Shock Lead Dislodgement Related To Its Small Hair-Pin Curve In A Pocket -A Case Of Ratchet Syndrome
Yuka Taguchi, Kohei Matsushita, Toshiyuki Ishikawa, Yutaka Ogino, Hirooki Matsushita, Junya Hosoda, Katsumi Matsumoto, Satoshi Umemura
Department of Cardiology, Yokohama City University Hospital.
There have been few reports about ratchet syndrome. We report a case of ratchet syndrome caused by small hair-pin curve of lead that triggered the lead retract itself. A 69-year-old man with a past history of inferior wall myocardial infarction, presented with progressive congestive heart failure. He underwent implantation of cardiac resynchronization therapy with an implantable cardiac defibrillator (CRTD) at our hospital. At 33 days after implantation, shock lead dislodgement was revealed. X-ray showed that the lead tip was in left subclavian vein, leaving its screw out, and a large part of the proximal portion of the lead was retracted into the pocket, while the other two leads remained in appropriate positions and the device had not rotated. An X-ray series showed that a hair-pin curve had been expanding gradually from just after implantation. In this case, relatively stiff shock lead was markedly bent and expanded the curve in the pocket, and ratchet-like movement occurred. We here report a new type of ratchet syndrome.
Key Words : Dislodgement, CRT, Ventricular, Proximal..
Correspondence to: Yuka Taguchi,The Second Department of Internal Medicine Yokohama City University School of Medicine,Yokohama,Japan.
Lead dislodgement is an unusual complication and a significant dangerous occurrence. Twiddler syndrome and reel syndrome, consisting of lead dislodgement caused by generator rotation on its long axis and transverse axis, respectively, have been previously reported.1-3 Ratchet syndrome is another mechanism of lead retraction, caused by ratchet-like movement of the lead through the suture sleeve.3,4 We here report a case of ratchet syndrome caused by a small hairpin curve of the lead.
Patient was a 69-year-old man. He had inferior wall myocardial infarction in 2000 and progressive congestive heart failure despite appropriate medical therapy. He had New York Heart Association class III heart failure, with ejection fraction of 27%. PQ interval was 281 ms (first degree atrioventricular block) and QRS durations was 131 ms. CRT-D (cardiac resynchronization therapy with an implantable cardiac defibrillator, QUADRA ASSURA, St. Jude Medical, St. Paul, MN, USA ) was performed in October 2014 at our hospital. In this case, extrathoracic puncture technique was used. The lead insert site and the pocket site were separated, and leads were connected to the device through a subcutaneous tunnel. Passive fixation lead Quaretet model 1458-85, SJM was positioned in the lateral cardiac vein for left ventricular pacing. Active fixation lead Optisense model 1999-52, SJM was positioned in the right atrial appendage. Active fixation shock lead Durata model 7122Q-58, SJM was positioned at right ventricular apex. The threshold of the shock lead was 0.5 V, and amplitude was 11.7 mV after the operation. At 24 days after implantation, the patient heard repeated alarms from his chest and had hiccups lasting two days, which suggested phrenic nerve stimulation. When he attended our hospital for routine follow-up at 33 days after implantation, shock lead dislodgement was found. Right ventricular capture failed at maximum output. No ventricular electrogram was detected. Stored telemetry data showed that shock lead noise was increased from 24 days after implantation, which indicated lead detachment from the endocardium.
Chest X-ray showed that the shock lead tip was positioned in left subclavian vein and the proximal portion of the lead was retracted into the pocket. However, the other two leads remained in appropriate positions and the generator was not rotated in the pocket (Fig. 1). Surgical revision was performed 6 weeks after first implantation. The operative findings showed that, the generator was fixed on the fascia, and the atrial lead and left ventricular lead were covered with tissue behind the pocket (Fig. 2); however, the shock lead showed no adhesion to tissue and could be moved in the pocket. Each sleeve was secured by one suture to the original position. However, the shock lead slipped in the sleeve when it was pulled. There was no damage of
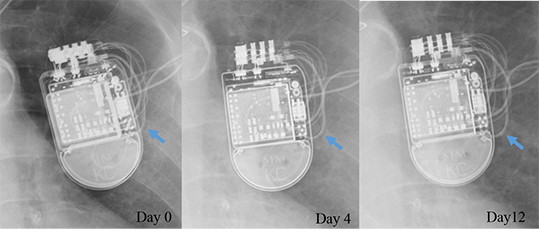
the lead, and it was successfully repositioned at the right ventricular apex. After reoperation, there were no subsequent problems. A small hair-pin curve of the shock lead in the pocket was found in the present case. Differences in the length of each lead caused the small hair-pin curve in the pocket. An X-ray series showed that the hairpin curve had been expanding gradually from just after implantation (Fig. 3).
Figure 1. Chest X-ray showed shock lead dislodgment at 33 days after implantation. The shock lead tip was in the left subclavian vein, while the other leads and pulse generator remained in the original positions
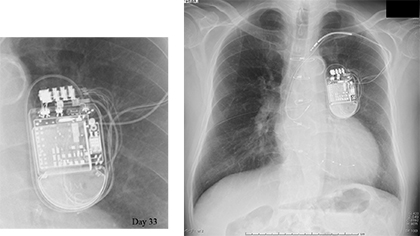
Figure 2. At operation, the generator was fixed on the fascia, and the atrial lead and left ventricular lead were covered with tissue behind the pocket; however, the shock lead showed no adhesion to tissue and could be moved in the pocket (white arrow)

Figure 3. X-ray series showed that a hair-pin curve of the shock lead had been expanding gradually from just after implantation
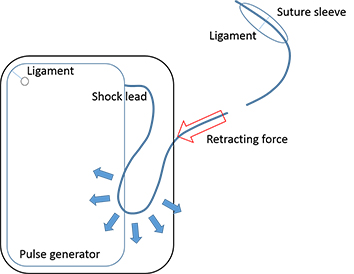
In this case, a large part of the proximal portion of the lead was retracted into the pocket, but the generator was fixed in the pocket and had not rotated. The mechanism in this case is completely different from that of reel syndrome and twiddler syndrome. Ratchet syndrome is due to ratchet-like movement of the lead in the sleeve. When ligation of the suture sleeve is insufficient, the pendula-like movement of the generator due to movement of the arm may cause ratchet syndrome.4-6 The relatively stiff shock lead was markedly bent and could expand the hair-pin curve in the pocket (Fig. 4). It cannot
be denied the possibility that the hair-pin curve became a trigger to
pull the lead. Once ratchet-like movement occurred in the suture
sleeve due to the hair-pin curve, the lead could slide into the pocket
repeatedly. In order to avoid ratchet syndrome, it is important not
only to ligate the suture sleeve firmly, but also to avoid such a small
hair-pin curve. As the DF4 lead is very stiff around the connecter,
it may easily induce pendulum-like movement. As the atrial and
left ventricular leads were strongly fixed behind the pocket, ratchet
syndrome could not occur in these leads. This in a case of ratchet
syndrome, not reel syndrome. We considered the other cause is the
material of the lead. In previously reported cases, the material of the
dislodged leads was polyurethane or silicon-polyurethane copolymer.4,7,8 Our present case also had a polyurethane lead. Polyurethane
has a surface lubricity and a low coefficient of friction compared to
silicon. The less friction between the lead and the sleeve, the more
slippery inside the sleeve.
Figure 4. The relatively stiff shock lead was markedly bent and expanded the curve in the pocket, and consequently pulled the lead into the pocket, which caused ratchet-like movement in the suture sleeve, and the lead could slide into the pocket repeatedly
A small hair-pin curve may be one of the causes of ratchet
syndrome.






