Idiopathic VPC: Distribution Of FOCI And Tips Of Ablation
Jose C Pachon M, MD, PhD1,2,3, Tasso J Lobo, MD3, Enrique I Pachon M, MD1,3, Tomas G Santillana P, MD3, Carlos TC Pachon, MD3, Juan C Pachon M, MD1,2,3, Remy N Albornoz V, MD1,3, Juan C Zerpa A, MD3, Felipe A Ortencio, MD.3
1Sao Paulo State Cardiology Institute.2Sao Paulo University.3Sao Paulo Heart Hospital.
Idiopathic Ventricular Premature Contraction (VPC) is currently more routinely referred for electrophysiology evaluation. Usually it carries a good prognosis but, when symptomatic or suspected to produce ventricular dysfunction, will require treatment. Nowadays, RF ablation has great advantages over antiarrhythmic drugs. Classically the outflow tract (right or left), with the typical inferior axis with left (eventually right) bundle brunch block like ECG morphology, is considered the most frequent site of origin for idiopathic VPC, but with the widespread of EP procedures and advancement of technology making possible to map and ablate difficult locations, it is possible to see a growing and changing population referred for idiopathic VPC ablation, displaying that, almost any region of the heart may be source of this kind of arrhythmia that can be successfully treated. A well-planned procedure, with the presumed region of origin settled and employing the current technology and knowledge (tips), will have a high chance of cure.
Key Words : Idiopathic, Ventricular Premature Contraction, Ablation, Outflow tract.
Correspondence to: JC Pachon,Sao Paulo,Brazil.
Ventricular premature contraction (VPC) in a apparently healthy young adult with no previous history is not so uncommon, and may cause emotional stress until the accurate diagnosis is done. Described as “idiopathic ventricular arrhythmia”, it is defined as the arrhythmia not related with any detectable structural cardiac disease. It accounts for about 20% of all patients referred for evaluation of ventricular arrhythmias. Most patients are symptomatic and will need treatment; other are asymptomatic but have a high burden of the arrhythmia and may be at risk of developing a reversible form of left ventricular dysfunction (tachycardia-induced dilated cardiomyopathy)1 and will need treatment as well.2 Pharmacologic treatment of these arrhythmias, usually with beta-blockers, calcium channel blockers and even amiodarone, has only modest efficacy (around 25 to 50%). Most young patients do not desire long-term medical therapy or are not drug tolerant. Some patients can even feel a worsening of symptoms after medications due to drug induced bradycardia or to an increase in VPC burden. Considering that usually the source of the arrhythmia is unifocal, ablation has undoubtedly some advantages over medical treatment, since it has a high chance of cure.3 Therefore, broadly speaking, the key decision is if the patient needs or not treatment, if so, the best option is usually the RF ablation.
Ventricular premature contraction in structural normal heart may arise from any region but the outflow tract VPC / VT is the most common form, known almost as synonymous of idiopathic ventricular arrhythmia; one concern, is to differentiate from initial form of arrhythmogenic right ventricular cardiomyopathy/dysplasia. The reason these arrhythmias come most frequently from outflow is still not clear. The typical electrocardiogram features is the inferior axis and left branch block morphology. For a long time it has been taught that the right ventricular outflow tract (RVOT) accounts for the majority (about 80%) of idiopathic VPCs, however, taken into account the great growing of referred population, the foci location has changed significantly in the last decade. Maybe due to the ability of mapping complex or difficult structures and the widespread of ablation procedures, the kind of patient that is referred for electrophysiology evaluation nowadays has been show a shift to other regions, outside of RVOT. Recently Penela et al.4 studied 117 patients with outflow tract arrhythmias and found almost the same distribution of foci from left and right side (left: 51%; Right: 49%). A newly and big study from Latchamsetty et al.5give a compelling evidence for distribution of foci in current VPC ablations based on 8 international centers, comprising 1,185 patients between 2004 and 2013. They found and described the origin as follow: RVOT: 45%; Aortic Cusps: 15%; Papillary Muscles: 5%; Epicardium: 11%; Other (not specified) origin: 24%. Therefore any area of the heart may be source of idiopathic ectopy.
