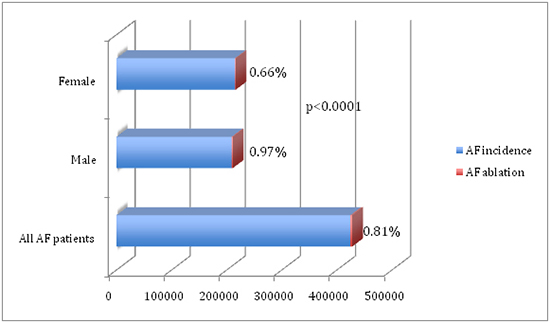
Figure 2B. Racial distribution of hospitalization or emergency department visits for NVAF in non federal hospitals in California (2010)
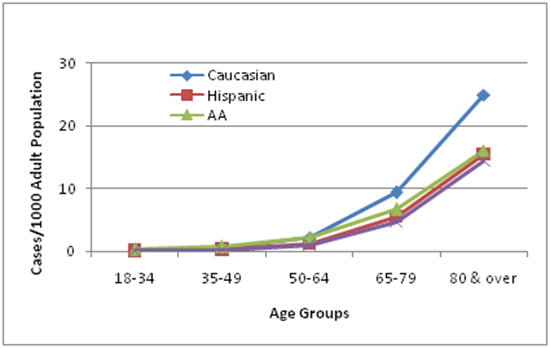
Table 3. Results: Predictors of early ablation for non –valvular atrial fibrillation (NVAF)
|
Ablation(n=3440) (%) |
No ablation(n=421152) (%) |
P value |
| Principal Diagnosis of NVAF |
|
1.8 |
<0.0001 |
| Secondary Diagnosis of NVAF |
|
0.5 |
<0.0001 |
Patient age (yrs)
| 18-34 | | 35-49 | | 50-64 | | 65-79 | | 80 or older |
|
|
|
<0.0001 |
| Male
Female |
|
0.97
0.66 |
<0.0001 |
| Payer source
Medicare
Medicaid
Private |
45.3
3.4
46.6 |
69.4
4.9
21.1 |
<0.0001 |
| Race
White
Hispanic
Black
Asian/Pacific Islander
Other
|
71.6
12.1
5.0
7.4
3.9 |
0.92
0.54
0.38
0.51
0.83 |
<0.0001 |
| Discharge Severity
ED case
Minor
Moderate
Major
Extreme |
23.1
10.1
31.2
27.2
8.3 |
1.1
1.76
0.77
0.42
0.25 |
<0.0001 |
| Co Morbidities:
Heart failure
Coronary artery disease
Peripheral vascular disease
Prior stroke/neuro disorders
Pulmonary disease
Obesity
Diabetes
Hypertension
Renal Failure |
15.4
8.8
3.4
3.7
14.8
11.3
15.8
49.6
4.8 |
25.0
13.0
9.1
10.8
21.9
11.8
26.0
60.0
13.3 |
<0.001
<0.001
<0.001
<0.001
<0.001
ns
<0.001
<0.001
<0.001 |
Risk-adjusted predictors included: admission for principal diagnosis of NVAF (HR=2.1), younger age (HR= 3.9); age (50-64 vs >80); male (HR=1.2), private insurance (HR=1.8vs. Medicaid); Caucasian (HR= 2.1 vs. Hispanic), mild severity of illness (HR=1.4). There was less coronary artery disease, peripheral vascular disease, stroke/ neurological disorders, DM, HTN, HF, renal failure, and COPD, but no difference in obesity between ABL and non ABL groups. [Table 4]
Table 4. Predictors of ablation of patients hospitalized for atrial fibrillation
|
Ablation (n=3440) |
No ablation (n=421152) |
P value |
| Heart failure (%) |
15.4 |
25 |
<0.001 |
| Coronary artery disease |
8.8 |
13 |
<0.001 |
| Peripheral vascular disease |
3.4 |
9.1 |
<0.001 |
| Prior stroke/neuro disorders |
3.7 |
10.8 |
<0.001 |
| Pulmonary disease |
14.8 |
21.9 |
<0.001 |
| Obesity |
11.3 |
11.8 |
Ns |
| Diabetes |
15.8 |
26 |
<0.001 |
| Hypertension |
49.6 |
60 |
<0.001 |
| Renal failure |
4.8 |
13.3 |
<0.001 |
The prevalence of AF is high,[2], [32]primarily attributable to its association with aging, HTN, DM,HF, sleep apnea, pulmonary diseases and obesity.[33]-[37]Worldwideadmissions for AF have increased from 35 to 110/10,000 population between 1996-2006, likely due to the augmented prevalence of these risk factors.[2]However, because of the presence of asymptomatic episodes of AF, the exact prevalence is unknown.[38]-[40]In this study, we attempted to determine if these epidemiologic data correlate with an increase in hospitalizations/ ED visitsfor AF in California. We found that the average admissions for AF have been ~ 60,000/ year without a significant change between 2005-2011,[Figure 1A], although this could reflect improved ambulatory care of AF patients.
