It is well known, that rhythm disorders play a pivotal role in patients with hypertrophic cardiomyopathy (HCM) and that ventricular arrhythmias are the major course of sudden cardiac death especially in young HCM patients[1]–[5]. Nevertheless, up to date the impact of atrial fibrillation (AF) in these patients is not well understood and in most cases detected by chance as a cause of heart failure or stroke[6]–[7]. Early recognition and treatment of AF is essential to improve both, quality of life and clinical outcome. This review article gives an update about incidence, implication, diagnosis and therapy of atrial fibrillation in HCM.
HCM is the most frequent monogenetic cardiomyopathy with a prevalence of 1:500[8] Depending on the localization and degree of hypertrophy, HCM patients may present with various pathoanatomic and pathophysiologic anomalies, such as left ventricular outflow tract obstruction, mitral regurgitation, diastolic dysfunction and/or myocardial ischemia and fibrosis [Figure 1]and[Figure 2]. AF is the most frequent arrhythmia in HCM. Its prevalence depends on the severity of the disease with 22 % in a general cohort [7]and up to 32% in a cohort prior to ICD and pacemaker implantation [9][Table 1]. The incidence for de-novo AF in a general HCM cohort is about 2% per year[7]–[10].
Table 1. Prevalence of Atrial fibrillation and stroke in non-referral bias HCM cohorts
| Author |
Year |
Number |
Prevalence |
Prevalence of |
|
|
of patients |
of AF |
Stroke or TIA |
| Masri et al[18] |
2015 |
1005 |
19% |
3% |
| Guttmann[58] |
2015 |
4815 |
12.5% |
3.6% |
| Siontis[26] |
2014 |
3673 |
18% |
n.a. |
| Tian[6] |
2013 |
654 |
24% |
n.a. |
| Maron[33] |
2009 |
900 |
21% |
6% |
| Olivotto[7] |
2001 |
480 |
22% |
21% for patients with AF , |
|
|
|
|
2.6% for patients without AF |
Although the majority of HCM patients are asymptomatic, some develop heart failure, present with palpitations or suffer from stroke [10]–[13] ([Table 1]). In all these devastating conditions, AF plays a key role[6].
Figure 1. Left atrial enlargement in Hypertrophic Cardiomyopathy
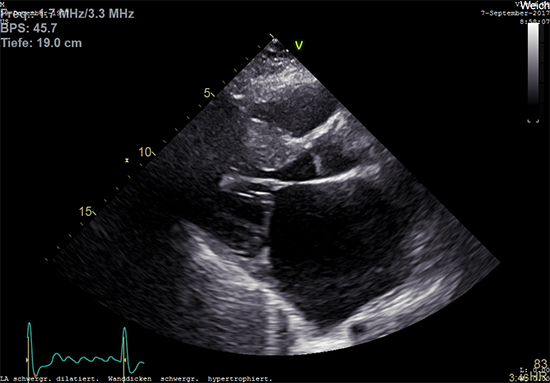
Two-dimensional transthoracic echocardiography in a 40-year-old male patient with HCM and persistent atrial fibrillation showing an enlarged left atrium with LVOT hypertrophy (IVS 20mm).
Figure 2. Mitral regurgitation in Hypertrophic cardiomyopathy
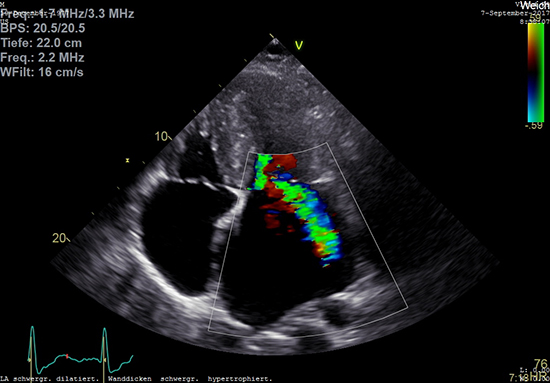
Two-dimensional transthoracic echocardiography in the same 40-year-old male patient with HCM and persistent atrial fibrillation showing an enlarged left atrium and significant eccentric mitral regurgitation.
