Cardiac electronic implantable device (CIED) infections are devastating, contribute to morbidity and mortality, and are potentially disfiguring for patients.[1] The focus of this document is first to review contemporary information describing incidence, prevalence and microbiology of CIED infections, and then to describe the role of novel therapeutic options developed to reduce this type of complication.
Incidence, Prevalence, and Microbiology
CIED infections encompass a spectrum of possible local and/or systemic findings.[2],[3] The clinical presentation can range from the common indolent infection to the rare presentation of acute sepsis syndrome.[3],[4]
One paradigm for categorizing these infections is based on the involved device or anatomic structures. For example, a pocket infection is generally characterized by findings localized to the soft tissue and may or may not have associated bacteremia. In contrast, endocarditis includes the presence of bacteremia with the involvement of vascular or cardiac tissue demonstrated with imaging such as transthoracic or transesophageal echocardiography. Imaging demonstrates lesions or masses on native tissue or associated with endocardial leads. However, abnormalities on imaging in the absence of bacteremia or signs of infection are not diagnostic of CIED infection. The spectrum of CIED infection also includes hematogenous seeding of endovascular leads from remote sources of infection, such as osteomyelitis.
CIED infections can also be described using the Center for Disease Control’s (CDC) definition of surgical site infections.[5] The criteria for superficial incisional, deep incisional, and organ/tissue infection are shown in [Table 1]. As most CIED procedures involve the continued presence of an implanted device, the time course for the development of such an infection is out to one year after the procedure. Although a positive wound culture is not always present in situations where the device has eroded through the skin, it is important to note that these are, by expert consensus, considered infected systems.[4] [Figure 1] is an example of an erosion. In cases of erosion, negative cultures may be due, in part, to the prior use of empiric antibiotics for localized swelling or redness
Table 1. Center for Disease Control Definitions of Surgical Site Infections (SSI)5
|
Superficial Incisional SSI: Limited to skin or subcutaneous tissue
|
|
Onset within 30d of procedure or operation
|
|
Presence of at least one of the following:
|
|
Purulent drainage from the incision
|
|
Organism identified from aseptically obtained fluid or tissue (+ gram stain or culture)
|
|
At least one clinical sign of infection such as pain, tenderness, swelling, redness, warmth
|
|
Diagnosis of superficial incisional SSI by surgeon or attending physician
|
|
Deep Incisional SSI: Involves deep tissue layers such as muscle or fascia
|
|
Onset within 30d of procedure or operation if no implant left in place with infection related to procedure or operation
|
|
Onset within 365d of procedure if implant left in place with infection related to procedure or operation
|
|
Presence of at least one of the following:
|
|
Purulent drainage from deep in the incision
|
|
Spontaneous dehiscence
|
|
At least one clinical sign of infection such as temperature > 38 C,pain, tenderness, swelling, redness, warmth
|
|
Abscess or evidence of infection seen on direct examination or imaging
|
|
Diagnosis of deep infection by surgeon or attending physician 1.6% respectively,(P< 0.0001).[9]
|
|
Organ/Space SSI: involves organ or space manipulated during operation or procedure exclusive of incision
|
|
Onset within 30d of procedure or operation if no implant left in place with infection related to procedure or operation
|
|
Onset within 365d of procedure if implant left in place with infection related to procedure or operation
|
|
Presence of at least one of the following:
|
|
Purulent drainage from a drain placed into the organ or space
|
|
Organism identified from aseptically obtained fluid or tissue culture (+ gram stain or culture) from organ/space
|
|
Abscess or evidence of infection seen on direct examination or imaging
|
|
Diagnosis of organ/space infection by surgeon or attending physician
|
Figure 1. Pacemaker pocket with erosion.Generator and lead with suture sleeve vistible. Notice the lack of surrounding erythema

The incidence of CIED infection for initial implants has been determined from prospective randomized trials of pre-incisional intravenous antibiotics. One of the first randomized trials of intravenous antibiotics, reported in 1981, randomized patients who were scheduled to have a transvenous pacemaker implanted, to both intravenous flucloxacillin and intramuscular benzylpenicillin or to no antibiotics.[6] Two hundred and thirty four patients received antibiotics and one hundred and ninety-seven did not. Infection rates were 0.8% for the antibiotic treated group and 3.6% in the group who did not receive antibiotics. A similar infection rate was seen in the more contemporary randomized trial of cefazolin reported in 2009.[7] In that prospective randomized trial, the overall incidence of infection was 2% with a rate of 0.6% in the cefazolin arm and 3.2% in in the placebo treated group. The incidence of infection after generator replacement has also been prospectively determined. The REPLACE Registry, a prospective multicenter registry that enrolled and followed 1744 patients after pacemaker or ICD generator replacement, revision, or upgrade, described an infection rate of 1.3%.[8]
