Brugada Syndrome:Risk Stratification And Management
Yoshifusa Aizawa, MD, PhD
Research and Development, Tachikawa Medical Center. Nagaoka, Japan.
The Brugada syndrome (BrS) is an arrhythmogenic disease associated with an increased risk of ventricular fibrillation and sudden cardiac death. The risk stratification and management of BrS patients, particularly of asymptomatic ones, still remains challenging. A previous history of aborted sudden cardiac death or arrhythmic syncope in the presence of spontaneous type 1 ECG pattern of BrS phenotype appear to be the most reliable predictors of future arrhythmic events. Several other ECG parameters have been proposed for risk stratification. Among these ECG markers, QRS-fragmentation appears very promising. Although the value of electrophysiological study still remains controversial, it appears to add important information on risk stratification, particularly when incorporated in multiparametric scores in combination with other known risk factors. The present review article provides an update on the pathophysiology, risk stratification and management of patients with BrS.
Key Words : Brugada Syndrome, Risk Stratification, Electrophysiological Study, Sudden Cardiac Death.
Correspondence to: Yoshifusa Aizawa, Research and Development, Tachikawa Medical Center. 3-2-11, Kanda-cho.
Brugada syndrome (BrS) is an inherited arrhythmogenic disorder characterized by an elevated ST-segment and J-point in the right precordial leads of an electrocardiogram (ECG) in the absence of structural heart disease, and it may cause sudden cardiac death due to ventricular fibrillation (VF).[1] Currently, BrS is diagnosed using criteria from the second consensus report, which was released in 2005.[2] According to the report, the new diagnostic criteria require typical ECG changes in one precordial lead.
Since BrS was described in 1992, a tremendous number of BrS cases have been reported,up to 1–5/10,000 worldwide.[3-4] Mastuo et al. investigated 4,788 subjects (1,956 men and 2,832 women) who were < 50 years old in 1958 and had undergone biennial health examinations, including electrocardiography, through 1999. The prevalence and incidence of the BrS ECG pattern were 146.2 in 100,000 persons and 14.2 persons per 100,000 person-years, respectively.[5] The average age at presentation of BrS was 45 ±10.5 years, with a peak at 30-40 years of age, and the incidence was nine times higher among men than women.
The implantation of cardiovertor defibrillator (ICD) is the only reliable therapeutic modality to prevent sudden cardiac death from cardiac arrest (CA).[6-8] ICD is clearly indicated for those with prior CAof VF. However, for asymptomatic patients with BrS, a risk stratification is needed. This article reviews the current status of risk stratification for BrS and management of the patients.
BrS patients with a history of CA carry the highest risk for recurrence of CA (Figure-1), and implanting ICD is considered a necessary precaution.[6-8]
Figure 1: The averaged annual rate of arrhythmic events in Brugada syndrome (BrS) from the literature
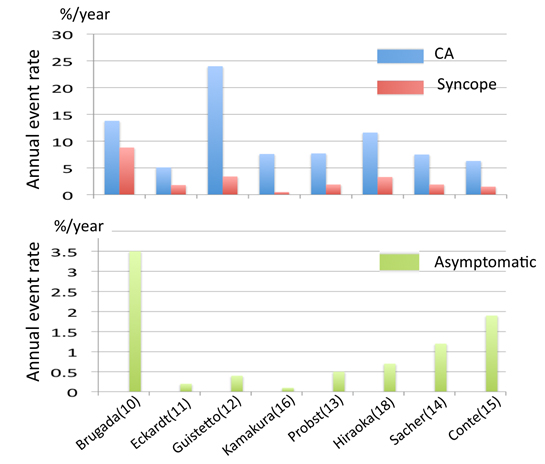
Upper column. The annual event rates of BrS patients with prior cardiac arrest (CA) (blue) and those with syncope (red). Lower column. The event rates of pateints with asymptomatic BrS. Sacher and Conte are providing the event-rates after ICD implantation. The numericals in the parenthesis is the reference number in the text.