A regular atrial contraction is necessary for left ventricular filling and function especially in HCM patients with impaired diastolic function[14]. In this context, the presence of atrial arrhythmia impairs left ventricular outflow obstruction, mitral regurgitation, diastolic dysfunction and myocardial ischemia[14].
The interaction between AF and the pathophysiological and -anatomical changes in HCM is complex. It is known that atrial fibrillation reflects both, the trigger and the result of morphological and physiological changes in cardiac anatomy[5]. In HCM, multiple changes may trigger atrial fibrillation [Figure 3]. As demonstrated in MRI scans, myocardial fibrosis disturbs a regular electrical activity leading to enhanced ectopy in atrial and ventricular myocardium[15]. Thick myocardium with reduced diastolic relaxation leads to higher left ventricular pressure resulting in elevated left atrial pressure. This process may induce atrial stress ultimately leading to atrial enlargement and the development of AF. In some HCM patients with LVOT obstruction, mitral valve anatomy and function are altered leading to valve insufficiency that further enhances the left atrial volume[16]. Mitral regurgitation is present in up to 30% in HCM patients[16].
For many years, a high LVOT gradient was the key determinant in the diagnostic and therapeutic approach in HCM. However, recent studies have shown that additional parameter should be used to predict patient´s outcome: On a stepwise multivariate survival analysis, exercise capacity during stress echocardiography, abnormal heart rate recovery, and atrial fibrillation independently predicted patients´ outcome, whereas the LVOT gradient was not associated with atrial fibrillation and had no impact on the outcome[17]-[19].
Figure 3. Pathophysiology of Atrial Fibrillation in Hypertrophic Cardiomyopathy
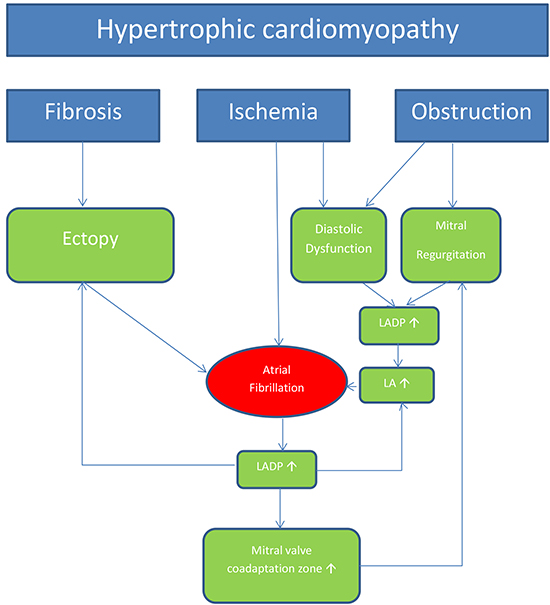
LA: left atrial diameter, LADP: left atrial diastolic pressure 10
Clinical Symptoms and Implications
Maron et al. defined three distinctive modes of death in HCM: sudden and unexpected death (51%), progressive heart failure (36%), and HCM-related stroke associated with AF (13%)[20]. Sudden cardiac death is most common in young patients, whereas heart failure and stroke-related death occur more frequently in midlife and beyond[10].
The clinical presentation of HCM patients with AF is unspecific: some patients present with signs of heart failure (dyspnoea, hypotension, pulmonary edema, chest pain), arrhythmia (palpitations, presyncope, syncope) and/or stroke. However, many patients with AF do not have any symptoms and the AF is classified as subclinical. In our own experience, the majority of HCM patients with a cardiac rhythm management device and de-novo AF were free from clinical symptoms (88%)[9]. The incidence of subclinical AF was higher in this HCM cohort compared to other patients treated with cardiac rhythm management (CRM) devices such as patients with sick sinus syndrome[21], atrioventricular block[22],[23] or stroke[23],[24]. Only patients with ischemic cardiomyopathy and an ICD had an equivalent high incidence of de-novo AF[25].
