Stroke Prevention for Patients with Atrial Fibrillation: Beyond the Guidelines
McIntyre WF1,2, Jeff Healey1,2
1McMaster University, Hamilton, Ontario, Canada.2Population Health Research Institute, Hamilton, Ontario, Canada.
Atrial fibrillation (AF) is the most common serious heart rhythm disorder, with a lifetime incidence of 1 in 4 for patients >40 years of age[1]. AF is a major cause of death and disability, as it is associated with a 4-5 fold increase in the risk of ischemic stroke[2]. In patients with AF, oral anticoagulation (OAC) therapy can reduce the risk of stroke by about two-thirds and the risk of all-cause mortality by approximately one-quarter, but is associated with an increased risk of bleeding[3], [4]. Atrial fibrillation (AF) is the most common serious heart rhythm disorder and is associated with an increased risk of ischemic stroke. This risk can be moderated with oral anticoagulation therapy, but the decision to do so must be balanced against the risks of bleeding. Herein, we discuss three emerging areas where more high-quality evidence is required to guide risk stratification: 1) the relationships between the pattern and burden of AF and stroke 2) the risk conferred by short episodes of device-detected “sub-clinical” atrial fibrillation (SCAF) and 3) the significance of AF that occurs transiently with stress (AFOTS), as is often detected during medical illness or after surgery. Risk stratification is important to identify patients with AF who can benefit from OAC therapy. There are, however, several common clinical scenarios where guidelines do not yet provide direction for stroke prevention; or do so based on limited high-quality evidence.
Key Words : Atrial fibrillation, subclinical, stress, stroke.
Correspondence to: Dr Jeff S Healey Email: Jeff.Healey@phri.ca David Braley Cardiovascular and Stroke Research Institute Population Health Research Institute McMaster University Hamilton, ON, L8L 2X2, Canada Tel: 905-527-0271, ext 40312 Fax: 905-297-3786 Mobile: 905-330-6760
Atrial fibrillation (AF) is the most common serious heart rhythm disorder, with a lifetime incidence of 1 in 4 for patients >40 years of age[1]. AF is a major cause of death and disability, as it is associated with a 4-5 fold increase in the risk of ischemic stroke[2]. In patients with AF, oral anticoagulation (OAC) therapy can reduce the risk of stroke by about two-thirds and the risk of all-cause mortality by approximately one-quarter, but is associated with an increased risk of bleeding[3], [4]. Risk stratification is important to identify patients with AF who can benefit from OAC therapy. There are, however, several common clinical scenarios where guidelines do not yet provide direction for stroke prevention; or do so based on limited high-quality evidence.
AF Burden and the Risk of Stroke
Current AF guidelines recommend risk stratification, to estimate the risks of stroke and bleeding and offering OAC to patients who have a favorable risk-benefit profile[5]-[7]. The risk of stroke and bleeding are estimated based on the patient’s age and comorbidities; typically using the CHA2DS2-VASc score for stroke[8]-[12], and the HAS-BLED score for major bleeding[13]-[15]. Current guidelines do not consider the pattern of AF (paroxysmal, persistent and permanent), nor the burden of time that a patient spends in AF when estimating the risk of stroke and whether or not to offer patients OAC [5]-[7].
Emerging evidence suggests that the pattern, frequency and duration of episodes of AF (also known as arrhythmia burden) may influence stroke risk. A large analysis of more than 6500 aspirin-treated patients from the ACTIVE-A and AVERROES trials suggested a clear gradient of increasing risk of stroke/systemic embolism (SE) from paroxysmal to persistent to permanent AF. In this study, which included rigorously adjudicated outcomes, annualized ischemic rates of stroke/SE rates were 2.1, 3.0, and 4.2% respectively, with an adjusted hazard ratio (HR) of 1.83 (95% CI 1.43-2.35; P < 0.001) for permanent vs. paroxysmal AF and 1.44 (95% CI 1.05-1.98 P = 0.02) for persistent vs. paroxysmal AF[16]. The concept of differing risk according to AF pattern is further supported by a report from the Fushimi AF registry that demonstrated that sustained (permanent or persistent) AF was independently associated with a higher incidence of stroke/SE as compared to paroxysmal AF (non-OAC users: HR 2.2, 95% CI 1.3–3.7; P<0.01 and OAC users: HR 1.7, 95% CI 1.1-2.9; P=0.03)[17]. Owing to observations of increasing risk of stroke/SE with increasing AF burden, some authors have proposed that embolic risk be estimated on the basis of refined algorithms that consider both the burden of AF and patient characteristics[18], [19]. Such schemata represent an emerging area of research, but require further prospective validation before they can be used clinically.
