Routine use of intracardiac echocardiography for atrial flutter ablation is associated with reduced fluoroscopy time, but not with a reduction of radiofrequency energy delivery time
Dalibor Herman, Pavel Osmancik, Jana Zdarska, Radka Prochazkova
Cardiocenter, Department of Cardiology, 3rd Faculty of Medicine, Charles University and University Hospital KralovskeVinohrady Prague, Czech Republic..
The ablation of cavotricuspid-isthmus (CTI) atrial flutter (AFL) dependent atrial flutter could be difficult in patients with complex anatomy of the CTI.The aim of the study was to assess whether the use of intracardiac echocardiography (ICE) was associated with less fluoroscopy time and faster ablations of cavotricuspid isthmus dependent atrial flutter (CTI-AFL).
Patients with an indication for an ablation of a CTI-AFL were enrolled. Patients in which ablation of a CTI-AFLas part of an atrial fibrillation ablation were not included. Randomization was done using the envelope method. Standard techniques (i.e., coronary sinus, 20-polar halo catheter, and an ablation catheter), and criteria of success (bidirectional block through the CTI) were used. In patients randomized to the ablation with ICE, a 10F AcuNav ICE probe (Siemens, Germany)was used.
Seventy-nine patients were enrolled; 40 were randomized to ablation with ICE and 39 without ICE. The X-ray exposure was shorter (3.29±2.6 vs. 5.94±3.43 min, p<0.001) and total X-ray dose was reduced (3.30±1.98 vs. 6.68±5.25 Gy.cm2, p<0.001) in the ICE group. However, the total RF energy ablation time was not different between groups (ICE group: 604.56±380.46sec vs. 585.82±373.39 sec, p=0.8). The procedure duration was slightly longer in the ICE group (82.0±20.8 vs. 72.1±19.0 min, p=0.03). Procedural success was 100% (40/40) in the ICE group and 95% (37/39) in the control group. Two control patients required crossover to ICE at a prespecified point to achieve bidirectional block. There were two femoral hematomas in the ICE group and one in the control group.
The use of ICE for atrial flutter ablation is associated with less fluoroscopy time and improved ability to achieve bidirectional block compared to traditional conventional flutter ablation methods. However, it is not asoociated with reduced ablation time or overall procedure duration.
Key Words : Atrial flutter, Ablation, Intracardiac echocardiography, Fluoroscopy.
Correspondence to: Pavel Osmancik, MD, PhD Cardiocenter, Department of Cardiology 3rd Medical School Charles University and FNKV Srobarova 50 100 34 Praha 10 Czech Republic Tel: 00420-721544447 Fax: 00420-267162621 Email: pavel.osmancik@gmail.com
Pharmacological treatment of typical atrial flutter (AFL, i.e. cavotricuspid isthmus dependent atrial flutter) is rarely effective and often insufficient to control the high ventricular rate during ongoing AFL. [1] Catheter ablation of AFL has been shown superior compared to pharmacological treatment and utilizes routine catheter ablations. [2] The goal of the procedure is the creation of bidirectional block across the cavotricuspid isthmus (CTI). The single-procedure success rate is more than 90% in treated patients.
Catheter ablation of AFL has a 1-10% clinical recurrence rate, that is related to inability to create durable bidirectional block. [3]Failure of CTI ablation in many patients is largely due to the anatomy of the CTI isthmus, including: 1) a steep angle at the onset of the CTI; 2) concave shape of the isthmus; 3) unexpected pouches, and;4)a prominent Eustachian ridges.[4]
To overcome these anatomical difficulties and to increase the procedural success rate, several techniques and tools have been developed to facilitate ablation of the CTI. As shown recently, the ablation of the CTI can be made easier using 3D mapping systems [5] or steerable sheaths. [6]
Intracardiac echocardiography presents a valuable tool for coupling to electrophysiology procedures. The method was first reported for use in AFL ablationsby Chu et al. [7] The use of ICE during AFL ablation can visualize pouches, the presence of the right coronary artery, and reveal prominent Eustachian ridges. Whether the routine use of ICE is associated with a shortening of the total procedure time, and reduced fluoroscopy and radiofrequency delivery times remains unclear, and was the aim of the present study.