The prevalence of CIED infection varies among published series, by duration of the follow-up period, and by CIED type. For example, in a sample of single, dual and cardiac resynchronization defibrillators from the American College of Cardiology Foundation National Cardiovascular Disease Registry (NCDR) and matched Medicare claims data, the prevalence of an infection was 1.7 % over a three year period.[9] The infection rate in single chamber devices was 1.4%, in dual chamber devices 1.5%, and in CRT devices 2.0%; (P<0.001). This analysis also demonstrated that the infection rate for generator replacement procedures was greater than initial implants, 1.9% vs 1.6% respectively, (P < 0.0001).[9]
Causative organisms for CIED infections can result from migration from the pre-axillary flora or from hematogenous seeding. The role of the pre-axillary flora as a potential reservoir of microorganisms is found in an elegant analysis from Da Costa and colleagues.[10] Three bacteriologic specimens were taken from each patient: first from the skin prior to skin antisepsis, second, from the pocket at the time of formation; , and third, from the pocket at the time of generator insertion. Patients were followed for the development of an infection. Skin antisepsis in this series was with both a 10% and subsequent 7.5% solution of povidone iodine. Overall, preoperative skin cultures were positive in 88.3% of samples; in 48% of samples obtained from the pocket prior to generator insertion and in 37% of samples obtained again prior to skin closing. The rate of clinical infection in these patients, who, incidentally, were not treated with pre-incisional intravenous antibiotics, was 4.5%. In 60% of the patients who developed a clinical infection, the organism cultured at the time of the procedure was present in the screening cultures. The dominant organisms in the positive cultures were of staphylococcal species, followed by enterococci and streptococcus viridans.
A recent retrospective series of CIED infections from one tertiary referral center, similarly reported a preponderance of staphylococcal infections. [11] Coagulase negative staphylococci identified in 18.8% of the cultures, methicillin-sensitive staphylococci aureus in 15.8%, methicillin resistant staphylococci in 15.0%, and methicillin resistant coagulase negative staphylococci in 18.8%. The remaining organisms cultured were atypical organisms such as vancomycin resistant enterococcus, or gram negative organisms. Cultures negative for an identifiable organism were seen in 13.2% of the cases.[11]
Risk Factors for infection
This identification of risk factors and the strength of association with infection is dependent upon the factors collected and the infection rate. Risk factors for the development of CIED infection can be characterized as patient factors or procedural factors. Recognized patient risk factors include the presence of a fever within twenty-four hours of the implant procedure, chronic kidney disease, diabetes mellitus, steroid use, prior valve surgery, chronic lung disease, cerebrovascular disease, and development of a clinically significant hematoma.[7],[8], [12]-[14] A specific analysis of ICD infections from the NCDR in over 200,000 patients identified prior valve surgery, cerebrovascular disease, chronic lung disease, and renal replacement therapy with hemodialysis as independent risk factors for infection.[9]
Procedural factors that have been associated with infection include the presence of a temporary wire, need for re-intervention, use of drains, or multiple procedures.[9], [14],[15]
Antibiotics: Intravenous, intra-procedural, post-procedural, skin antisepsis
