Internal Jugular Vein Complete Thrombosis After Dual Chamber Pacemaker Implant
Angelo Placci, Maria Mattioli, Maria Francesca Notarangelo, Gianluca Gonzi, Marco Zardini
Parma University Hospital, Parma, Italy.
Venous thrombosis after pacemaker implant is a known, although often underrecognized condition that can challenge system revision or upgrading, leading occasionally to thromboembolic complications. Several factors are considered to promote thrombus formation. Among them, alteration of blood flow mechanics due to the presence of catheters in the vessel lumen may itself play a pivotal role. Hereby we present the case of a 65-year old men who underwent a dual-chamber pacemaker implant in another institute for sick sinus syndrome by means of left cephalic venous access. About two months later he started experiencing neck swelling, pain and dysphagia. Six months later, ultrasonography and CT-scan revealed complete jugular vein thrombosis caused by a lead loop at the level of the left subclavian vein. Of note, thrombosis occurred despite proper oral anticoagulation with warfarin undertaken for coexisting atrial fibrillation. It’s important to keep in mind this possible complication of pacemaker implant to allow for early diagnosis and better treatment chances. This case report is an example of how proximal catheter displacement may promote thrombus formation, probably by affecting blood flow mechanics, even in spite of proper oral anticoagulation.
Key Words : Venous Thrombosis, Pacemaker Implantation, Pacemaker Implantation Complications.
Correspondence to: Maria Mattioli, UO Cardiologia, Azienda Ospedaliero-Universitaria di Parma Via Gramsci 14, 43126 – Parma, Italy.
A 65-year old men underwent a dual chamber pacemaker implant (Boston Advantio DR) in another hospital center due to sick sinus syndrome. The atrial and ventricular passive fixation leads were inserted by cut down approach by means of the left cephalic vein. No periprocedural complication was reported, and electric parameters (pacing threshold, impendance, and sensing) were optimal. At discharge, warfarin was started because of persistent atrial fibrillation.
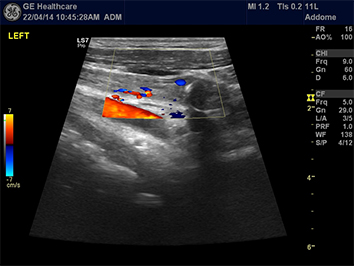
A few months later the patient complained of pain and left latero-cervical neck swelling. Only six months later doppler ultrasonography and CT scan revealed left internal jugular vein (IJV) thrombosis caused by a lead loop occurring at the origin of the left subclavian vein Figure 1, 2. Pacing and sensing parameters were stable. The patient underwent an unsuccessful lead extraction procedure; therefore, a new contralateral implant was performed by means of subclavian vein access. Although taken into account, the hypothesis of a hypercoagulability state was deemed as low due to absence of thrombotic disease at young age both in the patient’s and in his familial history. In the literature, to our knowledge, only a few cases of IJV thrombosis following a permanent pacemaker implant were reported.1-5
Venous thrombosis after pacemaker implant is a known, although underdiagnosed condition that can challenge system revision or upgrading, and poses a threat of possible thromboembolic complications.4 Numerous cases of venous complications due to pacemaker leads have been reported, namely stenosis, occlusions, and superior vena cava syndrome, the catheter itself acting as a nidus for clot formation, as happens for other intravascular devices (e.g. central venous catheters). Available epidemiologic studies show an incidence of pacemaker-related venous complications around 14-38%.6,7 Most cases (97%) are asymptomatic, thus revealing that this condition is broadly underdiagnosed. The clinical spectrum is variable, ranging from asymptomatic forms, usually unmasked during venography at time of system revision upgrading, to lateral neck swelling and pain or, in extreme cases, pulmonary embolism.
Although numerous risk factors were proposed (i.e. number of leads, age of leads, lead material, personal history of previous thrombosis, systemic infetion),5 attempts to define precise risk factors are, to date, inconclusive.
Factors involved in the pathogenesis of upper extremity and internal jugular deep venous thrombosis include hypercoagulable states, but alteration in flow mechanics caused by the presence in the vessel lumen of the lead itself8 is considered to play a pivotal role in thrombus formation. Endothelial dysfunction due to inflammation by continuous lead trauma may further act as a procoagulant factor. Moreover, ligation of the access vein (cephalic vein) can initiate thrombus formation and promote further propagation.
Figure 1: Neck and thoracic contrast tomography showing a lead loop at the origin of the left subclavian vein

This case report enphasizes that it’s important to remind that homolateral pain, dysphagia and lateral neck tumour after a pacemaker implant can suggest internal jugular vein thrombosis, a condition requiring early diagnosis to restore blood flow using antithrombotic drugs to allow better chances of successful lead extraction. In this particular case, since no alteration in routine post-implantation tests were reported, we assumed that the displacement of the pacemaker lead and its subsequent wire loop became a nidus for clot formation and propagation, possibly by promoting blood stasis even in a patient undergoing proper anticoagulant therapy.
Figure 2: Doppler ultrasonography showing internal jugular vein thrombosis