Patients with documented or ongoing typical AFL were eligible for the study. Patients indicated for more complex ablation procedures (e.g., concomitant pulmonary vein isolation), and patients undergoing a redo procedure for AFL were excluded. Ablations took place during ongoing arrhythmia or while the patient was in sinus rhythm. The study was approved by the local ethics committee, and all patients provided informed consent before enrollment. Patients were randomly assigned to undergo CTI ablation with ICE (ICE group), or without ICE, using a conventional fluoroscopic approach (non-ICE group). 3D electroanatomic mapping system was not used during ablations. The randomization was done using the envelope method. All procedures were performed by two surgeons who were familiar with ICE during all kind of ablations since 2010.
The electrophysiological study and catheter ablation were performed during the fasting state. Continuous ECG monitoring was performed using surface (low pass filter 0,1 Hz, high pass filter 25 Hz, and notch filter 50 Hz) and endocardial electrocardiography (low pass filter 30 Hz, high pass filter 250 Hz, and notch filter 50 Hz) at a sweep speed of 200 mm/s. Data were stored on a digital amplifier and recorder system (LabSystem PRO v2,6a EP Recording System, C. R. BARD, Lowell, MA, USA).
The duration of the procedure was defined as lasting from the initial connection of the patient to ECG monitoring in the EP lab until the withdrawal of the sheaths and final assessment of hemostasis (achieved through manual compression). In patients randomized to the ICE group, two sheaths (F6, F11) were inserted. From the left femoral vein, a 10-F phased-array ICE probe (AcuNav, Siemens,Erlangen, Germeny) was inserted into the right atrium and connected to echocardiography (Vivid Q, GE Healthcare, Wauwatosa, USA), and a 6-F decapolar catheter was inserted into the coronary sinus (Dynamic XT Catheter, Boston Scientific, Marlborough, MA, SA or ViaCath, Biotronik SE &Co.KG, Berlin Germany). The right femoral vein was used to introduce a7-F duodecapolar (halo) catheter into the right atrium (Map-iTTM TF 4/3.3F Duo-Decapolar,Access Point Technologies, Rogers, MN, USA or ViaCath, Biotronik SE &Co.KG, Berlin Germany) and a 3.5 mm irrigated-tip ablation catheter (AlCath Flux Black or Blue eXtra Gold, Biotronik SE &Co.KG, Berlin Germany) was placed in close proximity to the right atrial cavotricuspid isthmus using an 8F long sheath (Fast-CathTM SR0TM, St. Jude Medical, Plymouth, MN, USA). In patients randomized to the non-ICE group, the same decapolar, duodecapolar, and ablation catheters were inserted, however, all were inserted via the right femoral vein.
In the beginning of the ablation, the ablation catheter was positioned at the ventricular aspect of the CTI. Ablation was carried out using the power-control mode with the energy output set at 25–35 W (30–35 Watts close to the tricuspid valve, and 25 Watts close to the inferior caval vein), temperature was limited to 43 °C and the irrigation rate was 15–30mL/min, under anatomic (ICE or fluoroscopy) and electrographic guidance using the point-by-point technique, which means that the ablation catheter was not withdrawn during individual applications of energy, unless necessary (due to an increase in impedance or temperature, or catheter instability). The duration of RF energy pulses, on one location, was 40 sec. After which, the ablation catheter was slightly withdrawn, the next position was checked using ICE (if available), fluoroscopy, and local electrocardiogram.Ablationswere performed either during ongoing AFL or during sinus rhythm (pacing from the proximal CS or distal poles on duodecapolar catheter) with the procedural endpoint being a complete bidirectional isthmus block. Bidirectional block was assessed by activation sequence on duodecapolar catheter and proximal pole of CS catheter during stimulation from distal pole of duodecapolar catheter and proximal pole of CS catheter. In difficult cases,differential pacing was performed to distinguish complete from incomplete blocks. If a complete conduction block of the CTI was not present after the firstablation line, individual conduction gaps were sought out and ablated. If the block was not achieved in the non-ICE group after 10 min of X-ray,it was recommended that the ICE should be added ( without a change in surgeons. In such cases, the ICE probe was added from the left femoral vein. After block completeness, a 15-min waiting period was started, after which the block was reassessed. If the bidirectional block was maintained, the procedure was finished and all catheters and sheaths were withdrawn. If conduction remained, gaps were once again sought out andablated, and a new 15-minwaiting period was started.
