Adjunctive Therapies for Catheter Ablation of Non-Paroxysmal Atrial Fibrillation
Joshua A. Cohen1, Moussa Mansour2
1Massachusetts General Hospital Department of Medicine.2Massachusetts General Hospital Corrigan Minehan Heart Center.
The success rate of pulmonary vein antral isolation (PVAI) for paroxysmal atrial fibrillation (AF) has not been realized for persistent or long-standing AF, collectively termed nonparoxysmal AF. Many investigators have described adjunctive ablation strategies to improve outcomes for catheter ablation in patients with non-paroxysmal AF. In this focused review we aim to describe these therapies and current evidence pertaining to their utilization. At present, left atrial posterior wall (LAPW) ablation, non-pulmonary vein (non-PV) trigger ablation and rotor ablation appear to improve outcomes for patients with non-paroxysmal AF when performed in conjunction with PVAI. Randomized controlled trials are necessary to further elucidate such claims.
Correspondence to: Corresponding Author
Moussa Mansour MD
55 Fruit Street
Boston, MA 02114
Atrial Fibrillation (AF) is the most common sustained arrhythmia encountered in clinical practice, and is associated with significant morbidity and mortality. In 2010 it was estimated that AF afflicted 5.2 million patients, with 1.2 incident cases diagnosed yearly. These numbers are expected to more than double by the year 2030 to 12.1 million and 2.6 million respectively [1] .
Clinically, AF is classified by the duration of time in the arrhythmia and can be categorized as paroxysmal (self-terminating usually within 48 hours but must last <7 days including spontaneous or electrical cardioversion), persistent (episodes lasting >7 days including pharmacologic or electrical cardioversion after that time), and long standing (continuous AF lasting >1 year at which time a rhythm-control strategy is adopted). These distinctions have been adapted in clinical trials and other forms of research as such classifications have prognostic and therapeutic implications when considering catheter ablation [2] .
Catheter Ablation of Atrial Fibrillation
Although approximately 20-40% of patients with AF are asymptomatic, the vast majority of patients present with symptoms [3]. In general, the approach to asymptomatic patients usually involves a rate-control strategy, whereas symptomatic patients tend to prefer rhythm-control. Radiofrequency (RF) catheter ablation is a successful therapy for eliminating AF and reducing the symptomatic burden in patients with this arrhythmia. Pulmonary Vein Antral Isolation (PVAI) has become the primary ablation strategy for catheter ablation of AF [4]. Success rates vary based on patient characteristics, comorbidities and operator experience, but in general those patients with paroxysmal AF undergoing pulmonary vein isolation have success rates with freedom from atrial arrhythmias approaching 80-85% [5],[6]. Unfortunately, these outcomes have not been realized when PVAI alone is carried out in patients with non-paroxysmal AF where freedom from atrial arrhythmias is closer to 50-60% [7].
Current indications for catheter ablation as proposed by three societal guidelines are outlined in [table 1] [2],[4],[8].These indications continue to evolve over time as catheter ablation has been shown to be more effective in maintaining sinus rhythm as compared to antiarrhythmic drugs (AADs) and the rate of adverse pre, peri and post-procedural events, though not trivial, is comparable to that associated with AADs [2],[9]. Given the disparity in outcomes surrounding paroxysmal and non-paroxysmal AF after PVAI, multiple adjunctive ablation strategies have been described with varying rates of success; the subject of which is discussed below.
Table 1. Indications for catheter ablation for symptomatic non-paroxysmal AF as defined by different societal guidelines.
|
Guideline
|
Indication
|
AF Type
|
Recommendation
Class
|
Level of Evidence
|
|
HRS 2012
|
Failure or Refractory to at least 1 Class I/III AAD
|
Persistent
|
IIa
|
B
|
|
Longstanding
|
IIb
|
B
|
|
First line therapy
|
Persistent
|
IIb
|
C
|
|
Longstanding
|
IIb
|
C
|
|
ACC/AHA 2014
|
Failure or Refractory to at least 1 Class I/III AAD
|
Persistent
|
IIa
|
A
|
|
Longstanding
|
IIb
|
B
|
|
First line therapy
|
Persistent
|
IIb
|
C
|
|
ESC 2016
|
Failure or Refractory to at least 1 Class I/III AAD
|
Persistent/Longstanding
|
IIa
|
C
|
Adjunctive Modalities for Non-Paroxysmal Atrial Fibrillation
Adjunctive therapies have been developed and studied in an attempt to increase success rates after PVAI in patients with non-paroxysmal AF. These methods, described below, include left atrial posterior wall (LAPW) ablation, non-pulmonary vein trigger ablation of the superior vena cava (SVC), inferior vena cava (IVC), left atrial appendage (LAA), coronary sinus (CS), and vein of marshall (VOM), complex fractionated atrial electrogram (CFAE) ablation, and rotor ablation. It is important to note that these therapies occur in conjunction with PVAI or on repeat catheter ablation.