In the meantime, it should be stressed that the presence of paroxysmal AF does NOT obviate the need for OAC in patients with additional stroke risk factors. In the pooled ACTIVE-A and AVERROES analysis, the 5 year rate of stroke among patients with paroxysmal AF was approximately 10% - this is well above our current threshold to consider treatment with OAC[16]. Another group of patients of interest are young patients without additional stroke risk factors who have persistent or permanent AF, which may place them at increased risk of stroke and other adverse neurological outcomes[20], [21]. Approximately 10-15% of patients with AF may not have any additional stroke risk factors, but still have some risk of stroke[22]. Such patients are currently being randomized to receive aspirin or 15 mg of rivaroxaban once daily in the BRAIN-AF trial (NCT02387229) to determine if stroke (clinical and covert) as well as cognitive decline can be prevented through the use of OAC.
Subclinical Atrial Fibrillation (SCAF)
Given the current widespread use of continuous long-term cardiac monitoring, it is now recognized that many patients have evidence of short-lasting AF, without recognizable symptoms. This phenomenon has been termed subclinical atrial fibrillation (SCAF), and was first described in studies of pacemaker patients, such as ASSERT, TRENDS and MOST, where it was initially given the more descriptive term “atrial high-rate episodes (AHRE)”[23]-[25]. SCAF does not simply mean asymptomatic AF, which could encompass AF that is permanent. Arrhythmias referred to as SCAF must also be short-lasting, be detected only with long-term continuous monitoring, and not captured on routine surface ECG[23], [26]-[29]. The concept is that short-lasting AF detected after many weeks of monitoring represents a low overall burden of AF, which appears to convey an increased risk of stroke/SE, albeit lower than would be expected in otherwise similar patients with clinical AF[23], [25].
The management of patients with SCAF is much less clear. High quality evidence for treatment benefit is lacking. The Relationship Between Daily Atrial Tachyarrhythmia Burden From Implantable Device Diagnostics and Stroke Risk (TRENDS) study was among the first to suggest that SCAF was associated with an increased thromboembolic risk, although these were prospective observational study included some patients with clinical AF[24], [25]. The increased stroke risk associated with SCAF was confirmed in The Asymptomatic Atrial Fibrillation and Stroke Evaluation in Pacemaker Patients and the Atrial Fibrillation Reduction Atrial Pacing Trial (ASSERT), which reported exclusively on patients without a known history of clinical AF[23]. In this study, SCAF was associated with an increased risk of new clinical AF (HR 5.56, 95%CI 3.78-8.17; P<0.001) and of ischemic stroke/SE (HR 2.49, 95%CI 1.28-4.85; P=0.007). However, among patients average CHADS2 score of 2, the annual risk of stroke was only 1.3%; far lower than would be expected in similar patients with clinical AF [Table 1][9].
Where it is generally accepted that SCAF is associated with an increased risk of stroke, the decision to anti-coagulate patients with SCAF is not straightforward. Despite the assertion of some experts that patients with SCAF and additional risk factors for stroke are high risk and merit OAC, clinical practice varies[23], [30]-[36].