Continuous variables are shown as mean ± SD. Comparisons between groups were performed using the Student’s-test, or the Mann-Whitney U-test, as appropriate. Categorical variables are shown as absolute numbers and frequencies, and were compared using the Fisher´s exact test. Statistical significance was defined as a p<0.05 using a 2-tailed comparison. Statistical analyses were done using Sigma STAT software (Systat Software, Inc., San Jose, CA, USA).
Eighty were initially enrolled in the study. Bidirectional block across the CTI was achieved in 79 (98.7%) of patients: in one patient, atrial fibrillation occurred during the procedure, and reoccurred despite IV anti-arrhythmics and electrical cardioversions; thus, in this patient, the presence of a block through the CTI could not be verified. Therefore, this patient was excluded from the analysis due to inability to test the endpoint. It means, 79 patients were included in the analysis. There were 56 (71%) men (mean age 67.7 ± 12.9 years). Ongoing AFL at the start of the ablation was present in 45(57%) of patients (mean CL 238.9 ± 25.8 ms). Forty patients were randomized to the ICE group and 39 patients to the non-ICE group. Basic clinical characteristics of both groups are shown in [Table 1]. There were no significant differences in terms of baseline characteristics between the two groups. The ablation catheter, as seen during the ICE guided ablation in one patient from the ICE group is shown in [Figure 1].
Figure 1. An example of the visualization of cavotricuspid isthmus using ICE during the ablation. A – cavotricuspid isthmus with prominent Eustachian ridge B – cavotricuspid isthmus with flat Eustachian ridge
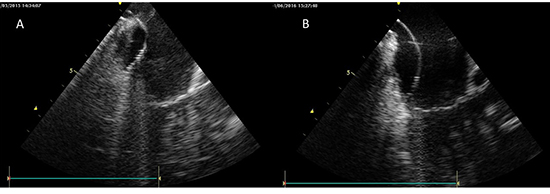
Table 1. clinical characteristics of studied patients in both groups
|
ICE (n=3440) |
No-ICE (n=39) |
P |
| Age |
68.6 ± 8.8 |
67.4 ± 9.3 |
0.55 |
| Gender (male) |
29 (73%) |
27 (69%) |
0.75 |
| LV EF (%) |
51.6 ± 13.2 |
54.2 ± 11.5 |
0.36 |
| LA size (mm) |
44.8 ± 5.4 |
44.1 ± 4.5 |
0.53 |
| Tri gradient (mmHg) |
25.9 ± 6.4 |
28.8 ± 7.3 |
0.15 |
| Mi regurgitation (moderate, severe) |
4 (10%) |
5 (13%) |
0.69 |
| History of atrial fibrillation |
14 (35%) |
13 (33%) |
0.88 |
| History of AFL (months) |
15.4 ± 26.0 |
8.9 ± 14.8 |
0.28 |
| History of heart failure |
22 (55%) |
17 (44%) |
0.31 |
| NYHA class (in HF pts.) |
1.7 ± 0.8 |
1.6 ± 0.8 |
0.89 |
| History of hypertension |
29 (73%) |
23 (59%) |
0.33 |
| Amiodarone |
7 (18%) |
4 (10%) |
0.35 |
| Propafenone |
4 (10%) |
3 (8%) |
0.72 |
| Beta-blocker |
21 (53%) |
27 (69%) |
0.13 |
| Ongoing Warfarin |
23 (58%) |
21 (54%) |
0.74 |
| LMWH |
4 (10%) |
4 (10%) |
0.97 |
| NOAC |
9 (23%) |
9 (23%) |
0.95 |
| Aspirin |
4 (10%) |
5 (13%) |
0.69 |
Data are shown as mean+SD or absolute number and frequencies. Statistical analysis was done using t-test or chi-square test.
All procedures and ablation variables are shown in [Table 2]. In the non-ICE group, eight patients (20.5 %) received more than 10 min of X-ray exposure; however, in only two of them (5%), ICE probe was added (these patients were analyzed in the non-ICE group). The addition of ICE was only recommended, not mandatory after achievement of 10 min fluoroscopy, and the final decision was left on the operator. In the two patients, in whom the ICE probe was added, not only X-ray exposure, but also the number of RF energy applications was very high (more than 1000 sec in both of them). In both patients, a CTI block was finally achieved. A concaved CTI with a prominent Eustachian ridge was observed by means of ICE. In the ICE group, the X-ray exposure longer than 10 min was present in 2 patients. Reconduction across the CTI, during the 15 min waiting period, occurred in 12 patients (6 patients in the ICE group and 6 patients in the non-ICE group, in the majority of them this occurred shortly after the first ablation line and block), however, a bidirectional block was ultimately achieved in all of these patients.