Similar to previously described associations,in our large study from a California multiethnic population, two-thirds of the patients were over 65 yrs of age, with a third each in the age groups 65-79 yrs and > 80 yrs. AF has been reported to have an increased frequency in males although there are more women with this arrhythmia due to their longer life expectancy.[33], [41] By contrast,in our NVAF population, we found equal prevalence of women and men among those hospitalized for NVAF, which is likely due to a higher association of valvular heart disease among women in the afore mentioned study.[33]As has been previously described, there was also a Caucasian preponderance of NVAF in our cohort.[42]Two- thirds of our patients were admitted with moderate or major illnesses, while a third were either ED admissions or had mild severity of illness, confirming the widely known association of AF to acute ailments.
Due to lack of a specific ICD-9 code, we excluded other arrhythmias and considered ABL as specific for AF when associated in the principal position at the time of hospitalization. We also excluded patients with implantable cardiac devices to avoid those who could have AV node ablation. We decided on an approximate interval of two years as “ early” for these patients to have received follow-up care and to have declared themselves in need of invasive management based on natural progression of NVAF and clinical trials of medical management previously described.[7], [14], [43]
Several studies have shown that the outcomes of ABL are superior with shorter duration of AF. [44]-[48]However, despite these salutary results and advances in ABL technology, this procedure is performed in < 1% of patients within two years after the initial hospitalization in our population and includes racial and gender disparities. The Caucasian preponderance could at least partially reflect income and insurance status, however, these variables were adjusted for in the statistical analysis. The majority of California’s population resides in urban areas with medical centers in all major cities providing ABL for NVAF, which is reflected by most of our population. In a study from a national inpatient sample of patients with AF, (NIS) by Patel et al, about 2.9% of patients with underwent ABL, with a significant increase in ABL through a twelve year study period.[49] However this study sample does not represent new onset AF. The results are also weighted, as NIS represents a stratified random sample and does not include all patients, in contrast to our study in which we were able to account for all first time diagnosis of NVAF admissions. Our finding of a low ABL rate is concordant with regional variations in ABL that were noted among the US hospitals by Patel et al. In contrast to their investigation, we found that ABL was more frequent in patients with private insurance than Medicare. Consistent with the study by Bhave et al [43]of Medicare population, male Caucasians were more likely to undergo ABL in our group, even though one third of our patients were <65 yrs. In theirstudy,althoughthe majority wastreated bycardiologists, only about 15% consulted an electrophysiologist and about 1% underwent ABL, which is similar to that of our cohort. Most patients were managed by rate control with about a third also receiving anticoagulation in their study.[43]This finding supported by low ABL rates in our study suggests that rhythm control of AF by intervention is not widely recognized as a potential treatment.
At the present time, failure of AF ABL isdefined as recurrence of >30 sec of monitored AF., which is challenging to identify.[27], [50]Outcomes of clinical significance such as mortality, stroke or hospitalization for AF, have not been clearly documented.The Heart Rhythm Society recommends against ABL as an indication to prevent stroke; it favors using the CHADS2VASC risk scorefor prophylactic anticoagulation. [51]These factors may contribute to underutilization of ABL in the relatively early phase of the natural history of AF, when ABL is most effective. AF burden demonstrated in our study from California is disproportionately high compared to the number of trained electrophysiologists nationwide during the same period[52] and may indicate lack of access to care. The physician reimbursement for AF ABL is also poor for the complexity and duration of the procedure, compared to simple ablations, which could contribute to diminished interest in this beneficial procedure.
This study is a retrospective investigation with the inherent limitations of that method. We did not capture outpatient visits that could have led to ABL, and therefore our results reflect only the data pertaining to patients hospitalized with a first time diagnosis of NVAF. Any prior ablation outside California, if not coded at index hospitalization would not be identified from this method. There is also noICD 9 code specific for AF ABL; therefore our method of analysis may have missed capturing this procedure. There also may have been missed diagnoses by the coders, but the validity of the data is supported by periodic audits performed for billing purposes in most of hospitals in this study.We have also reviewed sample charts to ensure accuracy of exclusion and inclusion criteria. Although the purpose of our study was to determine early ablation (within two years of first hospitalization/ ED visit), patients may have undergone ABL later than that interval.
Our investigation suggests limited acceptance of ABL within two years of first hospitalization for NVAF in a multi-ethnic population and may reflect the need for greater awareness, improved education and access to care including ABL, as well as enhanced definition of clinical outcomes of this intervention.