In the first report by Brugada et al.[9] in 1998, VF recurred in 34% of symptomatic patients with previous CA or syncope during a follow-up period of 34 months with 12 % recurrence per year. In their subsequent report in 2002,[10] 12 (62%) out of 71 patients who presented with CA developed new arrhythmic events during a mean follow-up period of 54 months (13.8% per year). In the study of Eckhardt et al.,[11] the arrhythmic event rates of patients with aborted sudden death was lower: 5.1% per year. The risk of recurrent VF among patients presenting with CA can be estimated as 10% at 4 years,[12,13] and >40% at 7 years.[14-15] The mean time from presentation to VF recurrence was 1.5-2 years,[15-16] but late recurrence (>5 years after the initial event) was not rare. Similar event rates were observed in studies from Japan: 8.4 % to 11.6% per year.[16-18]
VF storms defined as ≥ 3 separate VF episodes within 24 hours have occured before and after ICD implantation in up to 24 % of the patients with appropriate ICD shocks.[15,16,19] In the series with the longest follow-up ≥5 years for 75% of the patients,[20] VF storms occurred in 12 % of those initially presenting with CA. Of the 22 men with BrS who presented with VF storms, 12 patients (54.5%) suffered VF recurrences at 21 ± 24 months after the first arrhythmic storms whereas only 1 (5.9 %) out of 17 patients with a history of a single VF episode suffered VF recurrence.[19] Spontaneous type I ECG patterns and J waves were found in 77.3% and 36.4 % of patients with VF storms vs. 28.2 % (P < 0.0001) and 9.1 % (P=0.0007) in age- and sex-matched controls of BrS patients without VF storms, respectively. Patients with ES are at risk of VF storm recurrence.[15,16,19]
Patients with a personal history of aborted sudden death have a substantial risk for recurrence of arrhythmic events and the implantation of ICD is indicated as Class I.[6-8]
Arrhythmic (or malignant) syncope is suspected in the absence of prodromes and specific triggering circumstances when a brief loss of consciousness occurs with a rapid return. Sacher et al.[20] defined syncope based on a clinical impression as “probably arrhythmic,” “probably vagal,” or “syncope of unclear mechanism” in 40%, 30%, and 30% of patients, respectivel, including 57 BrS patients. VF occurred during follow-up in 22% of the patients with presumed arrhythmic syncope but in none of the other patients.
In another study of 118 patients with syncope,[21] 12% of those presumed to have arrhythmic syncope, but none of those with “non-arrhythmic syncope”, developed VF during the follow-up period 4.5 years. Take et al.[22] studied 84 patients with type 1 electrocardiograms and syncope (41 patients with prodrome and 43 patients without prodrome), and followed the patients for 48 ± 48 months. Syncope due to VF recurred in 13 patients among patients with unexplained syncope and was more frequent in the non-prodromal group than in the prodromal group. Blurred vision (hazard ratio [HR] 0.20) was negatively associated with VF occurrence and abnormal respiration (HR 2.18) or fragmented QRS (HR 2.39) was positively associated with VF occurrence.
Vagal syncope can occur in patients with BrS with concomitant accentuation of the ECG pattern in BrS.[23] A detailed clinical history at the time of syncope is essential to distinguish benign syncope from malignant syncope.
Priori et al. analyzed risks of cardiac events in 200 patients withy BrS;130 probands and 70 affected family members, and observed that the association between syncope and spontaneous ST-segment elevation was the strongest risk for cardiac events,[24] and this was confirmed by other workers: a risk for recurrence of arrhythmic events that ranges from 2.6-6.4% with an annual rate of 1.4-4.0 % per year as shown in Figure-1.[11,12,16-19,25-29] Some investigators propose syncope in patients with spontaneous type 1 ECG or fragmented QRS is a predictor of arrhythmic events,[24-27] whereas others do not believe there is enough evidence to support the connection denied by others.[30-31]
In BrS, ICD implantation can be considered useful in patients with a history of syncope judged to be likely caused by ventricular arrhythmias.[8]
A diagnosis of BrS is confirmed by the presence of a type 1 pattern, which is a coved-type ST elevation (≥ 2 mm) descending slowly and emerging into a negative T with little or no isoelectric separation, in ≥ 1 precordial leads (V1 to V3) at the 4th, 3rd, 2nd intercostal spaces, either spontaneously or following administration of sodium channel agents.[2] In addition to its diagnostic value, some ECG markers have been studied as risks for arrhythmic events in asymptomatic BrS.
