“Two for the Price of One”: A Single-Lead Implantable Cardioverter-Defibrillator System with a Floating Atrial Dipole
Nicole E Worden, MD, Musab Alqasrawi, MD, Siva M Krothapalli, MD, Alexander Mazur, MD
From the Division of Cardiovascular Medicine, University of Iowa Hospitals and Clinics, Iowa City, Iowa.
In patients known to be a high risk for sudden cardiac arrest, implantable cardioverter defibrillators (ICD) are a proven therapy to reduce risk of death. However, in patients without conventional indications for pacing, the optimal strategy for type of device, dual- versus single-chamber, remains debatable. The benefit of prophylactic pacing in this category of patients has never been documented. Although available atrial electrograms in a dual chamber system improve interpretation of stored arrhythmia events, allow monitoring of atrial fibrillation and may potentially reduce the risk of inappropriate shocks by enhancing automated arrhythmia discrimination, the use of dual-chamber ICDs has a number of disadvantages. The addition of an atrial lead adds complexity to implantation and extraction procedures, increases procedural cost and is associated with a higher risk of periprocedural complications. The single lead pacing system with ability to sense atrial signals via floating atrial electrodes (VDD) clinically became available in early 1980’s but did not gain much popularity due to inconsistent atrial sensing and concerns about the potential need for an atrial lead if sinus node fails. Most ICD patients do not have indications for pacing at implantation and subsequent risk of symptomatic bradycardia seems to be low. The concept of atrial sensing via floating electrodes has recently been revitalized in the Biotronik DX ICD system (Biotronik, SE & Co., Berlin, Germany) aiming to provide all of the potential advantages of available atrial electrograms without the risks and incremental cost of an additional atrial lead. Compared to a traditional VDD pacing system, the DX ICD system uses an optimized (15 mm) atrial dipole spacing and improved atrial signal processing to offer more reliable atrial sensing. The initial experience with the DX system indicates that the clinically useful atrial signal amplitude in sinus rhythm remains stable over time. Future studies are needed to determine reliability of atrial sensing during tachyarrhythmias, particularly atrial fibrillation as well as clinical utility and cost-effectiveness of this technology in different populations of patients.
Key Words : Implantable Cardioverter-Defibrillator, Floating Atrial Electrodes, VDD Pacing, DX ICD System.
Correspondence to: Alexander Mazur,,318E GH, 200 Hawkins Dr., Iowa City, IA 52242.
An implantable cardioverter defibrillator (ICD) is a proven life-saving therapy for patients at high risk of sudden death. However, device selection strategy, a single - versus dual-chamber system, in patients without conventional indications for pacing remains debatable. The majority of patients enrolled in the landmark clinical trials that evaluated the utility of ICDs for prevention of sudden death received single-chamber devices.1 The concept of prophylactic pacing in ICD patients without pacing indications has been tested in a number of large randomized clinical trials. In the DAVID (Dual Chamber and VVI Implantable Defibrillator) trail, dual chamber pacing was associated with worse outcomes than VVI back up (40 beats/min) pacing, most likely due to ventricular desynchronization caused by right ventricular (RV) pacing.2 In subsequent trials, dual-chamber programming that minimizes unnecessary RV pacing by using special pacing algorithms (AV Search Hysteresis, Boston Scientific or Managed Ventricular Pacing, Medtronic) or atrial based (AAI 60 beats/min) pacing have yielded no improved outcomes compared to VVI back up pacing.3-5 Yet, about two thirds of patients meeting criteria for a primary prevention ICD are implanted with dual chamber devices in the US; the majority of them have no conventional indications for pacing.6 An ICD system using a single lead with floating atrial dipole, which can provide diagnostic capability of a dual-chamber system without placing an additional atrial lead, has recently become available. In this article we discuss a rationale for its use in ICD candidates who do not require pacing and review initial clinical experience with this system.
Potential Advantages of an Atrial Lead in ICD Patients
Although there is no proven benefit of pacing in ICD patients without traditional pacing indications, recording of atrial electrograms has a number of potential diagnostic and therapeutic advantages. First, the distinction between supraventricular and ventricular arrhythmias using ventricular or far-field electrograms is limited and availability of atrial electrograms improves correct interpretation of stored arrhythmia events triggering ICD therapy.7 Correct diagnosis of arrhythmia treated by ICD is critical for guiding an appropriate therapeutic approach.