Table 1. Comparison of annualized event rates in patients with clinical AF, according to Gage et al., and SCAF, according to Healey et al.[9], [23]
| |
Rate of Ischemic Stroke/
Systemic Embolism (%/year)
|
|
CHADS2 Score
|
Clinical AF
|
SCAF
|
|
1
|
1.9
|
0.56
|
|
2
|
2.8
|
1.29
|
|
>2
|
4.0-12.5
|
3.78
|
There are several reasons why patients with SCAF might not derive the same risk-benefit from OAC as similar patients with clinical AF. First, the reported thromboembolic rates in patients with SCAF are low compared with patients with clinical AF who have otherwise similar risk profiles (Table 1)[9], [23], [25]. Second, the Randomized trial of atrial arrhythmia monitoring to guide anticoagulation in patients with implanted defibrillator and cardiac resynchronization devices (IMPACT) was stopped for futility[37]. This study was designed to test the hypothesis that initiation and withdrawal of OAC guided by continuous ambulatory monitoring of the atrial electrogram would improve clinical outcomes by reducing the combined rate of stroke, systemic embolism, and major bleeding as compared with conventional clinical management[33]. Third, it is important to recognize that observational data have failed to show a temporal relationship between SCAF and stroke in the majority of patients[25], [29], [38], [39]. For example, in an analysis of the ASSERT trial, only 8% of patients had SCAF detected in the 30 days prior to their stroke/SE. Furthermore, 16% of patients with SCAF and ischemic stroke/SE did not have any SCAF detected prior to their stroke/SE[29]. Similarly, in the TRENDS study, 73% of patients who experienced a stroke/SE had zero AF burden in the 30 days prior to their event[40]. These findings, in particular, raise the possibility that stroke/SE in patients with AF may occur secondary to pathophysiologic mechanisms other than the classically hypothesized construct of a minimum of 24 to 48 hours AF leading to atrial stasis, clot formation and subsequent SE[41]. Fourth, the trials that established the benefit of OAC for stroke prevention in AF were comprised predominantly of patients with sustained AF or high burdens of paroxysmal AF [3], [4], and data suggest that patients with paroxysmal AF may be at lower (albeit still significant) risk of stroke, as discussed in the previous section. The burden of SCAF has also been identified as a possible risk factor for stroke. In the TRENDS study, as compared to patients without AF, patients with <5.5 hours of SCAF were not at increased risk of stroke/TIA/SE (HR 0.98, 95% CI 0.34-2.82; p =0.97, but there was a trend towards increased risk in patients with >5.5 hours of SCAF (HR 2.2, 95% CI 0.96-5.05; p=0.06)[25]. In an analysis of data from the ASSERT study, the risk of ischemic stroke/SE was found to be increased with episodes of SCAF as short as 6 minutes in duration (RR 1.77, 95% CI 1.01-3.10; p=0.047) and the relative risk reached as high as 4.96 (95% CI 2.39-10.3; p<0.01) with episodes >24 hours in duration[23]. It is conceivable that on a spectrum of risk, SCAF could fall lower than paroxysmal AF and below a threshold at which the benefits of stroke prevention from OAC are outweighed by the risks of bleeding. Even assuming that OAC confers the same relative risk reduction for stroke in patients with SCAF as compared to those clinical AF, the lower absolute risk of stroke may have an important impact on the risk-benefit ratio and cost-effectiveness of OAC. As a result, clinical practice remains divided regarding the treatment of SCAF. At least two randomized clinical trials are underway to address the use of OAC for patients with SCAF, including Apixaban for the Reduction of Thrombo-Embolism in Patients With Device-Detected Sub-Clinical Atrial Fibrillation (ARTESiA, NCT01938248) and Non-vitamin K Antagonist Oral Anticoagulants in Patients With Atrial High Rate Episodes (NOAH, NCT02618577).
Atrial Fibrillation Occurring Transiently with Stress (AFOTS)
Uncertainly surrounds the approach to stroke prevention for patients who experience AF occurring transiently with stress (AFOTS). In patients without a history of the arrhythmia, AF is often observed for the first time in the setting of an acute stressor, such as medical illness or surgery, typically while the patient is undergoing continuous surface ECG monitoring. Physicians frequently do not prescribe OAC therapy when it is judged that AF may have occurred due to a potentially reversible precipitant[6], [42]-[45].