In addition to proper surgical technique, intravenous pre-incisional antibiotics is fundamental for prevention of CIED infection is pre-incision intravenous antibiotics. Prior to 1994, the data supporting the use of intravenous antibiotics was variable.[6], [16] In 1994, Drs. Mounsey and colleagues reported one of the first prospective randomized trials that demonstrated a benefit of pre-incision antibiotics. In this trial, four hundred and thirty-one patients were randomized to administration of flucloxacillin or clindamycin, or no antibiotic, administered pre-operatively and continued for forty-eight hours post procedure. The infection rate was 0% in the patients treated with antibiotics and 4% (p= 0.003) in the patients randomized to no antibiotic treatment.[15] In 2009, the landmark de Oliveria prospective double-blind placebo-controlled trial of pre-incisional antibiotics before implantable cardioverter defibrillator or pacemaker procedures was published. This trial planned to randomize 1000 patients with follow-up out to six months. The definition of infection included superficial infection of the pocket with the presence of purulence and no systemic manifestations, pocket infection with positive microbiological culture findings, and systemic infections. The infection rate was 0.63% in the antibiotic treated arm and 3.28% in the placebo arm (p=0.016). The trial was halted after 649 patients due to a significant difference in infection rate favoring the antibiotic treated arm. In 2010, the American Heart Association published a Scientific Statement “Update on Cardiovascular Implantable Electronic Device Infections and Their Management” and recommended that a parenteral administered antibiotic be given 1 hour before the procedure.[4]
Less well evaluated is the role of intra-procedural antibiotic irrigation and post-procedural parenteral or oral antibiotics. The use of wound irrigation in contaminated wounds stems from battlefield medicine experience. Despite anecdotal experience with this practice, the effect of intra-procedural wound irrigation for prevention of CIED infection has not been specifically evaluated to date.[16] Similarly, post-operative antibiotics have been included in prior trials of parenteral antibiotics, but the effect of post-procedural antibiotic administration on the subsequent infection rate was not evaluated, possibly due to the low absolute number of infections.[15] In the prospectively designed REPLACE trial which included a pre-specified infection analysis, a higher infection rate was seen in patients treated with post-operative antibiotics. However, in this registry, the use of any or no post-operative antibiotics was left to the individual investigator, thus limiting any specific conclusions.[8]
The on-going PADIT Trial will prospectively evaluate the practice of post-operative antibiotic administration to reduce CIED infection. This investigative strategy involves an investigative center based cluster crossover design to evaluate the role of incremental antibiotics before during and after the CIED procedure. Each implanting center will be randomized to pre-incision cefazolin (or vancomycin in penicillin allergic patients) alone, or with intra-operative bacitracin 50,000 U in normal saline wound irrigation and a two day post-operative course of oral cephalexin, or clindamycin in penicillin allergic patients. Patients eligible for inclusion are those who present for generator replacement, revision or upgrade procedures or cardiac resynchronization procedures.[17]
Skin antisepsis is another recognized tool in reducing surgical site infections. Two current formulations are available in contemporary practice, povidone iodine, and chlorhexidine gluconate. Povidone-iodine is a complex of bactericidal iodine and a synthetic polymer.[18] Chlorhexidine gluconate is both bactericidal via lysis of cell membranes, and is also bacteriostatic. To date, there have been no randomized prospective evaluations of these two agents in CIED procedures. A randomized trial performed in adult patients undergoing clean contaminated surgery in the gastrointestinal, urologic abdominal surgery, and non-abdominal surgery, demonstrated an overall surgical site infection rate of 9.5% in patients treated with chlorhexidine alcohol and 16.1% in the povidone-iodine treated patients (p= 0.004).[19] The type of skin antisepsis was also prospectively collected in the REPLACE Registry. In that pre-specified infection analysis, all patients received pre-procedural antibiotics. Centers with infection rates greater than 5%, were sites more likely to use povidone iodine as a skin antiseptic where chlorhexidine gluconate use was more prevalent at low infection rate sites. However, a subsequent single center retrospective analysis from the Cleveland Clinic of 2,792 CIED patients, demonstrated an identical infection rate of 1.1% at one year irrespective of skin antisepsis with povidone iodine or chlorhexidine gluconate.[20]
Procedural approaches to preventing CIED infections
Optimizing patients’ clinical status prior to device placement is good clinical practice; a prolonged procedure during acute decompensated heart failure is unlikely to improve compromised cardiac or pulmonary status. Yet, eliminating medical comorbidities is unrealistic, so targeting procedural factors may be an alternative approach in attempts to reduce infection. Changes in battery chemistry to improve longevity, algorithms to reduce ventricular pacing, and evoked response algorithms to allow lower pacing output voltages are a few approaches that may indirectly reduce infection by reducing the number of procedures patients face over their lifetime.