Secondly, although published data are mixed, the presence of an atrial
lead can potentially reduce the risk of inappropriate ICD therapies
by enhancing automated arrhythmia discrimination.8-11 While
appropriate device programming with a relatively high detection
cut off rate may significantly reduce the risk of inappropriate ICD
shocks for supraventricular arrhythmias regardless of device selection
(single versus dual), this strategy is not practical in patients with a
relatively slow ventricular tachycardia (VT).10 Inappropriate shocks
predominantly for supraventricular arrhythmias have been reported
in 11.5% - 17.4% of patients enrolled in major ICD clinical trials.12,13 Poorly tolerated high voltage ICD shocks can cause significant
psychological stress and adversely affect patient’s acceptance of the
live-saving ICD therapy. Although the causality remains unclear,
inappropriate ICD shocks have been associated with increased
morbidity and mortality in heart failure patients.12-15
Finally, the presence of an atrial lead allows monitoring of atrial
fibrillation (AF). This aspect of an ICD patient’s management has
become increasingly important with advent of remote monitoring
with automatic wireless data transmission capability that allows
early detection of clinically significant events such as AF, ventricular
arrhythmias or device malfunction.16 It is well recognized that AF
is associated with adverse outcomes in heart failure patients and the
most common trigger of inappropriate ICD shocks.13-15 Asymptomatic AF is commonly found in ICD recipients.10,17 Although there is no consensus on the optimal anticoagulation
strategy in patients with brief asymptomatic episodes of AF detected
by implantable devices, there seem to be no argument that heart
failure patients with sustained forms of AF should be managed with
anticoagulation to reduce the risk of thromboembolic complications.
In addition, early detection and prompt management of sustained
AF by restoration of sinus rhythm or adequate control of ventricular
rate can potentially prevent decompensation of heart failure and
avoid inappropriate ICD shocks.
Disadvantages of the Addition of an Atrial Lead in ICD Patients
The addition of an atrial lead in ICD patients has a number of disadvantages. This adds complexity to implantation and extraction
procedures, prolongs procedure and fluoroscopy time, increases
procedural cost and is associated with higher rate of adverse outcomes.1,6,10,18 An outcome analysis of 104, 049 ICD implantation procedures
using the National Cardiovascular Data ICD Registry found that
selection of a dual- versus a single-chamber device was associated
with increased risk of periprocedural complications and in-hospital
mortality.6 More recent analysis of data from the same registry by
Peterson et al. revealed that the use of a dual-chamber ICD compared
with a single chamber ICD was associated with almost two-fold
higher risk of tamponade and mechanical complications requiring
surgical correction while 1-year hospitalization and mortality rates
were similar.1
A Single-Lead ICD System with Floating Atrial Electrodes
The single lead pacing system that affords atrio-ventricular (AV)
synchrony through floating atrial electrodes (VDD) was introduced
into clinical practice in early 1980’s as a simplified alternative to a
dual chamber pacemaker for patients with complete AV block and
preserved sinus note function.19 While conceptually appealing, VDD
pacing systems are implanted infrequently (< 1% of pacemaker
implants in the US) primarily because of inconsistent atrial sensing
causing intermittent loss of AV synchrony and a concern about
the potential need for upgrade to a dual-chamber device if sinus
node fails.20 However, most ICD patients do not have indications
for pacing at implantation and subsequent risk of symptomatic
bradycardia seems to be low. In the Managed Ventricular Pacing
Versus VVI 40 Pacing Trial, 5.5% of the 1030 enrolled ICD patients
developed an indication for pacing over 2.5 years - some of them due
to AV block.5
The concept of atrial sensing via floating electrodes was
implemented in Biotronik ICDs (Biotronik, SE & Co., Berlin,
Germany) in early 2000’s in hopes to provide all of the potential
advantages of available atrial electrograms without the risks and
incremental cost of an additional atrial lead. The system has since
undergone a series of device and lead modifications to optimize
atrial signal recording and processing (optimization of atrial dipole
spacing and distance from the RV tip, improvement of atrial
signal processing and filtering, implementation of automatic atrial
sensitivity control, adjustment of blanking periods, among others)
prior to its commercial release (Biotronik, personal communication).
The current generation of the system (DX system) consists of a VR-T
DX device and a Linox Smart DX active fixation lead. The Linox
Smart DX lead is a 7.8 French single coil true bipolar lead, which
contains 15 mm spaced pair of atrial ring electrodes mounted 15 -17
cm from the lead tip (Figure 1). Atrial electrodes are floating and
usually not in direct contact with myocardium. The DX ICD system
has no atrial pacing capability but allows optional AV synchronous
VDD pacing. Compared to a traditional VDD pacing system, the
DX ICD system has a number of unique features that offer more
reliable atrial sensing. The optimized atrial dipole spacing covers a
relatively large area of atrial surface of 49 mm2. This provides better
flexibility with its positioning within the atrium and improves stability
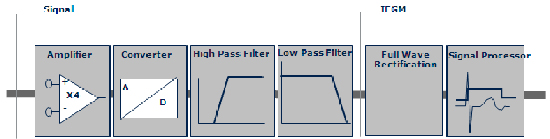
of the atrial signal (Figure 2A). To minimize atrial undersensing, the
DX devices use a pre-amplifier, which progressively increases atrial
gain up to four times. High gained atrial signals are then band-pass
filtered to exclude signal frequencies outside the atrial component
range (30-70 Hz) (Figure 3). While VDD pacemakers use a static
sensitivity setting, the adaptive sensing feature implemented in DX
ICDs helps to prevent oversensing of far-field noise. The DX ICD
system received regulatory approval in Europe in 2011 and in the US
in 2013.