Table 2. Procedure and ablation variables
|
ICE (n=40) |
No ICE (n=39) |
P |
| Ongoing AFL at the start |
24 |
21 |
0.58 |
| Total procedure time (min) |
82.0 ± 20.8 |
72.1 ± 19.0 |
0.03 |
| X-ray time (min) |
3.29 ± 2.60 |
5.94 ± 3.43 |
<0.001 |
| X-ray dose (Gy.cm2) |
3.30 ± 1.98 |
6.68 ± 5.25 |
<0.001 |
| Nr of RF pulses |
18.6 ± 12.9 |
19.1 ± 13.7 |
0.85 |
| Energy duration (sec) |
604.6 ± 380.5 |
585.8 ± 373.4 |
0.82 |
| Length of the CTI (mm) |
28.6 ± 12.4 |
- |
|
| Reconduction |
6 (15%) |
6 (15%) |
1.0 |
Regarding complications, there were three small hematomas, two in the ICE group (5%) and one in the non-ICE group (2.5%). However, none required a transfusion of blood products or prolongation of hospitalization. Additionally, one steam pop occurred in each group without complications.
In the ICE group, the X-ray time was significantly shorter compared to the non-ICE group (3.29 ± 2.60 min vs. 5.94 ± 3.43, p=0.0003). Similarly, the radiation dose was significantly lower in the ICE group (3.30 + 1.98 Gy.cm2 vs. 6.68 + 5.25 Gy.cm2). However, the number of RF energy pulses (18.5 ± 12.9 vs. 19.1 ± 13.7) and the total RF energy duration (604.6 ± 380.5 sec vs. 585.8 ± 373.4 sec) were similar in both groups. The total procedure time was non-significantly longer in the ICE group. The total procedure time was longer in the ICE group than in the non-ICE group (82.0 + 20.8 min vs. 72.1 + 19.0 min); however, the prolongation was due to one more venous access in the ICE group.
Our main findingswere that the use of ICE significantly shortens X-ray exposure, but not the number of RF energy applicationsor the RF time. The use of ICE was 100% effective in terms ofcreation of a bidirectional block (compared to 95% effectiveness without ICE).In difficult cases that originally started without the use of ICE, the addition of ICE enabled a bidirectional block across the CTI to be achieved.
Several tools and techniques have been developed to facilitate CTI ablation. Matsuo et al. reported a reduction in time and amount of RF energy needed in a randomized study comparing steerable vs. non-steerable long sheaths for CTI ablations without different X-ray exposure. [6]Reduced ablation times and amounts of energy delivery was only seen in patients with a non-straight CTI anatomy (concave and pouch-like, determined by cardiac CT) but not in patients with “easier” straight CTI anatomy. It means, in patients with difficult CTI anatomy, steerable sheaths, due to better stability and contact, could significantly enhance CTI ablations. The use of a 3D mapping system for CTI ablation was reported by Kottkamp et al. [8] 3D mapping of CTI ablations was associated with a substantial reduction in X-ray exposure (22 min vs. 3.9 min), however, it did not lower the number of RF pulses needed to achieve a complete bidirectional block. 3D mapping systems are also not able to directly show CTI anatomy.
Because the main issue in CTI ablations has to do with difficult CTI anatomy, attention needs to be focused on methods that allow visualization of the CTI. CTI anatomy can be visualized using cardiac CT, angiography, or echocardiography.
As shown by Kajihara et al., visualization of the CTI prior to ablation, using cardiac CT, is capable of predicting difficult CTI ablations and can facilitate the formation of an ablation strategy. [4] In their study, the most difficult CTI anatomies were concaved CTI (present in 26% of patients) and pouch-like CTI (present in 16% of patients). In the second part of the abovementioned study, patients with difficult CTI anatomy, which were identified prior the ablation, were randomized to the modulation ablation technique (catheter inversion technique) or conventional technique. Modulation of the catheter shape, based on the knowledge of CTI anatomy, was associated with shortened RF application duration and lower total amounts of RF energy, as well as reduced X-ray time (14 min vs. 6.8 min). It emphasizes the importance of the knowledge of CTI anatomy for the ablation. However, cardiac CT has its own level of radiation exposure, and cannot be used in real-time during the ablation.