It is not known whether a presentation of AFOTS occurs secondary to a reversible cause and is ultimately benign, or is simply the first documentation of paroxysmal AF and is therefore associated with an increased risk of stroke[46]. Major guidelines do not currently make recommendations for OAC or for post-discharge screening for recurrent AF in patients who experience AFOTS[5]-[7]. Moreover, more recent guidelines have acknowledged that we are lacking in data to direct the long-term management of patients with AFOTS[6].
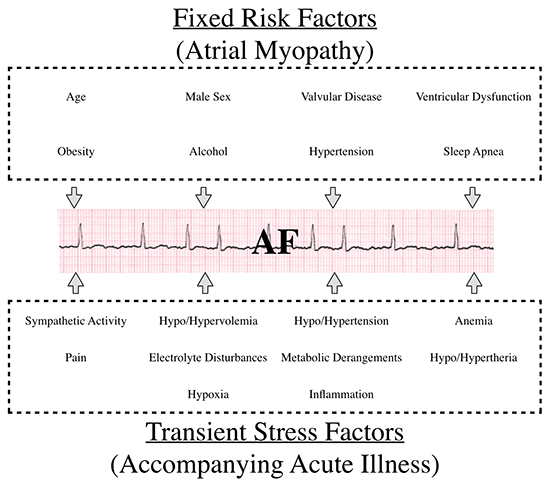
It can be conceptualized that during an episode of AFOTS, there is interplay between fixed and transient arrhythmogenic factors [Figure 1][44], [47]-[57]. Traditional risk factors for AF are present in many acutely ill patients, and may have led to the development of AF-promoting electro-anatomical alterations in atrial tissue[48], [50]. This substrate has been termed atrial myopathy[57], [58]. In the setting of acute stress, such as accompanies acute medical illness or surgery, multiple additional and potentially provoking acute factors come into play[51]-[56]. What remains unknown is to what degree an episode of AFOTS represents a predisposition for recurrence of AF (and therefore a risk of stroke, heart failure and death).
Figure 1. Pathophysiological Factors implicated in Atrial Fibrillation Occurring Transiently with Stress (AFOTS).
AFOTS occurs frequently (incidence 4-44%) in the setting of acute illness[56], [59]-[83]. AFOTS has been shown to occur with many medical illnesses, including local and systemic infections, myocardial infarction, hyperthyroidism, lung disease and venous thromboembolic disease. In patients admitted to general medical wards and intensive care units, AFOTS is common across a wide variety of conditions. The incidence of AFOTS has been reported to range from 5-44% in sepsis[60], [66]-[74], 4-18% in acute pulmonary syndromes (e.g. pneumonia, exacerbation of chronic obstructive pulmonary disease and pulmonary embolism)[75]-[80] and 10-25% in hyperthyroidism[81], [82]. AFOTS is also common in post-surgical patients. Here, the incidence of AFOTS is approximately 1% for all surgery, 8-10% in vascular surgery, 9-14% in colorectal surgery, 10-35% in thoracic surgery and 18-50% in cardiac surgery[84]-[96]. Across the literature, the incidence of AFOTS tends to be higher in prospective studies. This likely originates from the fact that detection of AFOTS usually requires continuous monitoring and active surveillance facilitates recognition of this intermittent arrhythmia. The incidence also tends to be higher in critically ill patients. This could be a reflection of an increased propensity for AFOTS with more severe illness or simply a reflection of more intensive rhythm monitoring.