The impact of AF on survival of HCM patients is discussed controversially[6],[26]. Olivotto et al. reported a HCM-related mortality of 1.7% per year and confirmed AF as an independent risk factor for cardiovascular death, heart failure, and stroke[6],[22]. Siontis et al. demonstrated that AF is associated with a nearly 50% increased relative risk for overall mortality[26]. However, in this study AF did not affect cardiac mortality[26]. One trial identified just paroxysmal AF but not permanent AF as an independent determinant of outcome, including the risk of HCM-related death [27], which was explained by the fact that paroxysmal AF in HCM patients may be frequently subclinical and therefore untreated. Of note, HCM patients with paroxysmal AF demonstrate exercise intolerance despite being in sinus rhythm at the time of exercise testing[28].
Interestingly, in a few case reports atrial fibrillation was anticipated to trigger sustained ventricular tachycardia and sudden cardiac death in HCM patients[29],[30]. Nevertheless, as valid data are missing atrial fibrillation is not classified as a major risk factor for sudden death in the current guidelines[5].
Patients with HCM have a high risk for stroke or thromboembolic events. Stroke is an important determinant of mortality, especially in older patients. Since symptomatic and subclinical AF is the main cause of thromboembolic stroke, early detection of AF is crucial for further therapy, particularly with regard to a required oral anticoagulation. Recently published reports have suspected the left ventricular apex as an alternative source of thromboembolic complications in HCM patients[31],[32]. In unselected HCM patients, stroke and peripheral embolism occur with a prevalence rate of 6% and an incidence of 0.8% per year[7],[33] [Table 1]. However, in our own cohort of HCM patients who received a CRM device a much higher incidence of thromboembolic stroke could be detected (18%)[9]
Mandatory diagnostic interventions in patients with HCM are:
- ECG
- 48-hour ECG
- Transthoracic Echocardiography
- In case of pacemaker or ICD: ECG storage check
Additive investigations in HCM with suspected AF are:
- Magnetic resonance tomography
- external and/or implantable loop recorder
Role of ECG and 48-hour ECG
Early diagnosis and treatment of AF is crucial. However, no data exist for a standardized screening protocol to detect AF in HCM patients. In concordance with the European guidelines, we recommend an electrocardiogram and 48-hour ECG monitoring in patients with suspected AF[5]. In selected patients with left atrial dilation, we would recommend recurrent ECG and 48-hour ECG monitoring as a routine investigation in 6-month intervals to detect subclinical AF – irrespectively of clinical symptoms or echocardiographic parameters. Prolonged and recurrent ambulatory ECG monitoring increases the chance to detect subclinical AF. Remarkably, the use of ambulatory ECG monitoring reveals AF in up to 9 % of all HCM patients at the initial and annual clinical assessment[4],[5].
Furthermore, we endorse checking the ECG storage in patients with CRM devices for AF at least every 6 month. Modern ECG monitoring features of ICDs, pacemakers and implantable loop recorders are very useful to discover subclinical AF. In patients with pacemakers, subclinical atrial tachyarrhythmia without clinical symptoms was frequently detected and was associated with a significantly increased risk of thromboembolic complications[23].
Implantable loop recorder
Implantable event recorders can survey the ECG and detect atrial arrhythmia easily without intracardiac leads[24].However, no data exist regarding implantable loop recorder in HCM. As in other patients with suspected AF, implantable loop recorders are excellent tools to detect AF e.g. in patients with stroke[24],[34].
The incidence and implication of subclinical AF in patients with HCM was the subject in just a few studies. In this regard, we investigated 44 patients with HCM with a CRM device and observed a high incidence of de-novo AF after implantation in 53% of patients. The majority (88%) of these patients was asymptomatic at the time of detection[9].
