Heart failure (HF) is one of the biggest epidemics of modern cardiovascular medicine. Cardiac resynchronization therapy (CRT) with biventricular (BiV) pacing has proven to have an integral role in the management of patients with reduced left ventricular (LV) function and left bundle branch blocks (LBBB). However, CRT with BiV pacing is not always feasible and even when it is, the percentage of non-responders remains high. Limitations in LV lead implantation due to anatomical or other constraints; non response to BiV pacing due to lead position or patient related factors and lack of benefit in patients with RBBB and patients with AV block and low normal LV function limit the use of BiV pacing. Permanent His Bundle pacing (HBP) is now a feasible alternative to BiV pacing for CRT therapy. This allows for recruitment of BBB disease and ventricular activation in a more physiological fashion. In this paper we review the physiology of HBP, available data on HBP for CRT and highlight how HBP can be a potential alternative in patients in whom BiV pacing did not provide clinical response or was unsuccessful.
Heart failure (HF) has become one of the biggest epidemics of modern cardiovascular medicine.HF affects approximately 5.7 million patients in the United States and it is predicted that by the year 2030 an additional 3 million Americans will have HF, representing an astounding 25% increase from 2010[1]. As a consequence, the management of HF accounts for one of the biggest burdens on health care expenditure. In 2007, the American Heart Association estimated that $33 billion was spent on heart failure alone and the annual direct cost of HF treatment in the Unites states is expected to increase from $24.7 billion in 2010 to $77.7 billion in 2030[2].
Conventional cardiac resynchronization therapy
Cardiac resynchronization therapy (CRT) has emerged as an integral part of the therapy for patients with HF with severely reduced ejection fraction and bundle branch block (representing inter-ventricular conduction delays). Conventional CRT achieves the synchronization of ventricular contraction through biventricular (BiV) pacing using an endocardial right ventricular (RV) lead and an epicardial left ventricular (LV) lead via the coronary sinus. The patients that benefit the most from BiV pacing are patients with severely reduced LV systolic function with a poor NYHA class and a wide left bundle branch block (LBBB) >= 150ms[3]. Multiple prospective randomized studies have shown that conventional CRT pacing yields improved quality of life, increased exercise capacity, reduced heart failure hospitalization and decreased all-cause mortality[4]-[9].
The indication for BiV pacing in patients with narrow QRS complexes has been limited to patients with a low LVEF undergoing implantation of a new or replacement pacemaker or implantable cardioverter defibrillator (ICD) with an anticipated requirement for a significant percentage (>40 %) of ventricular pacing[10].
Limitations of BiV pacing (Conventional CRT)
However, despite a significant benefit and evolving indications, there are still limitations to biventricular pacing. Firstly, up to a third of patients treated with conventional CRT do not derive a detectable clinical or echocardiographic benefit, and indeed, some worsen after resynchronization[4]; [6]; [11]. Secondly, procedural factors such as the location of the LV lead may also affect longer term outcome. An analysis from the MADIT-CRT trial by Singh et al[11] and other studies showed that a lead placed in the LV apical region is associated with a worse clinical outcomes. Anatomical limitations including lack of suitable coronary sinus venous branches and unavoidable phrenic nerve stimulation at ideal anatomic LV lead positions can limit the success of LV lead placement as well.
Conventional CRT has also shown a lack of benefit in patients with a normal QRS duration and among patients with RBBB[3]. It is also well known that long-term RV pacing can worsen LV function and HF. Recent trials have evaluated the utility of BiV pacing in the setting of heart block with contradicting results. The biventricular pacing for atrio-ventricular block and systolic dysfunction (BLOCK-HF) trial randomized patients with atrioventricular block, NYHA symptom class I to III heart failure, and left ventricular ejection fraction ≤50% to BiV versus RV pacing and demonstrated an improved quality of life and NYHA class with BiV pacing, mostly driven by change in left ventricular (LV) systolic volumes[12]. On the other hand, results from the BiV pacing for atrio-ventricular block to prevent cardiac de-synchronization (BioPace) trial that randomized patients who needed ventricular pacing at least two-third of the time, failed to show a significant clinical benefit of BiV pacing over RV pacing[13].