Outflow Tract is still the most common site and is classified
as one group apart. This area include the following structures:
right ventricular outflow tract (RVOT), left ventricular outflow
tract (LVOT), the aortic sinuses of Valsalva, the area of aortomitral
continuity, the superior basal septum near the His bundle, the
pulmonary artery, and the epicardial surface of the outflow tracts.
Although some clinical differences4 may exist, these arrhythmias
have similar characteristics and share the same behavior. Actually
the right and left ventricular outflow tracts are in close relationship
and this explains the difficult of differentiating them by
ECG criterion and the phenomenon of shifting, when 2 discrete
morphologies are seeing changing during the catheter ablation.
Tricuspid Annulus was the source of origin of 8% of idiopathic
VPC/VT as described by Tada et al.;6 they show that the majority
(74%) of them originated from the septum portion. Yamada
et al7 presented a case report where they did ablation of
tricuspid annulus VPC using a halo-type catheter to help mapping.
Mitral annulus ventricular arrhythmias have been described
as 5% of idiopathic arrhythmias in a large series;8 the authors
showed that in all patients an S-wave was present in lead V6.
Pappilary Muscles has a rich network of Purkinje fibers, 9 these structures
are accountable for 4,2% of idiopathic VT/PVC in one series;10
they may arise in normal hearts but, when compared with fascicular
and mitral annular PVC, it seems that these arrhythmias occur in older
patients and are often related with the presence of coronary artery
disease and left ventricular dysfunction;11 they also showed that papillary
ectopy has a wider QRS duration than fascicular arrhythmias.
The Fascicles of the left bundle branch are classically knowing as
source of a typical idiopathic VT, but it may arise ectopy as well; it is
ready identified by a narrow QRS and the characteristic ECG morphology
of the fascicle of origin: left posterior fascicle with a right
bundle branch block and left axis deviation; left anterior fascicle with
morphology of right bundle branch block and right axis deviation; high
septal fascicle with relatively narrow QRS complex and normal axis.
Epicardial and/or Peri-Vascular are other source of idiopathic
ectopy. 12 Scanavacca et al suggest that these arrhythmias may
be accessed by the venous system or by subxiphoid epicardial
mapping, but do not recommend an epicardial approach on
the first procedure for outflow tract arrhythmias;13 one concern
is the presence of the coronary arteries and phrenic nerves. A delay
in the initial time of the QRS complex indicated a epicardial
origin as suggest by the Maximum Deflection Index (MDI). 14
One important aspect in counseling patients with idiopathic
arrhythmias, essentially outflow tract, is the challenge of predicting
the site of origin, therefore discussion about treatments
options and intervention planning. There are several ECG criteria
that try to locate the focus (Figure 1), some of them are based
on complex process analysis or formulas. The inspection of QRS
morphology of the VPC compared with the normal sinus rhythm
(“the V2 transition ratio”)15 is practical and helpful, Figure 2.
Figure 1 Scheme of the main ECG morphologies of the basal PVCs. There is a progressive modification of the QRS from negative to positive in lead V1 according the origin of the PVC from the anterior RVOT to the epicardium of the posterior left ventricle.