Echocardiography and magnetic resonance tomography
Echocardiography is the method of choice for HCM diagnosis. However, so far, no specific echocardiographic risk factor for the development of AF has been identified in these patients. A variety of pathologic alterations associated with HCM, such as diastolic dysfunction, left atrial enlargement, myocardial fibrosis, and myocardial ischemia, may promote the development of AF[17],[35],[36] [Figure 1]and [Figure 2]. Some studies reported that left atrial dilation was related to an adverse outcome[6],[37]. Magnetic resonance tomography can add optional information, especially regarding the fibrotic burden[38]. Nevertheless, the extent of late gadolinium enhancement was inferior to the left atrial size as the strongest determinant for predicting AF prevalence, which was the strongest determinant of AF[38]. Diastolic dysfunction was also confirmed as a predictor for AF in this MR study[38]
Therapeutic options for HCM patients with AF do not differ from those without HCM. Early detection and therapy of AF is essential in the management of HCM.
Two aspects in the management of AF in HCM are important: a timely oral anticoagulation even after one single episode of AF and an appropriate rhythm or rate control using medical and interventional options[39],[40].
We strongly suggest attempting a rhythm control strategy for every symptomatic patient with newly detected AF. Even though at the moment no data are available comparing a rhythm control versus rate control strategy in HCM, maintaining sinus rhythm as long as possible and restoring sinus rhythm as soon as possible is beneficial for both: control of symptoms and improvement of hemodynamics[40].
In symptomatic patients, we prefer a rapid electrical cardioversion to restore sinus rhythm according to the 2014 AHA/ACC/HRS and the 2016 ESC guidelines[5],[41]. Although, medical
cardioversion is an alternative to electrical cardioversion, no controlled trials exist investigating different drugs in this regard. Suggested drugs to restore and maintain sinus rhythm are amiodarone, sotalol, disopyramide and dofetilide[5] .
Amiodarone is considered as the best option for rhythm control because it is safe and effective in HCM patients[40]. For other antiarrhythmic drugs, there are no valid data regarding the value. We do not recommend class I antiarrhythmic agents (flecainide, disopyramide), sotalol, or dronedarone in HCM, because of their possible side effects like ventricular arrhythmia, atrioventricular conduction delay, QTc prolongation (sotalol) or anticholinergic syndromes (disopyramide)[40]. Dofetilide as a class III antiarrhythmic agent and an alternative for amiodarone is not available in Europe and Australia.
In all cases of HCM with AF a Beta-blocker is the basis of therapy[5]. Beta-blockers modulate sympathetic activity and improve ventricular contractility, so LVOT gradient lowers, diastolic dysfunction is improved, and the incidence of supraventricular and ventricular arrhythmia is reduced[40].
Patients with recurrent AF may benefit from interventional catheter-based radiofrequency ablation, but randomized controlled trials are missing.
Many studies confirmed that catheter ablation is safe and effective for patients with HCM. However, the overall success rate is lower and usually more ablation procedures are required to achieve sinus rhythm compared with patients without HCM[42] [Table 2]. Santangeli et al. investigated the role of pulmonal vein isolation in patients with AF and HCM (28% paroxysmal AF). In this study, the success rate was low and additional procedures were needed. After a median follow-up of 42 months, only 49% of the patients remained free from AF/atrial tachycardia. All patients needed an additional procedure, in which pulmonal vein antrum and posterior wall remained isolated in 82% of the cases, but extra-PV triggers were documented in all patients[43].