His Bundle Pacing (HBP) for CRT
Over the past few years, permanent HBP has become more feasible with the availability of better delivery systems. More recently, it has become a more attractive alternative to BiV pacing for CRT with the demonstration of resynchronizing ventricular activation by various groups[14]-[18]. The physiologic benefit of permanent His bundle pacing (HBP) is the ability to stimulate the ventricles through the intrinsic His-purkinje system, which results in synchronous and a more physiologic electrical and mechanical activation. HBP can also be used as a bail-out strategy in cases where coronary venous anatomy limits the ability to place an LV lead. Other advantages include the lack of potential complications from LV lead placement that include coronary sinus dissection, venous perforation, cardiac tamponade and the potential for proarrhythmia.
Available data on HBP for CRT
The available data on HBP as an alternative to BiV pacing for CRT is limited. Only few studies with small number of participants and limited experience have been reported. [Table 1] summarizes these data.
Table 1. Available data on HBP for CRT
|
Study Name
|
Design
|
Study population
|
Total attempted cases
|
Success rates (recruitment of BBB) using HBP
|
Outcomes
|
|
Barba-Pichardo et al 2013(16)
|
Prospective
|
HBP attempted in pts with failed LV lead placement
|
16
|
9
|
Improvement in NYHA class; Improvement in LVEF and LV dimensions
|
|
Lustgarten et al 2015(19)
|
Crossover
|
HBP and LV leads in all patients undergoing CRT
|
29
|
21
|
Significant improvements in ejection fraction, functional status, 6-minute walk distance with both HBP and BiV in 12 pts who completed the crossover.
|
|
Su et al 2016(20)
|
Prospective
|
HBP in pts with indication for CRT
|
N/A
|
29
|
Tested various pacing configurations and demonstrated lower pacing thresholds using a bipolar HB lead and RV lead configuration.
|
|
Ajijola et al 2015(21)
|
Prospective
|
HBP attempted in pts with failed LV lead placement
|
13
|
12
|
Improvement in LVEF and dimensions; Improvement in longitudinal strain.
|
|
Vijayaraman et al(22)
|
Prospective
|
Failed LV lead placement; HBP with LV leads; HBP alone in pts with indication for CRT
|
32
|
29
|
Improvement in NYHA functional class; Improvement in LVEF
|
BBB: bundle branch block; BiV: biventricular; HBP: His bundle pacing; LV: left ventricular;LVEF: left ventricular ejection fraction.
Barba-Pichardo et al. described their experience with HBP in failed CRT cases[16]. They attempted HBP in 16 patients with cardiomyopathy and failed CRT (Ischemic cardiomyopathy in 7, Idiopathic in 9). This represented 14% of the total number of patients derived for CRT during the inclusion period. Of those, temporary HBP corrected LBBB in 13 patients (81%) who were considered suitable candidates for Hisian cardiac resynchronization. Successful CRT by permanent HBP was then obtained in 9 patients, corresponding to 69% of the selected patients (Ischemic 4, Idiopathic 5). Mean QRSd decreased from 166±8 ms to 97±9 ms. HBP threshold at implant 3.09±0.44V @ 1ms. NYHA functional class improved from class III to class II and there was an improvement in left ventricular ejection fraction (LVEF) and LV dimensions.
Lustgarten et al compared HBP versus biventricular pacing in a crossover design among patients with indications for CRT defibrillator implants[19]. They enrolled 29 patients and were successful in demonstrating electrical resynchronization in 21 (72%) cases. All patients received both a coronary sinus LV lead and a HBP lead connected to the LV port via a Y-adapter. Patients were randomized in single patient-blinded fashion to either HBP or BiV pacing. After 6 months,patients were crossed over and followed for another 6 months. 12 patients completed the crossover analysis at 1 year. Both groups of patients demonstrated significant improvements in ejection fraction, functional status, and 6-minute walk distance. They concluded that HBP was noted to have an equivalent CRT response to conventional BiV pacing.
Su et al evaluated various pacing configurations in 16 patients undergoing successful CRT-D with HBP lead in the LV port and 13 dual chamber ICD implants (patients with permanent AF)with the HBP lead in atrial port[20]. They demonstrated that incorporation of HBP into a CRTD/ICD system is feasible, and capture thresholds and R-wave sensing can be optimized using an integrated bipolar configuration with the RV lead.
Ajijola et al evaluated thirteen patients with indication for CRT implant with failed coronary sinus LV lead placement[21]. The HBP lead was successfully placed in 12 of 13 patients (92%), with significant narrowing of the QRS duration to 120±23ms (p<0.0001). At 6-month follow up,they demonstrated an average increase in LVEF by 18.7%, and decrease in left ventricular end diastolic internal dimension (LVIDd) by 0.9cm. Echocardiographic global longitudinal strain improved from -9.1 to -10.5%.