The development of a hematoma after CIED implant has been associated with increased length of hospital stay, increased hospitalization costs, and greater in-hospital mortality.[21] Importantly, hematoma development has been intermittently identified as a risk factor for the development of a CIED infection in multiple trials. The development of a post-operative hematoma was identified as a risk factor for infection in the REPLACE Registry.[8] The recently published BRUISE CONTROL INFECTION study demonstrated an infection rate of 11% in patients who developed a clinically significant hematoma, compared to an infection rate of 1.5% in patients who did not develop a hematoma, corresponding to a greater than seven fold risk of infection if a hematoma develops.[13]
Strategies to reduce hematomas are recommended in the AHA guidelines, such as meticulous electrocautery to control local bleeding, use of pressure dressings, and evacuating the device pocket if impending dehiscence.[4] Due in part to the BRUISE CONTROL Trial, minimizing the use of heparin products in the peri-procedural period is now standard of care.[22]
The use of topical hemostatic agents is common in surgical practice.[23] Limited data in pacemaker and ICD patients is available. Interestingly, one prospective trial of a topical hemostatic agent after CIED implant was terminated early due to the increased risk of infection, and it did not reduce the incidence of pocket hematoma.[24] Conversely, a smaller retrospective series utilizing oxidized regenerated cellulose resulted in no hematomas nor infections.[25]
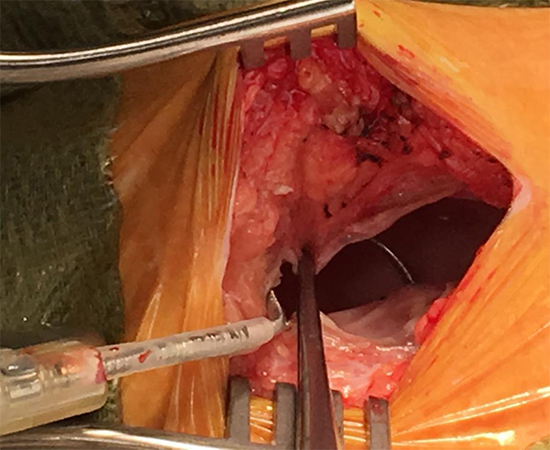
Wound healing requires a multi-step series of biological processes that ultimately result in the restoration of tissue integrity. The phases of wound healing begin with inflammation, re-epithelialization, keratinocyte proliferation, matrix metalloprotinease deposition, angiogenesis, and ultimately wound contraction and closure.[26] Furthermore, the body’s ultimate response to a retained foreign object is a complex multi-phase inflammatory response that involves expression of transforming growth factor-B, and finally results in fibrosis. This end result is recognized as a capsule as shown in [Figure 2A] and [Figure 2B]. This fibrotic avascular capsule has been implicated as a potential source of infection due to the presence of bacterial colonization.[27] Based on this, one potential approach to reduce infection is to consider excision of this fibrous capsule at the time of generator replacement. This concept was recently evaluated in the prospective randomized single-center MAKE IT CLEAN trial.[28] Eligible patients were those who were to undergo device replacement, upgrade, or lead extraction. The randomization was between pocket revision or no pocket revision. Pocket revision was defined as complete capsule excision which included removal of the floor and roof of the capsule, and included removal of all fibrous tissue surrounding the leads and lead anchoring sleeves. All patients received pre-incisional antibiotics within one hour of the procedure. Skin antisepsis was chlorhexidine, and all pockets were irrigated with the same antibiotic that was administered prior to the incision. The use of topical hemostatic agents and the strategy for peri-procedural management of anticoagulants was at the discretion of the implanting physician. The primary endpoint was the presence of a deep pocket infection. The secondary endpoints included the presence of a superficial pocket infection, hematoma, prolonged serosanguinous drainage for greater than three days, or mortality within the one year following the procedure. Two hundred and fifty-eight patients were randomized with one hundred and thirty-one to the pocket revision group and one hundred and twenty-seven to the no revision group. Eleven patients crossed over to the other groups due to specific operative findings. Not unexpectedly, these findings included: i) a thin anterior capsule seen in frail patients that precluded pocket revision; or ii) the presence of significant adherent tissue that required removal to enable lead revision. Procedure types were similarly distributed between the pocket revision and no revision groups, and there was no statistically significant difference in procedure duration. At the one year follow-up, no deep-space infections were seen in either group, which persisted at a mean follow-up of 33± 76 months. The superficial infection rate was not statistically different between the two groups (1.5% in pocket revision group, 4.7% in non- revision group, P= 0.13). Similarly, mortality was no different with three deaths in the pocket revision group and one death in the no-revision group (P=0.3). Serosanguinous discharge for greater than three days was more common by a factor of ten in the no revision group (7% versus 0.7% in the pocket revision group, P= 0.004). The hematoma rate in the pocket revision group, 6.1%, was markedly greater than the 0.8% observed in the no-revision group (p=0.03), and two patients who had the pocket revision required a second procedure for hematoma evacuation. No patient who developed a hematoma in either group was “bridged” with heparin or enoxaparin. Thus, routine pocket revision with capsulectomy is not recommended as a preventative strategy to reduce CIED infection, and increases the risk of pocket hematomas.[28] It is important to clarify, however, that in the presence of an existing deep pocket infection, debridement of all infected tissue is imperative for complete eradication.