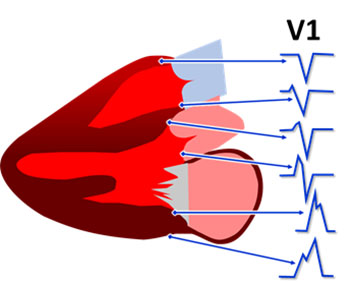
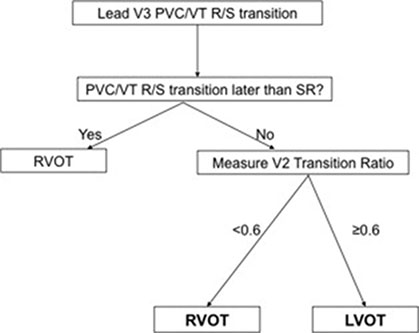
Figure 2 Algorithm developed by Betensky BP et al.15 for OTA ECG localization. If the PVC transition to an R>S occurs later than the SR transition then the PVC origin is the RVOT (100% specificity). If the PVC transition occurs at or earlier than the SR transition (i.e., SR transition lead V3 or later), then the V2 transition ratio is measured. If the transition ratio is <0.6, then RVOT origin is likely. If the transition ratio is ≥0.6, then LVOT origin is likely (sensitivity 95%, specificity 100%).
Beyond morphologic criteria, others ECG characteristics and clinical
aspects may be valuable in arrhythmia discrimination. Recently
Bradfield et al.16 demonstrated that arrhythmias that arise from sinus
of Valsalva and great cardiac vein have a highly variable coupling
interval with the preceding normal QRS, probably due to a lack of
electronic coupling with the surrounding myocardial. PVC originated
from RV or LV myocardial have a relative fixe coupling interval
compare with PVC from sinus of Valsalva and great cardiac vein; a
pronounced variability in couple interval (Delta > 60ms) helps discriminate
the origin of PVC. Another interesting study from Penela
et al.4 evaluated clinical characteristics in patients with outflow tract
arrhythmias; they showed that the presence of hypertension, male
gender and age > 50 years were independent predictive of LV outflow
tract origin and a score with these three variables was proposed.
Different from reentry ventricular tachycardias, which can be usually
reproduced with programmed ventricular stimulation techniques,
ventricular premature beats has the disadvantage of being less easily
reproduced. All antiarrhythmic medications should be discontinued
for at least five half-lives before the ablation. Not uncommonly, even
in patients with very frequent clinical arrhythmia, it may be necessary
to perform the procedure in the absence of ectopic beats. It is
helpful to see in the Holter if the arrhythmia is more frequent during
the sleep or vigil. In the last case a deep sedation must be avoided.
One of the key point of ablation of idiopathic VPC is to have the
arrhythmia (spontaneously) in the moment of the procedure or to
identify a protocol that induce the arrhythmia; It is really important
for mapping and for having an end point during the procedure. There is
no unique maneuver or protocol that works satisfactorily for ever case.
Despite being unpredictable, it is usually possible to trigger the
ectopies appearance, so we always try to perform the procedure
on the day that the patient was scheduled, but many researchers
suspend the procedure if there is no spontaneous arrhythmia.
At the beginning, in the case there are no arrhythmias, with the patient
fully monitored and awaked, some ventilation maneuvers (depth
breath or Valsalva) may provoke VPC allowing to get recordings (that
must be saved) for pace mapping. After sedation, ventilation changes
induced by the anesthesiologist, like short hypoxia periods, may also
reproduce the arrhythmia. After placing the catheters, there is a good
chance that some atrial or ventricular stimulation protocols with different
cycle length or extra-stimuli, may reproduce the arrhythmia
during the stimulation or after stopping, during the pause. Ventricular
stimulation must be attempted with programmed stimulation
or burst. Some people try isoproterenol (despite epinephrine seems
to be better), but in our experience it may be trick; some times with
the sinus rate increasing it may eliminate any sporadic ectopy that
could be present; also, with the vigorous myocardial contraction due
to isoproterenol, the manipulation of the catheter (and pace mapping)
is more difficult or even risky. It seems that isoproterenol works
better when it is given as small bolus than continuously (progressive),
because there is a better chance that the arrhythmia is induced after
the peak effect of the drug, when the sinus rate is slowing down.
Another very interesting issue is autonomic stimulation to promote
cardiac reflex for triggering some arrhythmias.