Spontaneous Type 1 ECG Pattern
In the FINGER study,[13] 1,090 patients were recruited from 11 tertiary centers in 4 European countries (745 men; 72%) with a median age of 45 (35 to 55) years. The inclusion criteria consisted of a type 1 ECG present either at baseline or after drug challenge. During follow-up up of 31.9 (14 to 54.4) months, the cardiac event rate per year was 7.7% in patients with aborted CA, 1.9% in patients with syncope, and 0.5% in asymptomatic patients. The aforementioned symptoms and spontaneous type 1 ECG were predictors of arrhythmic events, whereas gender, a familial history of SCD, the inducibility of ventricular tachyarrhythmias during electrophysiological study, and the presence of an SCN5A mutation were not predictors.
Curio et al.[32] studied 64 subjects who were diagnosed with BrS from ECGs with high intercostal spaces. The mean age from the last follow-up was 42±11 years. A typical ECG pattern was recorded at baseline in 4 subjects before a drug-challenge with sodium-channel blockers. Of those 4 subjects with spontaneous abnormal ECG, 3 experienced cardiac events.
Drug-Induced Type 1 ECG Pattern
In the PRELUDE study,[26] none of the asymptomatic patients with drug-induced type I ECG developed arrhythmic events during the 3 years of follow-up, regardless of VF inducibility at EPS. Curio[32] observed that none among the 60 patients with drug-induced ECG pattern from high intercostal spaces experienced cardiac events. Thus, patients with spontaneous type I ECG consistently have twice the risk of arrhythmic events than patients who develop a type 1 ECG pattern when challenged with a sodium-channel blocker.[13,14] ICD implantation was not indicated in asymptomatic BrS patients with a drug-induced type I ECG in the expert consensus statement.[8]
Fragmented QRS complexes (f-QRS) are defined as ≥ 4 spikes in the QRS by Morita et al.[33] or as ≥2 spikes in the QRS of V1, V2, or V3 by Priori et al.[26] Morita[33] noted that f-QRS was more frequent in patients with BrS than in controls with right bundle branch block (RBBB) (43% vs. 3%), and particularly among BrS patients with CA (85%). Its presence was associated with an increased risk of arrhythmic events. In the PRELUDE study,[26 a prospective evaluation of 308 patients without CA (including 65 with syncope and 243 with no symptoms) revealed that patients with f-QRS were associated with a 9 times higher risk for VF recurrence. f-QRS is a promising predictor for arrhythmic events,[26,33-35] but may needs a further study before it can be declared a criterion for justifying ICD implantation in asymptomatic patients with BrS.[8]
Early Repolarization Pattern (ERP)
Notch or slur at the terminal part of the QRS complex often represents early ERP. ERP was observed in 3 of the 8 patients with idiopathic VF in 1993,[36] and recently the association was confirmed by a larger study by Haissaguerre et al.[37] The dynamic characteristics of ERP were also shown in idiopathic VF patients[38] ERP can be observed in healthy individuals, and ERP with horizontal or down-sloping ST was cennected to the malignant type of ERP.[39,40]
ERP can coexist with BrS, and Sarkozy et al.[41] observed that 15% of patients with BrS had ERP in the inferolateral leads. Kamakura et al.[16] observed a similar prevalence of ERP in BrS. ERP was associated with a 4-fold increased risk of VF recurrence. Similarly, Takagi et al.[42] reported that the risk was 11 times higher in BrS when the patients had inferolateral ERP with horizontal pattern. Some researchers have suggested inferolateral ERP is a risk for VF recurrence,[16-43] but other researchers do not support this view.[44] Patients with VF storms were associated with a higher prevalence of ERP:36%.[19] During the follow-up of 22 patients presenting VF storms, 44% had recurring VF storms within the mean follow-up time of 21±24 months. When ERP is found in patients with BrS, either ERP or BrS can be a trigger of VF. Recently, we experienced a patient with BrS combined with prominent slurs, and marked and transient ERP was considered a trigger for VF storm.[45]
A wide QRS in lead V2 (≥ 120 ms );[46] the duration of the S-wave in lead I,[47] the r-J interval in lead V2 ≥ 90 ms and the QRS width in V6 ≥ 90ms;[48] aVR sign[49] or Tpe interval[50] were found to be good predictors of VT/VF, but these factors need to be confirmed by a larger study. Complete RBBB may coexist with BrS and unmasks the ECG pattern of BrS.[51] The prevalence and prognostic significance as well as the pathophysiology of this comorbidity needs to be explored.