Another way to visualize CTI anatomy involves angiography, in which a contrast dye injection is applied via a pigtail catheter into the inferior vena cava at its junction with the right atrium (isthmogram). Unlike a cardiac CT, an isthmogram can be done directly in the EP lab. Da Costa et al. showed that isthmus characteristics, such as a concave shape or prominent Eustachian ridge, are factors that significantly increase procedure duration, X-ray exposure and the duration of required RF applications.[9]
Because of the absence of radiation exposure and real-time visualization during ablation, ICE represents an optimal tool for CTI visualization during ablations. The use of ICE during CTI ablation was reported for the first time by Chu et al. in 1994.[7]ICE, especially in patients with complicated CTI anatomy, can make ablations feasible, even in patients with a history of unsuccessful ablations. [10]Recently, Bencsik et al. reported a randomized study similarly designed as ours. [11] In contrast to our results, they found not only lower X-ray exposure, but lower RF energy application in patients ablated with ICE.In contrast to our study, Bencsik et al. reported higher overall X-ray times (18.6min in the conventional group, and 5.5min in the ICE group). In our patients ablated without ICE, the X-ray time of 5.9 ± 3.4 min was closer to the X-ray time of patients ablated with ICE in Bencsik´s study. In this context, thesignificant reduction of X-ray exposure seen in our study, i.e., 3.29 ± 2.6 min in our ICE group, is of importance and could be achieved only by a new tool added to conventional setting. The RF duration time in our study (604.6 ± 380.5 sec, or 585.8 ± 373.40 sec, resp.) varried between the values reported by Bencsik for their ICE and conventional groups (i.e., 482.8 ± 534.1 in the ICE group and 779.7 ± 620.8 sec in the conventional group). The explanation of lower X-ray exposure, but unchanged RF energy application between ICE and non-ICE groups in our study, could have been due to the ablation technique used in our lab (point-by-point approach). With the point-by-point technique, ICE is used for catheter visualization (i.e. instead of X-rays), however, it is not used to assess the formation of the RF lesion.
Thirteen percent of the conventionally ablated patients in the Bencsik´study, and 5% of our patients had to be switched to the ICE approach in order to complete the bidirectional block. In our study, the efficacy of CTI flutter ablation was 100% in the ICE group, and 95% in the non-ICE group (up to switch to the ICE approach). We can´t conclude that the ablation in those patients would have been unsuccessful without the switch to ICE; however, the addition of ICE facilitated a successful ablation result.
The total procedure time was longer with ICE than without using it. However, in the ICE group, there was one more vein puncture, and because the total procedure time was calculated until successful hemostasis, the prolongation of the procedure was caused by additional vein puncture and adequate hemostasis. Importantly, in the ICE group, no more major vascular complications were observed, despite having one more 11F vein puncture in patients on anticoagulation.
Over the last year, the awareness of the risk related to the use of ionizing radiation in medicine has progressively increased. According to a survey undertaken in Italy, interventional cardiologist and electrophysiologist represent more than 60% of the medical staff receiving the highest annual radiation exposure, with no statistical difference between physicians, nurses and technicians. [12] Due to both the stochastic and deterministic effect of radiation, there is no magnitude of radiation exposure that is known to be completely safe and, the use of radiation exposure should be As Low As Reasonably Achievable (ALARA principle). This principle confers to physicians the responsibility for reducing as much as possible the dose of radiation during cardiovascular procedure, in order to minimize the radiation injury of the patients as well as of the medical staff. ICE represent an excellent tool for on-line visualization of the anatomy of the area of interest, ablation and other catheters without any exposue of radiation, and so could be considered even for conventional ablation in any patient.
The use of ICE for atrial flutter ablation was associated with less X-ray exposure and reduced total X-ray dose, but did not reduce the total radiofrequency energy ablation time. The use of ICE for atrial flutter ablation was 100% effective in terms ofcreation of a bidirectional block. Moreover, in difficult cases (in patients with an unsuccessful ablation using fluoroscopy), the addition of ICE was effective in creating a bidirectional block across the cavotricuspid isthmus.
The work was supported by a research grant of Charles University PRVOUK P 35.