17,18
This can be
important to achieve the morphology in 12 lead ECG of a PVC
that eventually becomes completely absent at the time of the procedure
in order to proceed with the pace mapping. We are studying
the potentiality of vagal stimulation performed by placing a catheter
inside the internal jugular, up to the superior wisdom tooth
level by using even the RF catheter temporarily detached from
the RF generator and connected to a neurostimulator, Figure 3.
In this place, it is usually easy to get an intense vagal stimulation
that causes transient asystole, Figure 4-A. Soon after the vagal
effect, a reflex sympathetic response occurs usually causing
the appearance of PVC, Figure 4-B. Depending on the case, that
may be better than the isoproterenol infusion because it triggers
the sympathetic response by natural paths. Paradoxically, by causing
an important heart rate increase, the isoproterenol may prevent
the PVC appearance just because of the diastolic extent reduction.
Figure 3 Scheme of the methodology for vagal stimulation during EP studies developed by authors. The RF catheter, temporarily detached from the RF generator and connected to a neurostimulator, is advanced to the internal jugular vein. This position usually has a great proximity with the vagus nerve allowing its stimulation. This maneuver must be only accomplished after being the patient anesthetized.
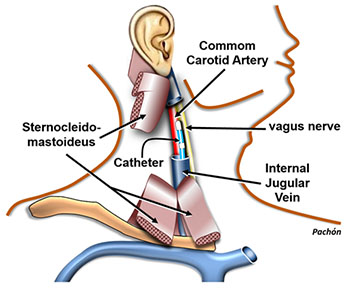
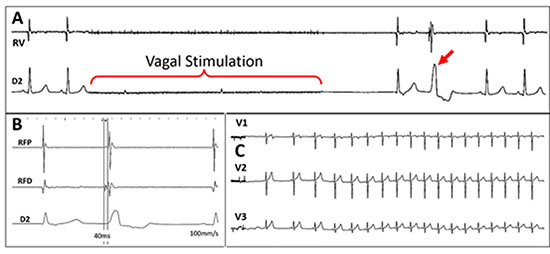
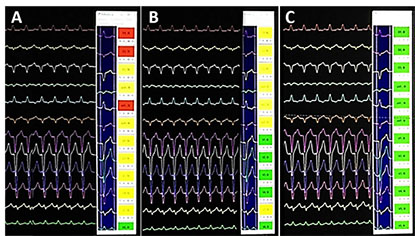
Figure 4 Case of a patient who was symptomatic due to a very frequent monomorphic VPC. However, in the EP laboratory the arrhythmia was completely absent. A: during vagal stimulation there is an immediate asystole followed by a junctional beat and one PVC (red arrow). This response was typically reproducible. All other attempts to reproduce the PVC were unsuccessful. B: The PVC triggered by the vagal stimulation was mapped and a good precocity was obtained allowing the ablation; C: After ablation, vagal stimulations were unable to reinduce new VPCs. Currently, this patient is asymptomatic and has no more arrhythmia.
It is a great aid technique pacing point-to-point areas suspected
from the ECG PVC morphology. The main objective is to reproduce
the morphology of spontaneous PVC in 12-lead ECG through electrical
stimulation of a certain point. This step can be accomplished
by direct subjective comparison of the operator or aided with automated
computerized systems, Figure 5. A major advantage of this
method is that it can be performed in the absence of the arrhythmia
since the PVC morphology in a 12-lead ECG technically identical
to the ablation ECG, can be compared. An important drawback
is that the pace mapping identifies the starting point of the PVC
appearance in the myocardium and not necessarily the actual focal
origin.19 Despite being not totally necessary, the use of three-dimensional
electroanatomical mapping system and, recently, the rotational
angiography may be of great value for mapping assistance.20
Figure 5 Computerized aid for pace mapping. Pace mapping is extremely useful in the PVC ablation however, it has some disadvantages like the time consuming and a huge dependency of the subjective interpretation of the operator. This software, developed by the authors, as other products on the market, has promoted great agility and efficiency in the pace mapping technique. In A and B there are two examples of pace mapping inappropriate for ablation, however in C the mapping is excellent that is, a place with a high probability of ablation success (all the flags are green).