Late potentials in a signal-averaged ECG are often found in BrS,[52,53] but the predictive value is considered limited. An increased TWA at night was observed more frequently among Brugada patients with a history of CA,[54] but its prognostic significance was limited.[54,55]
Electrophysiological Study
VF has been induced in 68-83% of symptomatic and in 33-39% of asymptomatic patients with BrS, and earlier studies suggested that the inducibility of VF during EPS is a risk for VF occurrence during follow-up.[10-12,56-59] However, other studies showed a negative or limited value for VF induction.[8,13,14,16,26] The VF inducibility might be affected by four factors:
The site of stimulation.
The number of extrastimuli.
The coupling intervals of extrastimuli and
The use of antiarrhythmic agents.
When the hearts of the patients with BrS was stimulated, a bigger conduction delay occurs in the right ventricle compared to the left ventricle,[60] and a conduction delay within the ventricle begins at longer coupling intervals of premature stimuli in BrS compared to non-BrS patients.[61] These findings support the existence of electrophysiological heterogeneity within the heart of BrS, and this heterogeneity may affect the responses to electrical stimulation during EPS.
To avoid non-specific results, some workers prefer the apex of the right ventricle for stimulation. Sieira et al.[59] updated their long-term follow-up data in 273 patients with asymptomatic BrS who underwent EPS only from the RVA and were followed for up to 15 years. The positive and negative predictive values of VF induction from the RVA for foreseeing arrhythmic events were 18% and 98%, respectively. However, the association between the site of VF induction (RVA vs. RVOT) and subsequent arrhythmic events was not evident in the studies of Makimoto et al.[62] and Kamakura et al.[16]
An increase in the number of extrastimuli will increase the rate of VF inducibility, and using two extrastimuli improved the sensitivity of the test from 50% to 75% with a low positive predictive value (13%) but a good negative predictive value of PES in asymptomatic non-inducible individuals (99%).[57]
Makimoto et al.[62] reported that 2 out of 17 patients (12%) who had VF induced by 1-2 extrastimuli developed VF, but none of the 14 non-inducible patients by 3 extrastimuli or the 11 patients with no inducible arrhythmias developed VF during the 6 years of follow-up. In a pooled analysis of 1,312 patients with BrS but without CA by Sroubek et al,[28] the mean age at the electrophysiology study was 44.9±13.3 years. Of those patients, 1,034 (79%) were male, 429 (33%) presented with syncope, and 696 (53%) had a spontaneous type 1 ECG pattern. Ventricular arrhythmia was induced in 527 of 1,247 (42%) as follows: 22 with a single extrastimulus, 231 with double extrastimuli and 274 with triple extrastimuli. The individuals induced with single or double extrastimuli rather than more aggressive stimulation protocols were associated with an increased risk for CA. However, Takagi et al.[63] reported that none of the 30 patients who had VF induced by 1-2 extrastimuli developed spontaneous VF during the 3 years of follow-up. In the PRELUDE study, no differences were observed in the VF-free survival curves between the 63 patients without prior CA who had VF induced by 1-2 extrastimuli and the 245 patients who were either non-inducible or had VF induced with 3 extrastimuli.[26]
Patients with BrS might have a shorter ventricular effective refractory period (VERP) compared to non-BrS patients.[64] The short VERP < 200 ms during basic ventricular pacing at 600 ms correlated with an increased incidence of spontaneous VF in the PRELUDE study.[26] This outcome differs from the data of Makimoto et al.[62] which showed that the VF-free survival curves of 81 patients with inducible VF were identical whether VF was induced with a coupling interval < 200 ms.