Table 2. Trials investigating Catheter Ablation in HCM patients with AF
| Author |
Year |
Number |
Paroxysmal |
Follow-up |
Patients in |
|
|
of patients |
AF |
in months |
sinus rhythm |
| Santangeli[43] |
2013 |
43 |
28% |
40 |
49% |
| Dareijko[59] |
2013 |
30 |
47% |
12 |
53% |
| Di Donna[60] |
2010 |
61 |
57% |
29 |
67% |
| Bunch[61] |
2008 |
33 |
64% |
18. |
62% |
| Gaita[62] |
2007 |
26 |
50% |
19 |
64% |
| Kilicaslan[63] |
2006 |
27 |
52% |
11.5 |
70% |
In a recent metaanalysis including 15 studies, single-procedure freedom from atrial arrhythmia at the latest follow-up was 45 %[44]. With multiple procedures, the final overall success rate was calculated with 66 %[44]. The final success rate was much higher in patients with paroxysmal AF with 72 % compared with only 47 % in persistent AF[44]. In many cases, even after successful ablation, antiarrhythmic therapy is required to maintain sinus rhythm[44]. Without anti-arrhythmic drugs, the single-procedure success rate at latest follow-up was 32.9% and after multiple procedures 50.4%[44]. The risk for HCM patients to experience a relapse after a single catheter ablation therapy is about 2 times higher compared to patients without HCM[42], [45], [46]. Left atrial dilation, mitral regurgitation, atrial fibrosis, left outflow tract obstruction, and persistent AF are linked to lower success rates of catheter ablation[42],[47],[48].
The best strategy for the ablation procedure (pulmonal vein isolation vs. pulmonal vein isolation combined with atrial modification) and the optimal energy force (radiofrequency ablation vs. cryoablation) is under discussion. Adding left atrial linear ablation to pulmonal vein isolation increased the success rate in one single center study[49]. Kuck et al. demonstrated that cryoablation is as safe and as effective as radiofrequency ablation in a general AF cohort[50]. In contrast to this observation, the success rate of cryoablation in HCM was low, but this trial observed only four HCM patients with AF[51].
Considering the present data, we do not recommend surgical ablation as first line or stand-alone ablation strategy. Compared to surgical ablation strategies the observed complication rate for catheter ablation procedures in HCM was low[42] with a higher success rate[52]. However, the Maze procedure, with concomitant septal myectomy or mitral valve replacement if indicated, appears to be feasible in patients with hypertrophic cardiomyopathy and refractory atrial fibrillation[53],[54].
Until now, no data exist investigating a rate control strategy in patients with permanent AF in HCM. In line with other studies investigating a rate control strategy, we suggest beta-blockers or calcium antagonists for rate control, if a rhythm control strategy fails. Positive inotropic drugs such as digitalis are contraindicated[55]. AV-nodal ablation is a final option to avoid high heart rate in patients without sufficient rate control[56].
Maron et al. proved in a large cohort analysis of 900 HCM patients, that the cumulative incidence of stroke and peripheral embolism among patients with atrial fibrillation was significantly higher in non-anticoagulated patients compared with patients receiving warfarin[33]. New data are in line with these observations and show a 1.0% yearly risk for stroke and embolic events[12].
In contrast to patients without HCM, we do not have a validated risk score to define patients who benefit from oral anticoagulation. Even if the CHA₂DS₂-VASc Score is zero, patients with HCM are at high risk for embolic events. Parameters, such as left atrial size, mitral regurgitation, and left ventricular outflow gradient may contribute to a higher stroke risk, but do not contribute to the CHA₂DS₂-VASc Score[12].
Patients with HCM suffering from stroke need careful screening for AF because 7.4 % of these patients have newly documented AF the time of the event and 14.7 % present AF during evaluation after stroke[12]. Repetitive ECG monitoring is mandatory. However, implantable loop recorders are superior to conventional follow-up and can detect atrial fibrillation in so-called cryptogenic stroke[24].
Although long-term studies with novel oral anticoagulants are missing to date, few case reports exist showing direct oral anticoagulants to be as effective and save in HCM patients[31],[57].
In conclusion, we recommend lifelong oral anticoagulation for every HCM patient with documented atrial fibrillation independent of her or his individual CHA₂DS₂-VASc Score to reduce the risk of stroke[33].