Left Atrial Posterior Wall Ablation/Isolation
The LAPW has been documented as a potential contributor to the initiation and maintenance of AF [10]. In addition, the structure shares an embryologic cell lineage with the pulmonary veins and thus logically may play a role in the initiation of atrial arrhythmias.
Figure 1. LAPW ablation
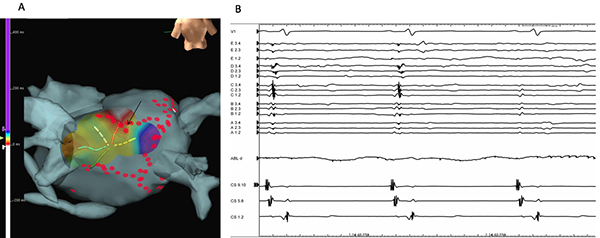
Isolation of the posterior left atrial wall. (A) Electroanatomical map of the posterior wall of the left atrium during sinus rhythm following an initial set of ablations. A multispline catheter positioned in the posterior wall showing the site of breakthrough (arrow). (B) Recording from the multispline catheter during ablation showing isolation of the posterior wall during the third beat.
Catheter ablation of the LAPW is accomplished via linear lesions connecting circumferential PV ablation sites, or spot ablations to the entire structure ([Figure 2]). Ablation and proven isolation of the LAPW in conjunction with extended PVAI resulted in superior outcomes (freedom from any atrial arrhythmia) throughout follow up at 1, 2, and 3 years and more than tripled the median time to recurrence in patients with persistent AF [12]. It has also been shown that isolation of the LAPW as compared to PVAI + Linear lesions (Roof and Anterior LA) was associated with a significant (>50%) reduction in the rate of recurrence over the course of 12 month follow up [11]. LAPW ablation/isolation can be accomplished without compromising the pump function of the LA, with few complications and no significant difference in fluoroscopy and procedural times [11],[12].
Figure 2. Superior Vena Cava Isolation
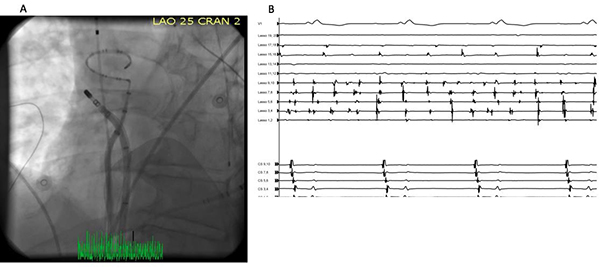
(A) Circular mapping catheter in the SVC and ablation catheter at the site of ablation at the ostium of the SVC. (B) Superior Vena Cava Isolation. Intracardiac recording showing isolation of the SVC which continues to be in atrial fibrillation while the atrium was in sinus as demonstrated by the recording of the coronary sinus catheter
The SVC shares an embryologic cell lineage with that of the sinus node and thus can represent an arrhythmogenic focus in patients with AF [13]. It also represents the greatest non- PV trigger with an incidence reported anywhere from 6-12% [14]. Although it represents the dominant site of non-PV triggers, early data supporting systematic SVC isolation has not been reproduced for patients with non-paroxysmal AF [15]. The potential benefits of this adjunctive therapy require further examination in larger randomized trials. Phrenic nerve paralysis and injury also poses a limitation on this procedure and precludes up to 15-18% of patients from successful ablation of the SVC [14].
The IVC has been documented in case-reports as a focal source of ectopic beats resulting in atrial fibrillation. While this trigger is very rare, it does exist and could account for a small proportion of AF recurrences following PVAI. Routine focal ablation of the IVC is not recommended unless triggers are identified [17],[18] .
Left Atrial Appendage (LAA)
The LAA is a known trigger of AF and has been reported in as many as 27% of patients undergoing repeat catheter ablation. In the same patient population, the LAA was found to be the only source of arrhythmia in 8.7%. With complete isolation of the LAA, patients with nonparoxysmal atrial fibrillation had a significant reduction in rate of AF recurrence, while those with focal LAA ablation or no ablation did not [19].
Figure 3. Epicardial Left Atrial Appendage Ligation
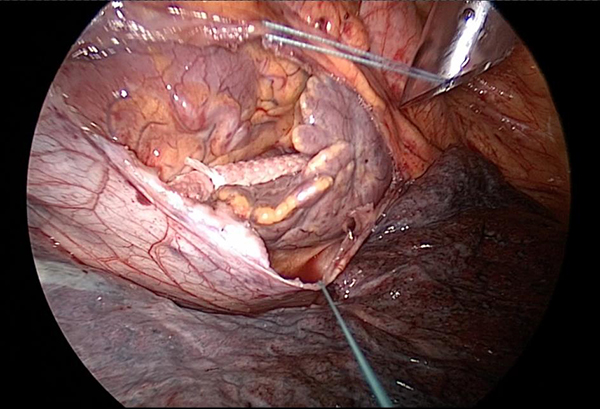
Intraoperative epicardial left atrial appendage ligation using AtriClip® [AtriCure, West Chester, OH]. Credit: Roger G. Carrillo MD MBA, University of Miami Miller School of Medicine
While catheter ablation leading to isolation of LAA has been shown to be effective during repeat ablation, endocardial isolation can be difficult to achieve due to significant anatomic variation in LAA anatomy, and inability to maintain catheter stability. As such epicardial methods to exclude and/or isolate the LAA have been studied. Devices such as the LARIAT© device [SentreHEART, Redwood, CA] and AtriClip® [AtriCure, West Chester, OH ([figure 4]) have been shown to not only mechanically exclude the LAA but also provide complete electrical isolation. Recently, epicardial LAA exclusion and isolation with the LARIAT© device was found to provide a significant reduction in AF burden at both 3 and 12 month follow up for patients with non-paroxysmal AF [20]. In addition, the strongest predictor of response was known LAA triggers in which the reduction of AF burden was even more pronounced. Complete electrical isolation of the LAA either by catheter ablation or thoracoscopic epicardial exclusion as an adjunct to current ablative therapies seems reasonable, especially in patients with known LAA triggers. A randomized clinical trial (AMAZE AF) is currently being conducted and aims to demonstrate the role of adjunctive exclusion of the LAA.