Some data exist on the recurrence of AF following AFOTS, but these are limited to retrospective study designs and rely on opportunistic diagnosis of AF through non-systematic follow-up methods. A recent publication from the Framingham Heart Study investigated long-term AF outcomes after diagnosis during a secondary precipitant (i.e. AFOTS). AFOTS precipitants included surgery, acute myocardial infarction, acute infection, acute alcohol consumption, thyrotoxicosis, acute pericardial disease and acute pulmonary syndromes. In this study, patients with AFOTS had an AF recurrence rate of 42% at 5 years. This was similar to the 59% recurrence rate of AF for patients in the cohort whose first presentation of AF was not in the setting of AFOTS (i.e. incident paroxysmal AF). Stroke risk (HR 1.13, 95%CI; 0.82-1.57; P=0.45) and mortality (HR 1.00, 95%CI 0.87-1.1.5; P=0.95) did not differ between those with AFOTS and those with incident paroxysmal AF[97]. A retrospective study using a United States Medicare 5% sample investigated long-term outcomes following development of AFOTS during sepsis. Recurrence of AF after discharge was ascertained through health care claims using International Classification of Diseases (ICD-9) codes. In this study, incidence of AF recurrence at one-year following sepsis hospitalizations was 44% in AFOTS patients. This was significantly higher than patients who did not have AFOTS during sepsis (7.7%, p<0.001). Compared with patients with no AF during sepsis, those with AFOTS during sepsis had greater 5-year risks of ischemic stroke (5.3% vs. 4.7%, HR 1.22, 95%CI 1.10-1.36), and death (74.8% vs. 72.1%, HR 1.04; 95%CI 1.01-1.07)[98]. Gialdini et al. reported on a 1,729,360-person retrospective cohort study of surgical patients who experienced AFOTS. Recurrence of AF after discharge was ascertained through health care claims using ICD-9 codes. Even though IC-9D coding may lack sensitivity for AF detection, the investigators found the one-year rate of recurrent AF after an episode of AFOTS associated with non-cardiac surgery to be 37%. This was higher than the rate of new AF diagnosis in patients without AFOTS (1.5%). At 1 year after hospitalization for non-cardiac surgery, cumulative rates of stroke were 1.47% in those with perioperative AF and 0.36% in those without AF (HR for all stroke = 2.0, 95%CI 1.7-2.3; HR for embolic stroke = 4.9, 95%CI 3.5-6.7)[84].
Where the three above studies provide a strong signal that AFOTS is associated with a risk of recurrent AF and stroke, they have important limitations that greatly impair their sensitivity for ascertaining recurrent AF. Thus, they have likely underestimated the rate of AF recurrence after AFOTS. First, none of these studies systematically investigated AF recurrence. Not all participants in these studies would have been subject to the same post-AFOTS monitoring strategy and it is likely that many were not subject to any monitoring at all. Therefore, study populations are heterogeneous and subject to bias towards lower rates of AF recurrence. Second, by relying on opportunistic diagnosis of AF, these studies are more likely to miss a substantial proportion of asymptomatic or unrecognized AF. Consequently, where the specificity for the diagnosis of recurrent AF is reasonably high, the ability to rule out AF is much more limited. Third, the most sensitive technology that would have been employed in either study would have been a 48-hour Holter monitor – a tool that is less sensitive as compared to the best technologies that are available currently, which includes patch ECG monitors that can be worn for 14 or more days and the implantable loop recorder[99], [100]. It is also important to note that because these studies did not employ a prospective and systematic strategy for monitoring for recurrent AF, they are therefore unable to offer clinicians any guidance on post-discharge rhythm monitoring for patients who manifest AFOTS. Prospective studies with systematic and sensitive screening are required to better define the recurrence rate of AF after AFOTS.
• Clinical guidelines for stroke prevention in patients with atrial fibrillation do not currently take pattern and duration of arrhythmia into account as part of risk stratification. More recent studies show that these factors may be important and further research is required to develop risk stratification schemata that incorporate clinical characteristics and arrhythmia burden.
• Where subclinical atrial fibrillation (SCAF) is associated with a risk of stroke and systemic embolism, the benefit of oral anti-coagulation in this patient group is not established and the results of ongoing clinical trials are awaited to help direct their management.
• Atrial fibrillation is often detected transiently in the setting of an acute, reversible stressor, such as a medical illness or surgery (AFOTS). AF recurs by 5 years in about half of these patients. However; the true rate may be under-estimated, as most studies used relatively insensitive methods to detect recurrent AF. Further studies employing prospective screening strategies that are both systematic and sensitive are required to better define recurrence rates and to guide management with respect to strategies for detection of recurrent AF and/or provision of prophylaxis against stroke.
Dr Healey has received a personnel award from the Heart and Stroke Foundation, Ontario Provincial office (MC7450). Dr McIntyre has received fellowship support from the Canadian Stroke Prevention Intervention Network (C-SPIN) and the McMaster Cooper Award.