Our experience with HBP for CRT
Our experience comprises of 29 patients with successful HBP for CRT (of 32 attempted cases)[22]. Fourteen of these were for failed coronary sinus LV leads, nine with primary HBP (AV nodal block), seven patients with HBP and LV leads and 2 patients with HBP leads due to conventional CRT non-response. QRSd improved from 165 +- 31 ms to 115 +- 19ms (p< 0.001).Over a mean follow-up of 17 +- 16 months, LVEF improved from a mean value of 30 +- 10 to 47 +- 11 percent (p< 0.05); and NYHA functional status improved by one class.
Possible mechanisms of Recruitment of LBBB with HBP
Various mechanisms for this recruitment of bundle branches in patients with bundle branch block/delay have been postulated. These include: (1) longitudinal dissociation in the HB with pacing distal to the site of delay/block and/or (2) differential source-sink relationships during pacing vs intrinsic impulse propagation and/or (3) virtual electrode polarization (VEP) effect[23].
The strongest postulated theory is that longitudinal dissociation exists within the HB and intrahisian disease is often responsible for BBB or delay. This concept was first elegantly studied by Narula et al back in 1977[24]. They postulated that delay within fibers in the HB could result in BBB or delay and demonstrated that pacing distal to the site of conduction delay could recruit fibers predestined to be the bundle branches and thereby narrow the QRS duration. Even if some of the disease is proximal within the intra-hisian region, it can be associated with a decrease in the number of conducting cells available to produce a sufficient upstream voltage gradient (source) to successfully depolarize through the diseased distal left bundle branch and increasing this number by pacing at a higher output might be sufficient to improve conduction[25].
Case 1:A 65-year-old man with nonischemic cardiomyopathy, LVEF of 20-24%, NYHA classIII functional status and chronic atrial fibrillation was referred for ICD implantation for primary prevention of sudden cardiac death. His medical therapy included carvedilol 25 mg twice daily,digoxin 0.25 mg daily, lisinopril 40 mg daily and spironolactone 25 mg daily. Holter monitoring showed average HR of 70 bpm with periods of rapid ventricular rate and nocturnal bradycardia.He underwent dual chamber ICD with HBP lead connected to the atrial port in anticipation of need for ventricular pacing. The device was programmed to DDIR mode at 50 bpm. During 3-month follow-up he was noted to have 60% HBP (atrial) and 99.5% RV sensed events. Despite adequate AV nodal blockade, he presented several months later with episodes of near syncope and two ICD shocks while carrying groceries. ICD interrogation revealed multiple episodes of FVT due to AF with RVR but therapy withheld due to recognition as supraventricular arrhythmias and the 2 episodes required ICD shocks due to organization into atrial flutter with 1:1 conduction at 230 bpm. Subsequently AV node ablation was performed allowing >99% HBP with paced QRS duration of 130 ms with minimal fusion ([figure 1] and [figure 2]). At 6 months his LV function improved to 38% and NYHA functional class to II. This case illustrates the value of HBP in patients with normal QRS in whom high percentage of ventricular pacing is anticipated. By preserving native His-Purkinje conduction through HBP, the adverse effects of right ventricular pacing can be prevented.
Figure 1. A. Twelve lead ECG of a patient with nonischemic cardiomyopathy and chronic atrial fibrillation at baseline is shown. B. Following AV node ablation, nonselective His bundle pacing with minimal RV fusion and paced QRS duration of 130 ms is shown.
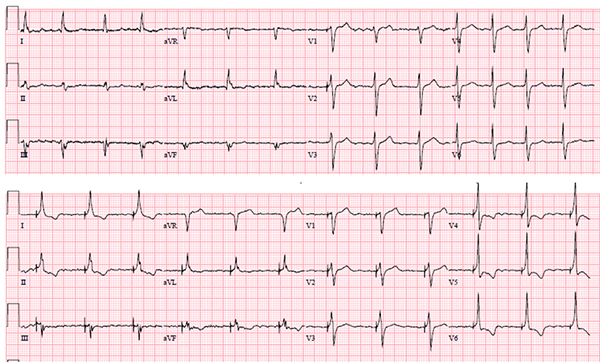
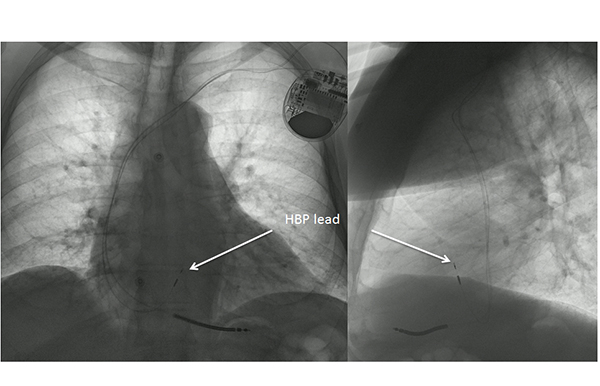
Figure 2. PA and lateral chest X-rays of patient in figure 1 is shown.