The CS has been implicated as a source of triggers contributing to the initiation and maintenance of AF after catheter ablation. In small samples and preliminary data both epicardial and endocardial catheter ablation (complete isolation) in comparison to focal ablation of the coronary sinus resulted in intraprocedural termination of AF in 30% of patients with nonparoxysmal AF [21], [22]. While data regarding CS ablation is less robust than other trigger ablation targets, experts in the field support both epicardial and endocardial ablation of the CS in conjunction with PVAI and other non-PV trigger ablations if spontaneously observed or induced [6].
The VOM is the embryologic remnant of the left common and anterior cardinal veins, and has been associated with intrinsic autonomic activity and trigger activity. The VOM was also found to play a role in PV reconnection and recurrence of AF after PVAI [23]. Ethanol infusion into the VOM was effective in disconnecting some of the previously reconnected PVs. In addition, the use of the VOM as a vascular route to the intrinsic cardiac nerves (ICNs) in an effort to modulate autonomic input to the AV node has been investigated [23], [24]. The above mentioned studies are small and larger trials are needed to confirm the role of VOM ablation as an adjunctive therapy for the treatment of AF.
Rotor ablation is founded on the localized source theory in which spiral waves (rotors) and/or focal sources of re-entrant electrical activity can become disorganized and sustain AF. This is in contrast to the multiple wavelet theory in which multiple wandering waves of electrical activity lead to AF. Such rotors and focal sources were found in 97% of cases presenting for ablation in the CONFIRM trial in which focal impulse and rotor modulation (FIRM) was found to successfully slow or terminate AF in 86% of patients (paroxysmal and non-paroxysmal) prior to conventional ablation [25]. In addition, there was a significant reduction in early and late recurrence (median follow up 271 days and 890 day post procedure) in patients undergoing FIRM and conventional ablation as compared to those undergoing only conventional ablation.
There was no difference in procedural time or complications [26]. Patient specific mapping and FIRM ablation is a promising adjunctive therapy and remains to be further validated in randomized controlled trials.
Complex Fractionated Atrial Electrograms (CFAE)
CFAEs are fractionated electrograms that are thought to result from the collision of wavelets and electrical signals traveling in different directions as atrial remodeling occurs. These fractionated electrograms are thought to maintain AF and can be targeted during catheter ablation along with conventional PVAI in an attempt to reduce AF burden. The literature regarding CFAE ablation is conflicting as one meta-analysis reports a significant increase in freedom from all atrial tachyarrhythmias (ATs) in patients with non-paroxysmal but not paroxysmal AF with reported follow up between 10-19 months post procedure depending on the study. Upon repeat analysis in which non-randomized clinical trials were taken out, this effect was no longer statistically significant [27].
In a larger randomized clinical trial with 589 patients, no significant difference in freedom from AF was observed at rigorous 18 month total follow up when comparing PVAI with PVAI + CFAE and PVAI + Linear ablations for patients with non-paroxysmal AF. CFAE ablation also increases procedural time as well as time under fluoroscopy [7]. As a result, it is important to recognize that improved outcomes with CFAE ablation in patients with nonparoxysmal AF have not been uniformly reported and that the rationale of CFAE ablation is not universally accepted.
Isolation of the pulmonary veins is a successful therapy for those patients with paroxysmal but not persistent or long standing (non-paroxysmal) AF. As such, adjunctive ablation strategies to combat recurrence rates in non-paroxysmal AF are the subject of significant research. Although many adjunctive strategies described above lack data from large randomized controlled trials, current evidence seems to support the use of LAPW ablation, rotor ablation, and non-PV trigger ablation of the LAA (from an endocardial or epicardial approach) and to a lesser degree the CS, SVC, IVC and VOM. These therapies are reasonable adjuncts to PVAI in patients with nonparoxysmal atrial fibrillation aimed at long-term freedom from AF recurrence while balancing the risks associated with more technically complex and lengthy procedures. It is important to remember that these procedures are highly dependent on experienced operators in specialized centers.