Figure 2A. Intra-operative view demonstrating the capsule The Adson’s forceps are grabbing the superior surface of the fibrotic capsule
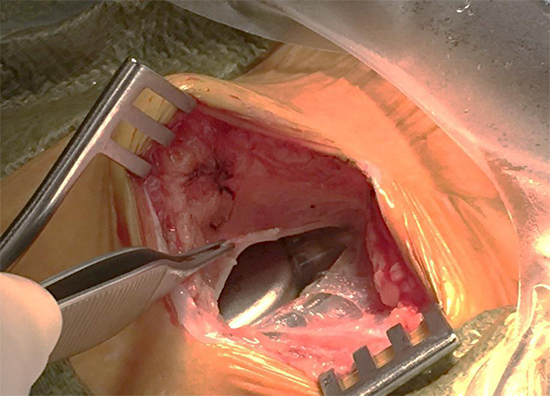
Figure 2B. Intra-operative view of capsule after generator and lead were removed. The blue arrow head identifies the surface of the fibrotic capsule.
Pocket-based interventions
Pocket based interventions as a technique to reduce infections have been a source of interest for a number of years. One such intervention is the prophylactic use of a removable drain such as red rubber catheters, Penrose, or other small catheters. In a retrospective series of 288 patients from a single center in which drains were used in half of the population, the nine patients who developed an infection all had prophylactic drains placed during their procedures.[29] More recently, an envelope or pouch of porcine small intestinal submucosa extracellular matrix, the CorMatrix® CanGaroo™ Cardiovascular Device Pocket, has been available for use in cardiac surgical procedures.[30], [31] Its proposed use in CIED procedures is for pocket stabilization and reinforcement. There are no data to date on its impact on CIED infections. Similarly, antibiotic impregnated suture is available, with no clinical trials in CIED infections. Topical dressings that include silver have likewise not been systematically evaluated in CIED procedures, and are generally reserved for situations of delayed wound healing due to elevated microbial burden.[32]
As discussed in section IIa above, intravenous antibiotic administration prior to skin incision is crucial in preventing CIED infection. Topical antisepsis and pocket irrigation are short term measures; the contact time with the wound is relatively short. More prolonged local delivery of antibiotics to the pocket is one of the contemporary approaches to reducing CIED infection. The antibacterial envelope is one such approach, and is comprised of a polypropylene mesh with a bio-absorbable polymer embedded with minocycline and rifampin. Rifampin inhibits bacterial RNA synthesis by binding to the beta subunit of DNA polymerase. Minocycline, a tetracycline derivative, inhibits bacterial protein synthesis. Both agents are active against staphylococci. This envelope is designed to release the antibiotics over seven days. The current version is a mesh that is fully resorbable at 9 weeks, with no systemic absorption.
This antibacterial envelope has been evaluated in multiple retrospective cohort series. One of the first series described 642 patients undergoing pacemaker, ICD or CRT procedures who were implanted with the original non-resorbable, antibacterial pouch.[33] Three major infections developed; all three patients had three or greater risk factors for infection. A subsequent case control series of 260 patients and 639 controls from Vanderbilt University demonstrated an infection rate of 0.4% in the patients who received an antibacterial envelope versus a 3.0% infection rate in the controls (P=0.044).[34] Propensity matching was done in a 209 patient subset with similar results, 0.5% infection rate in the envelope treated patients and 4.3% in the controls, P=0.035.[34] A subsequent propensity based single center evaluation also demonstrated a significant reduction in the likelihood of infection at 6 months with use of the envelope, 1.1% versus 3.6% in matched controls, P= 0.048). [35] The on-going WRAP IT Trial, [NCT #02277990] a multicenter prospective randomized trial, is evaluating the resorbable antibacterial envelope in dual low power or high power generator replacements and initial cardiac resynchronization device implants in up to 7,764 subjects from 225 world-wide sites. For this trial, CIED infection is defined as 1) superficial cellulitis in the region of the CIED pocket with wound dehiscence, erosion, or purulent drainage, 2) deep infection as defined by the surgical site infection definitions discussed earlier, 3) persistent bacteremia, or 4) endocarditis. The primary endpoint is the major infection rate at 12 months, with secondary endpoints of procedure-related, and system related complication rates, as well as infection rates over the entire follow-up period.
Figure 3. Tyrex TM resorbable antibiotic envelopes