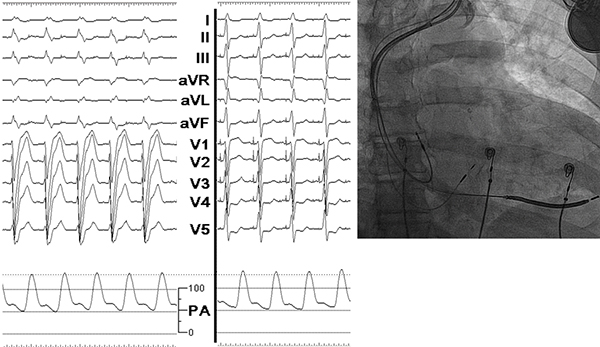
Case 2:A 70-year-old man with nonischemic cardiomyopathy and severely reduced LV function, LBBB and class III CHF on optimal medical therapy was referred for biventricular ICD. LV lead placement was unsuccessful due to lack of suitable lateral vein branches and diaphragmatic stimulation in the posterolateral vein branch with high LV capture thresholds. At this point, His bundle pacing was successfully performed and the lead connected to the LV port of biventricular ICD. During HBP, QRS duration significantly shortened from 210 ms at baseline to 130 ms ([figure 3]). LV ejection fraction improved from 25% to 40% and NYHA functional status changed from class III to II during follow-up. This case highlights the utility of permanent HBP as an option for cardiac resynchronization therapy in patients in whom LV lead placement is unsuccessful.
Figure 3. A. Twelve lead ECG of a patient with nonischemic cardiomyopathy and LBBB with QRS duration of 210 ms is shown. B. During selective HBP, QRS duration decreases to 130 ms with improvement in systolic BP by 6-10 mm of Hg. C. Fluoroscopic image of CRT-D with HBP lead is shown.
Conclusions and Future Directions
Cardiac resynchronization therapy with biventricular pacing has definitely made a significant impact in cardiovascular morbidity and mortality in patients with LV systolic dysfunction and heart failure. However, challenges remain due to high non-responder rates. While patients with LBBB, non-ischemic dilated cardiomyopathy, no or limited scar at MRI evaluation and female gender have high probability to be responders, permanent HBP may provide a real alternative to biventricular pacing in patients with low response rate. In our opinion HBP should be attempted in patients who fail LV lead placement prior to considering alternative options such as surgical epicardial or endocardial LV lead placement. HBP may be the more physiological primary option in patients with normal His-Purkinje conduction but requiring ventricular pacing in the setting of LV dysfunction and in patients undergoing AV node ablation. HBP may also be considered in patients with cardiomyopathy and underlying RBBB with or without prolonged PR intervals as an option for cardiac resynchronization therapy. [26]
Several questions remain regarding HBP as a viable option for cardiac resynchronization therapy. How effective is HBP compared to biventricular pacing in patients with LBBB? While preliminary data from a small, randomized, cross-over study suggest equivalent response, we do not have large, long-term outcome data. What percentage of patients with LBBB can be corrected by HBP? How much correction of LBBB is necessary to achieve electrical and mechanical resynchronization and clinical response? Can HBP correct BBB in similar fashion in both ischemic vs non-ischemic cardiomyopathy patients? Will HBP maintain electrical resynchronization during long-term follow-up? Can we improve on capture thresholds required to correct BBB? In order to answer all these questions, additional clinical research and investment to improve clinical tools to achieve optimal HBP is necessary. Last but not the least,large, multicenter, randomized study comparing HBP to biventricular pacing needs to be performed to evaluate the clinical efficacy of HBP and to define its role in achieving cardiac resynchronization therapy.