Some antiarrhythmic agents are known to prevent VF recurrence in BrS. The study by Belhassen et al. showed that the EPS-guided selection of IA antiarrhythmic agents, which prevent VF induction, was beneficial.[65] However, such studies are not routinely performed.
Familial And Genetic Background
The inheritance of BrS occurs via an autosomal dominant mode of transmission, and 12 responsible genes have been reported thus far.[66] Either a decrease in the inward sodium or calcium current or an increase in one of the outward potassium currents has been shown to be associated with the BrS phenotype. Some mutations may develop a more severe phenotype,[67] but in many cases, there is complex interplay between mutations and polymorphisms.[68-72] No associations have been observed between a family history of sudden cardiac deaths or mutations in the SCN5A gene, and the risk of VF in larger studies. Furthermore, SCN5A mutations were found only in 30% or less of BrS patients. This low yield is a limiting factor of genetic studies in BrS.
As acute managements of VF storms, both oral quinidine and intravenous isoproterenol are effective.[8,73-75] Quinidine blocks transient outward current and rapid delayed rectifier currents and isoproterenol augments L-type calcium current.[76]
For long-term management, ICD is the main therapy (Figure 2). In the expert consensus statements,[8] ICD implantation is considered a class IIB indication for asymptomatic patients with inducible VF. Whereas in Japan, Class IIA or Class IIB indication is determined from the number of risk factors: a history of syncope, a family history of sudden death and inducibility of VF (Class IIA for the patients with two risks factors and Class IIB for those with one risk factors.[77] However, the current recommendation of ICD is still debated.
Figure 2: Indications of ICD for patients with Brugada syndrome (BrS)
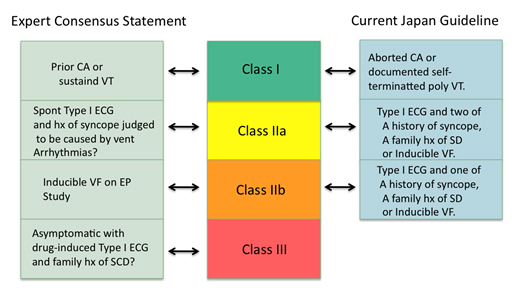
In the expert consensus statement (left) patients should have spontaneou type I ECG pattern of BrS when considering an implantation of ICD. In the Japan guideline (right), prior cardiac arrest or documentation of self-terminating polymorphic venticular tachycardia is requried for Class I indication. ICD may be recommended as Class IIA if patients have two of three risks factors, and as Class IIB if patients have one risk factor in addtion to spontaenous or drug-induced type I ECG pattern for BrS.
Quinidine is effective for prevention of VF in BrS,[65,73,74] but it may be intolerable in some patients. In a smaller number of patients, bepridil[78,79] or cilostasol[80] have been shown to be efficacious and promising. As new option, catheter ablation was shown to be effective in controlling VF storms by eliminating the VF triggering premature beats[81,82] or by modulating the arrhythmogenic substrate in the epicardial side.[83]
Current status of risk stratification of BrS and its managements were reviewed. For patients presenting with aborted sudden cardiac death or malignant syncope, ICD is recommended. However, risk stratification in asymptomatic BrS patients is still controversial and indication of ICD may vary from a country to another. Additional progress through the accumulation of pathophysiology data and genetic mutation data as well as clinical evidence are needed.