Figure 1 The Biotronik Linox Smart DX active fixation lead. The atrial dipole is mounted 15 -17 cm from the tip of the lead. Courtesy of Biotronik
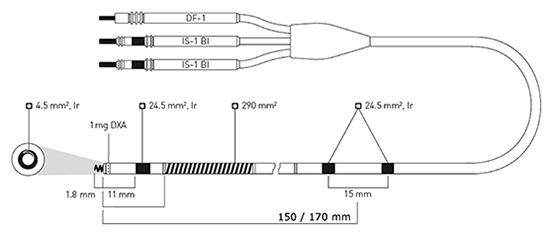
Figure 2A A chest X-ray images showing placement of the Biotronik Linox Smart DX active fixation lead in the apex
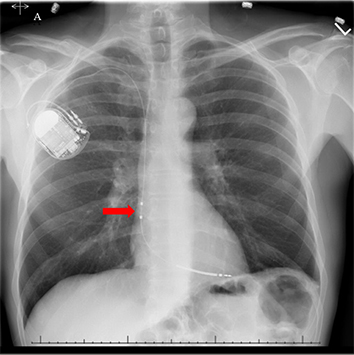
Figure 2B A chest X-ray image showing placement of the Biotronik Linox Smart DX active fixation lead in the septum
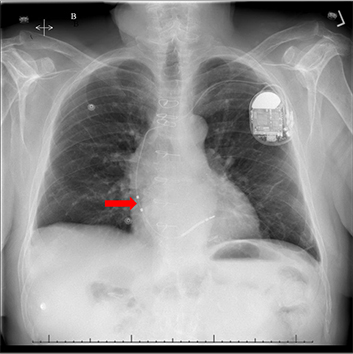
Figure 3 The schematic shows atrial signal processing in the Biotronik DX ICD system, which includes a dedicated atrial input stage with up to 4-fold signal amplification and noise filtering. Courtesy of Biotronik
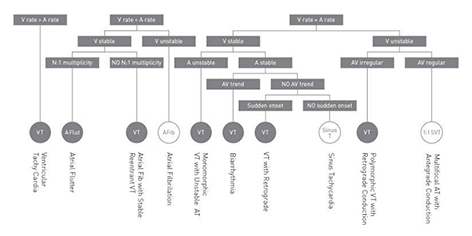
DX ICDs are equipped with the SMART tachycardia
discrimination algorithm, which is based on analysis of the tachycardia
onset, average heart rate, heart rate stability and beat-to beat relation
between atrial and ventricular signals (Figure 4). The algorithm has
been described in details elsewhere.21,22 Previous clinical studies have
shown that the SMART algorithm allows discrimination between
supraventricular and ventricular tachycardias with sensitivity of 100%
and specificity of 64-89%.21,23 In a simulation study, the algorithm
showed 95% specificity for correct detection of supraventricular
tachyarrhythmias.24
Figure 4 Rhythm discrimination criteria employed in the SMART Detection algorithm. A and V denote atrial and ventricular, respectively. Courtesy of Biotronik
Recent studies evaluating the Biotronik DX ICD system have
demonstrated stability of atrial signal within the clinically acceptable
range over time.22,25
In a study of 116 patients implanted with a DX
ICD system, mean P wave amplitude varied from 5.0 to 6.1 mV
during 6-month follow up in different body positions. None of the patients had P-wave amplitude lower then 0.4 mV.
Appropriate atrial sensing was observed in 93.8% of sensing tests with sensitivity setting of 0.4 mV.25 Iori et al. evaluated P-wave
amplitude stability in 13 patients implanted with a DX ICD. The
authors analyzed daily P-wave measurements using the Biotronik
Home MonitoringTM system over a 200-day follow up. Mean
P-wave amplitude was 4.2 ± 1.9 mV, whereas 95% of all daily
measurements varied less than 50% of the mean P-wave value.22
The ADRIA (Belos A+ versus DR Clinical Investigation of
Arrhythmia Discrimination) multicenter study randomized 249
patients without indications for pacing to either a single lead atrial
sensing (A+) system (an early generation of the Biotronik single lead
with floating electrode system which is now called DX ICD) or to a
conventional dual chamber ICD.23 The A+ system was found to
be equivalent to a dual chamber ICD in terms of arrhythmia
discrimination (specificity of supraventricular tachycardia
discrimination: 61.8% and 66.2% for the A+ group and dual chamber
group, respectively) while required significantly shorter implantation
time. The vast majority of the misclassified supraventricular
tachyarrhythmias were relatively slow sinus tachycardia. Low
specificity of the SMART discrimination algorithm found in this
study was attributed to a combination of low programmed VT
detection cut off rate (≤ 130 bpm per study protocol), a relatively
high incidence of abnormal atrial sensing (over- or under sensing)
during supraventricular events, and definition of the Onset criterion
to be triggered by a single ventricular premature beat (once the Onset
criteria is met, the algorithm classifies the rhythm as VT regardless
of other SMART criteria). The Onset criterion has been refined in
later generation of devices (Biotronik, personal communication).