Computer Aided Pace Mapping
Other area of great interest is to improve the performance and the
quality of the pace mapping technique, making it faster and less de-
pendent of the interpretation of the operator. Considering that sometimes
we do not have the PVC frequency as desired, pace mapping is
the main approach being the technique that allows getting close of the
site of origin and save time. There are some reports dealing with automatic
template for computerized interpretation of pace mapping.21
Ablation of Valsalva Sinus PVCs
A very delicate situation is when PVC is located in the sinus of
Valsalva because of the risk of coronary lesion. Only the non-coronary
sinus does not originate PVCs as it relates only with the fibrous
skeleton of the heart. That means, whenever there are PVCs of this location
they are surely originated from the left or right coronary sinus,
whose ablations should deal with the risk of coronary injury, Figure 6.
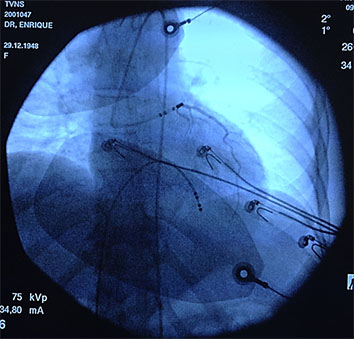
One fundamental tip for ablation in the right or left Valsalva coronary
sinus is to perform the coronariography immediately before
the RF release. A simple and practical way we have proposed is to
place the contrast dye in the irrigation system of the ablation catheter.
After positioning the RF catheter in the most appropriate mapping
place, radiographic contrast product is directly injected through
the irrigation system. This should be repeated immediately before
each new ablation case the catheter position has been changed.
If the contrast shows that we are far from coronary ostium we can
ablate without risk. Conversely, if it is found that we are very close
to the coronary ostium the ablation must be suspended (Figure 7).
Figure 6 Scheme of the cardiac fibrous skeleton and its relationship with Valsalva sinuses. The non-coronary sinus is related with fibrous tissue only and is the solely one that does not gives rise to PVCs. The coronary sinuses are relatively frequent source of PVCs and the ablation in these places must have special care for avoiding coronary injury.
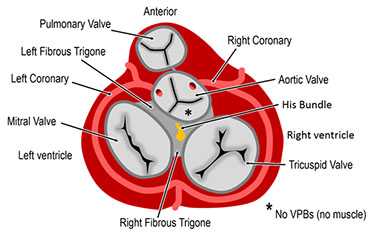
Figure 7 Forbidden PVC ablation. Method proposed and routinely employed by the authors using the irrigation system of the ablation catheter, placed in the best mapping position, by injecting X-ray dye for verifying if it is in a risk position, associated with a coronary ostium. In this example, a young woman had a ventricular tachycardia originated from the left coronary sinus. The best place for ablation was located in the left coronary ostium. The ablation catheter was relocated and the ablation was finally successful but performed outside the ostium, despite being a suboptimal position.
It can be performed directly with the RF catheter or through the
electroanatomic mapping system. It is certainly the key element to
the success of ablation. Generally, the potential that indicate the
position of the arrhythmogenic focus with great chance of success
precede the QRS surface of the PVC onset in 10 to 60ms,22 Figure
4-B. The morphology of these potentials is also of great value
especially the QS pattern in unipolar recording of the distal pole23
or the reverse potentials comparing two distal dipoles of the ablation
catheter.24 When myocardium mapping is not quite appropriate in
the myocardial the outflow tracts myocardium it is essential to make
an inspection on arterial insertions, above the pulmonary and aortic
valves,25,16
as well on the mitral annulus,8 as these places are often the
real origin of these arrhythmias, Figure 1.