Analysis of 492 misclassified sinus tachycardia episodes revealed
that the percentage of patients with atrial over-or undersensing was
significantly higher in the A+ arm compared to the dual chamber arm
(36% versus 11% of patients, respectively).23 As discussed earlier, the
system has since undergone a series of modifications to optimize atrial
sensing prior to its commercial release. Published clinical experience
with current generation of devices (DX) is limited. In the Linox DX Study, 23 patients had total 88 spontaneous tachyarrhythmia events. All 15
ventricular events were appropriately diagnosed and treated by the
device. In 54 out of 73 (74%) non-ventricular events, ICD therapies
were appropriately withheld. Inappropriately treated events were due
to supraventricular tachycardia (7 events), sinus tachycardia (4 events),
T-wave oversensing (7 events), or electrocautery noise (1 event).25 In
the study by Iori et al., twenty spontaneous tachyarrhythmia events
(3 ventricular and 17 supraventricular) were recorded in the VT zone.
All events were correctly diagnosed by the device.22
In our center, we followed 35 patients who were implanted with
the DX ICD system. We found that the atrial signal amplitude
remained in the clinically useful range (mean 5.4 - 8.7 mV) over
a mean follow up of 432 ± 197 days. There was no difference in
atrial signal amplitude between apical and septal lead positions.
All stored arrhythmia events showed readily interpretable atrial
electrograms (Figure 5A). The majority of the supraventricular events
(82%) were correctly classified by the device and ICD therapies were
appropriately avoided.26
Figure 5A An examples of stored arrhythmia events during supraventricular tachycardia
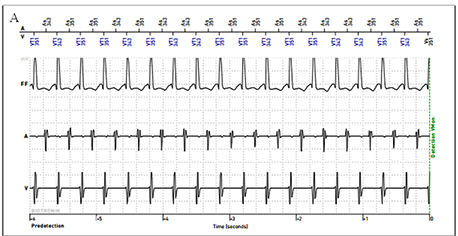
Figure 5B An examples of stored arrhythmia events during ventricular tachycardia
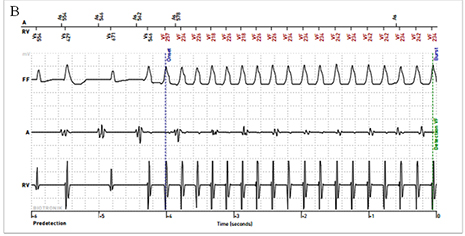
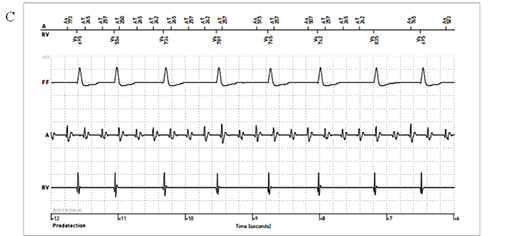
Figure 5C An examples of stored arrhythmia events during atrial flutter
A single lead ICD system with floating atrial dipole, which can
provide the benefit of available atrial electrograms without the risks
and incremental costs of an additional atrial lead, is a promising
alternative to a dual chamber ICD in patients without conventional
pacing indications. The initial experience with the Biotronik DX system
indicates that the clinically useful atrial signal amplitude remains
stable over time. However, since this is a relatively new technology
many questions remain. Future studies are needed to determine:
long-term lead durability
impact of floating electrodes on
complexity of lead extraction comparing to a conventional single coil
ICD lead
reliability of atrial sensing during tachyarrhythmias, particularly atrial fibrillation
subsequent need for atrial pacing
and device upgrades in patients implanted with this system
clinical utility and cost effectiveness of this technology in different patient populations (primary versus secondary prevention indication, primary arrhythmogenic syndromes such as Long QT or Brugada, etc.)
Alexander Mazur, MD - lecture honorarium from Biotronik
Nicole E. Worden, MD - travel grant from Biotronik
Musab Alqasrawi, MD - travel grant from Biotronik
Siva M. Krothapalli - none.






